Type 1 autoimmune hepatitis in a patient with microscopic
Anuncio

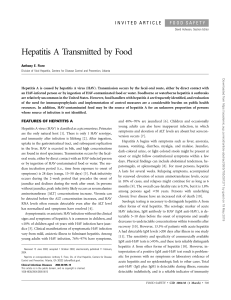
Documento descargado de http://www.elsevier.es el 16/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Med Clin (Barc). 2011;136(8):345–348 www.elsevier.es/medicinaclinica Clinical report Type 1 autoimmune hepatitis in a patient with microscopic polyangiitis: challenges in diagnosis and treatment Sergio Prieto-González a,b, Francesc Cardellach b, Ramon Estruch b, Rosa Miquel c, Josep M. Grau b, Maria Cinta Cid a,* a Vasculitis Research Unit, Department of Systemic Autoimmune Diseases, Hospital Clı´nic, University of Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Catalonia, Spain Department of Internal Medicine, Hospital Clı´nic, University of Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Catalonia, Spain c Department of Pathology, Hospital Clı´nic, Barcelona, Catalonia, Spain b ARTICLE INFO A B S T R A C T Article history: Received 8 October 2010 Accepted 14 October 2010 Available online 4 February 2011 Background and objective: Autoimmune diseases/autoantibodies tend sometimes to cumulate in the same individual, probably as a consequence of defects in immune regulation with breakdown of selftolerance. Autoimmune hepatitis and microscopic polyangiitis have been occasionally reported with other autoimmune diseases, but the particular association of these both disorders has not been previously reported in the English and Spanish medical literature. Case report: A 72 year-old woman presented with symptoms suggesting giant cell arteritis and polymyalgia rheumatica. Results: A temporal artery biopsy disclosed a spared temporal artery, with vasculitis involving surrounding small vessels. Anti-neutrophil cytoplasmic antibodies were positive, with myeloperoxidase specificity. Increased liver enzymes led to a wider autoantibody determination. Anti-nuclear antibodies and anti-smooth muscle cell antibodies with anti-f-actin specificity were also positive. A liver biopsy showed changes consistent with autoimmune hepatitis. Conclusions: Clues for the diagnosis of vasculitis and AIH in the context of this patient, challenges in its classification among systemic vasculitides, and difficulties in the choice of a suitable therapeutic management for this particular association are discussed. ß 2010 Elsevier España, S.L. All rights reserved. Keywords: Microscopic polyangiitis Autoimmune hepatitis Giant-cell arteritis Classification criteria Immunosuppressive therapy Hepatitis autoinmune tipo 1 en una paciente con poliangiı́tis microcópica: desafı́os en el diagnóstico y tratamiento R E S U M E N Palabras clave: Poliangiı́tis microscópica Hepatitis autoinmune Arteritis de células gigantes Criterios de clasificación Tratamiento inmunosupresor Fundamento y objetivo: Las enfermedades autoinmunes/autoanticuerpos en ocasiones tienden a presentarse en un mismo individuo, probablemente por defectos en la regulación inmune con pérdida de la autotolerancia. La hepatitis autoinmune y la poliangiı́tis microscópica se han descrito ocasionalmente asociadas a otras enfermedades autoinmunes, si bien la asociación particular de ambas entidades no se ha descrito previamente en literatura médica inglesa o castellana. Observación clı´nica: Mujer de 72 años que ingresó con sı́ntomas sugestivos de arteritis de células gigantes y polimialgia reumática. Resultados: Una biopsia de arteria temporal mostró una arteria indemne con presencia de vasculitis en vasos de pequeño tamaño a su alrededor. Una biopsia muscular confirmó la existencia de una vasculitis sistémica de pequeño vaso. Los anticuerpos anticitoplasma de neutrófilo fueron positivos, con especificidad antimieloperoxidasa. Dada la presencia de elevación de las enzimas hepáticas y anticuerpos antinucleares con especificidad anti-actina, se realizó una biopsia hepática que mostró cambios compatibles con una hepatitis autoinmune. * Corresponding author. E-mail address: mccid@clinic.ub.es (M. Cinta Cid). 