General Health Appraisal for enrollment in Child Care
Anuncio

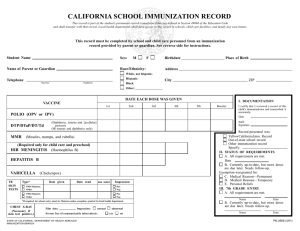
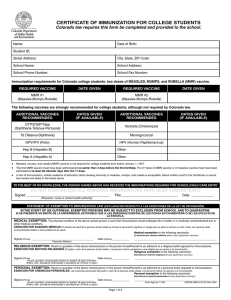
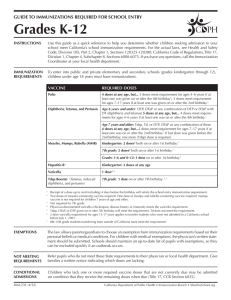
General Health Appraisal for enrollment in Child Care (To be Completed by a Health Care Professional) Child’s Name: _________________________________________ Birth Date: ____________ Health History & Medical Information pertinent to routine child care & emergencies: ______ None ______ Yes (Please describe): Special diet: ____________________________________________________________ Allergies: ____________________________________________________________ Type of reaction: ____________________________________________________________ Current medications: ____________________________________________________________ Describe any recurrent health