0025-7753/$ – see front matter ß 2010 Elsevier España, S.L. All rights reserved. doi:10.1016/j.medcli.2010.10.015 Documento descargado de http://www.elsevier.es el 16/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. S. Prieto-González et al / Med Clin (Barc). 2011;136(8):345–348 346 Conclusión: En el contexto de esta asociación insólita de enfermedades se discuten las claves del diagnóstico, la dificultad en la clasificación dentro de las vasculitis sistémicas y la elección del tratamiento más adecuado para la paciente. ß 2010 Elsevier España, S.L. Todos los derechos reservados. Introduction Microscopic polyangiitis (MPA) is a systemic, non granulomatous, necrotizing vasculitis preferentially involving small vessels1,2. It is frequently associated with the presence of antineutrophil cytoplasmic antibodies (ANCA) with anti-myeloperoxidase (MPO) specificity1,2. MPA may be associated with other conditions including interstitial lung disease and anti-glomerular basement membrane glomerulonephritis. Association with other autoimmune diseases, such as Sjögren’s syndrome, primary biliary cirrhosis, systemic sclerosis, and mixed connective tissue disease, has been sporadically reported3,4. Autoimmune hepatitis (AIH) is a chronic inflammatory liver disease predominantly affecting women of all ages. AIH shows a highly variable, clinical presentation, ranging from asymptomatic to fulminant5,6. The autoantibody pattern, along with clinical and epidemiologic findings, defines 2 types of AIH. Type I AIH is characterized by the presence of anti-smooth muscle cell antibodies, particularly with anti-f-actin specificity and/or antinuclear antibodies, and type AIH II by the presence of anti liver and kidney microsomal antibodies (LKM) or anti-liver cytosol (LC) I antibodies5,6. AIH is frequently associated with other autoimmune diseases, particularly thyroiditis, ulcerative colitis, celiac disease, type I diabetes, systemic lupus erythematosus, and rheumatoid arthritis5,6. We describe a patient who was simultaneously diagnosed with MPA and type I AIH. This association has not been previously reported in the English or Spanish medical literature. Besides raising awareness of this potential association and its clinical consequences, this report addresses additional educative purposes such as the diagnostic process of vasculitis and autoimmune hepatitis in this clinical context, challenges in its classification among systemic vasculitides, and difficulties in the choice of a suitable immunosuppressive agent for this specific association on the basis of current evidence-based recommendations. Case report A 72-year-old woman presented with a 3 month-history of asthenia, malaise, 5-kilogram weight loss, frontal headache, scapular girdle weakness and arthralgia in knees, elbows, and wrists. Generalized weakness was apparent at physical examination. Muscle strength was 3/5 in the upper girdle and 4/5 in the lower limbs. Osteomuscular reflexes and sensitivity examination were normal. Temporal arteries were not enlarged or tender and had a preserved pulse. No signs of inflammation were observed in the affected joints. Routine laboratory findings are depicted in table 1 table 1. Increased acute-phase reactants and liver enzymes, with both Table 1 Laboratory findings at baseline evaluation and after a follow-up period of 27 months. Baseline 27 months Reference values C Reactive Protein ESR Creatinine Urea nitrogen Aspartate aminotransferase (AST) Alanine aminotransferase (ALT) Gamma-glutamyltransferase (GGT) Alkaline phosphatase (AP) Total bilirubin Albumin Haemoglobin Platelet count WBC Gamma-globulin HBsAc HBcAb HCVAb 4.5 mg/dL 74 mm/hour 1.2 mg/dL 33 mg/dL 188 U/L 125 U/L 244 U/L 328 U/L 1.2 mg/dL 27 U/L 131 g/L 275 x 109/L 8.8 x 109/L 41 g/L Negative Negative Negative 0.04 mg/dL 7 mm/hour 0.90 mg/dL 23 U/L 18 U/L 14 U/L 135 U/L 1.2 mg/dL 148 g/L 249 x 109/L 8.16 x 109/L - (0.001-0.90) (1-20) (0.30-1.30) (10-25) (5-40) (5-40) (5-40) (90-290) (0.2-1.2) (37-53) (120-170) (130-400) (4-11) (9-17.5) Antineutrophil cytoplasmic antibodies (ANCA) ANCA specificiy PR3 MPO Positive perinuclear Negative 0 U/mL 54 U/mL 0 U/mL 43 U/mL Other ANCA specificitiesa Negative - Antinuclear antibodies (ANA) Anti-DNA antibodies Anti-Crithidia lucilliae Anti-smooth muscle antibodies (ASMA) Anti-actin antibodies (AAA) Anti-soluble liver antigen/liver pancreas antibodies (anti-SLA/LP) Anti-liver-kidney microsomal-1 antibodies Anti-liver cytosol antibody-1 Rheumatoid factor Prothrombin time 640 URF 26 U/mL Negative 1/160 Positive Negative Negative Negative 913 16%c 113 URF 36 mUI/mL Negative Negative 403 - a b c Tested antibodies directed against: cathepsin G, lactoferrin, lysozym, bactericidal permeability inhibitor and elastase. Normal reference values. Receiving acenocumarol for chronic atrial fibrillation.. < 25b < 25b < 10b < 25b (80-100) Documento descargado de http://www.elsevier.es el 16/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. S. Prieto-González et al / Med Clin (Barc). 2011;136(8):345–348 cytolysis and cholestasis, were the only abnormalities. A chest Xray showed no abnormalities and an abdominal ultrasound disclosed a liver normal in size and structure. Since one of the patient’s major complaints was headache, she was older than 50 years, had arthralgia and proximal weakness suggestive of polymyalgia rheumatica (PMR), and elevated acute phase reactants, giant-cell arteritis (GCA) was considered and a temporal artery biopsy was performed. Histopathologic examination showed mild mononuclear cell inflammation of a mediumsize artery in the vicinity of a spared temporal artery (fig. 1A). A systemic vasculitis other than GCA was deemed and the patient was re-evaluated. An electromyographic examination showed no muscle or peripheral nerve abnormalities and a blind muscle biopsy confirmed vasculitis involving small and medium-sized vessels (fig. 1B). Immunologic studies are displayed in table 1. ANCA were positive at immunofluorescence examination. AntiMPO specificity was confirmed by enzyme-linked immunoassay (ELISA). The increase in liver enzymes led to a wider autoantibody screening and anti-smooth muscle cell antibodies were positive with anti-actin pattern and anti-f-actin specificity. Antinuclear antibodies, anti-dsDNA and rheumatoid factor were also positive. The abnormal liver tests and autoantibody profile led to the performance of a liver biopsy which was consistent with AIH (fig. 1C and 1D). Combining clinical, analytical, immunologic and histopathologic data she reached a definite diagnosis of AIH, [()TD$FIG] 347 according to the International Autoimmune Hepatitis Group criteria and a recently simplified version7. The patient was treated with prednisone (60 mg/day) and azathioprine (100 mg/day) for one month with subsequent prednisone tapering. She quickly achieved clinical remission and the liver enzymes completely normalized 6 weeks after the beginning of treatment. Twenty-seven months after diagnosis the patient remains asymptomatic under azathioprine 100 mg/day and prednisone 2.5 mg/day. Discussion The patient reported had a biopsy-proven diagnosis of systemic vasculitis that could be classified as MPA on the basis of the size of involved vessels and positive pANCA with anti-MPO specificity2. She also had a definite diagnosis of AIH according to the International Autoimmune Hepatitis Group-scoring system and a recently revised version7. This patient illustrates how autoimmune diseases/autoantibodies tend sometimes to cumulate in the same individuals, probably as a consequence of defects in immune regulation with breakdown of self-tolerance. However, this particular association is unusual and this is the first case published in the English or Spanish medical literature. Two possible additional cases have been reported in Japanese journals8,9. A B C D Figure 1. A: Vasculitis involving small arteries in the scalp. Temporal artery biopsy disclosing a normal temporal artery and an inflamed and occluded small sized artery in the vicinity (hematoxylin and eosin staining). A higher magnification of the involved artery (inset) shows infiltration of the artery wall by a mixed inflammatory infiltrate. B: Vasculitis involving small arteries in skeletal muscle. Vasculitis involving a small sized artery in a muscle biopsy (trichromic acid staining). In both specimens, inflammatory infiltrates are predominantly mononuclear and no fibrinoid necrosis can be observed, possibly indicating chronicity. C: Chronic hepatitis. Liver biopsy disclosing slight periportal necrosis and moderate-intense inflammatory infiltrates with predominance of lymphocytes. Plasma cells (x100 magnification inset) and scarce eosinophils can also be seen. Mild erosive periportal and portal necrosis, mild sinusoid inflammation and hepatocellular necrosis are also observed (hematoxylin and eosin staining). D: Chronic hepatitis. Trichromic acid staining shows porto-septal fibrosis and incipient nodular formation (x10). Documento descargado de http://www.elsevier.es el 16/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 348 S. Prieto-González et al / Med Clin (Barc). 2011;136(8):345–348 The diagnosis and classification of vasculitis in this patient was not easy. Interestingly, our patient presented with symptoms suggestive of GCA and fulfilled 4 ACR classification criteria: age older than 50 years, new headache, elevated ESR and an abnormal temporal artery biopsy disclosing mononuclear cell inflammation10. In addition, although she lacked some typical PMR symptoms such as proximal stiffness, she had generalized arthralgia and proximal muscle weakness, which may have suggested PMR. However, the temporal artery itself was not involved and inflammatory infiltrates were restricted to a smallsized artery nearby. Involvement of small/medium-sized vessels surrounding a spared temporal artery may be an incomplete picture of GCA but may also occur in systemic necrotizing vasculitis11. Consequently, patients with inflammation of vessels surrounding a spared temporal artery should be subjected to an extensive evaluation to rule out systemic necrotizing vasculitis, even fulfilling ACR criteria for GCA11. Clearly illustrating this concept, this patient was classified as having MPA on the basis of the size of affected vessels, widespread involvement beyond small cranial arteries, lack of granulomatous inflammation, and ANCAMPO positivity2. Elevation of alkaline-phosphatase can be observed in 30-50% of patients with GCA or other systemic vasculitis12. However, with the exception of hepatitis B-related polyarteritis nodosa or hepatitis B or C-associated cryoglobulinemia, cytolisis is highly uncommon in systemic vasculitis. Elevated transaminases were an important clue for the diagnosis of AIH in our patient, leading to an extension of the immunologic study. Interestingly, 40-96% of patients with AIH have positive ANCA5,6. However, in AIH, ANCA exhibit an atypical perinuclear pattern, and specificities are highly variable including lactoferrin, cathepsin G, a-enolase, and bactericidal/permeability increasing protein, among others5,6. Our patient’s ANCA had a typical perinuclear pattern and confirmed specificity against MPO. Other specificities were excluded by ELISA (table 1). The importance of recognizing the presence of AIH in the context of MPA has prognostic and therapeutic implications. Although both diseases are responsive to immunosuppressive therapy, the treatment choice needs to be adapted to their coexistence. Moreover, since AIH is a recurrent and chronic disease, an inadequate monitoring of hepatic activity during follow-up, adjusting treatment to vasculitis activity indexes only, may lead to irreversible liver damage. Current evidence-based therapeutic recommendations advise that patients with systemic vasculitis involving small and medium-sized vessels should be treated with prednisone and an immunosuppressive agent13. Cyclophosphamide is the gold-standard for inducing remission in systemic necrotizing vasculitis but increasing awareness of its toxicity advises the use of less harmful drugs for patients without severe compromise of vital organs, such as the patient reported13. Methotrexate has been also demonstrated to be effective in inducing remission in a randomized clinical trial14; however, this study mainly included patients with Wegener’s granulomatosis. A recent prospective, randomized clinical trial has demonstrated that about 50% of patients with MPA with no involvement of vital organs (five factor score of zero) can be induced to remission with glucocorticosteroids alone. For those unable to achieve/maintain remission with glucocorticosteroids alone, azathioprine has been equally effective than cyclophosphamide in inducing remission15. Azathioprine is currently the gold-standard for the treatment of AIH and experience with other drugs is anecdotal5,6. Although not exempt of potential hepatotoxicity, the hepatic profile of azathioprine is safer than that of other drugs effective for systemic vasculitis. Azathioprine was, then, the adjuvant therapy chosen for our patient, with such uncommon, perhaps underrecognized, combination of diseases. Treatment was effective and she successfully achieved remission with no recurrences or adverse events during 27-month follow-up. Financing Supported by Ministerio de Ciencia e Innovación SAF 08/04328 and SGR 0300/2005. S. Prieto-González was a post-residency research award recipient form Hospital Clı́nic. M.C. Cid and G. Espı́gol-Frigolé were supported by Instituto de Salud Carlos III. R. Estruch was supported by CIBER 06/03. Conflict of interest The authors declare no conflicts of interest. References 1. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–92. 2. Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. 2007;62:222–7. 3. Gómez-Puerta JA, Espinosa G, Morlà R, Cid MC, Cervera R. Interstitial lung disease as a presenting manifestation of microscopic polyangiitis successfully treated with mycophenolate mofetil. Clin Exp Rheumatol. 2009;27:166–7. 4. Amezcua-Guerra LM, Prieto P, Bojalil R, Pineda C, Amigo MC. Microscopic polyangiitis associated with primary biliary cirrhosis: a causal or casual association? J Rheumatol. 2006;33:2351–3. 5. Krawitt EL. Autoimmune hepatitis. N Engl J Med. 2006;354:54–66. 6. Teufel A, Galle PR, Kanzler S. Update on autoimmune hepatitis. World J Gastroenterol. 2009;15:1035–41. 7. Hennes EM, Zeniya M, Czaja GN, Parés A, Dalekos GN, Krawitt EL, et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology. 2008;48:169–76. 8. Inada C, Yoshida H, Sumino M, Morita Y, Shimokawa Y, Sata M, et al. A case of microscopic polyarteritis nodosa associated with autoimmune hepatitis complicated with rheumatoid arthritis and chronic tiroiditis. Nipon Shokakibyo Gakkai Zasshi. 2000;97:925–9. 9. Suwa A, Inada S, Tanabe M, Yamada T, Goto M, Imaeda H, et al. An autopsy case of anti-neutrophil cytoplasmic antibodies associated vasculitis accompanied by autoimmune hepatitis and hepatocellular carcinoma. Nihon Rinsho Meneki Gakkai Kaishi. 1997;20:117–25. 10. Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, et al. The American College of Rheumatology 1990 criteria for the classification of giantcell arteritis. Arthritis Rheum. 1990;33:1122–8. 11. Esteban MJ, Font C, Hernández-Rodrı́guez J, Valls-Solé J, Sanmartı́ R, Cardellach F, et al. Small-vessel vasculitis surrounding a spared temporal artery. Arthritis Rheum. 2001;44:1387–95. 12. Hazleman B. Laboratory investigations useful in the evaluation of polymyalgia rheumatica and giant-cell arteritis. Clin Exp Rheumatol. 2000;18:S29–31. 13. Mukhtyar C, Guillevin L, Cid MC, Dasgupta B, de Groot K, Gross W, et al. EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis. 2009;68:310–7. 14. De Groot K, Rasmussen N, Bacon PA, Tervaert JW, Feighery C, Gregorini G, et al. Randomized trial of cyclophosphamide versus methotrexate for induction of remission in early systemic antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum. 2005;52:2461–9. 15. Ribi C, Cohen P, Pagnoux C, Mahr A, Arène JP, Puéchal X, et al. Treatment of polyarteritis nodosa and microscopic polyangiitis without poor prognosis factors: a prospective randomized study on 124 patients. Arthritis Rheum. 2010;62:1186–97.






![Criterios HAI hepatology 2008 48 (5) 1540-1548[1]](http://s2.studylib.es/store/data/008899439_1-a534ee0ad48aa86e86e69f309b158cb4-300x300.png)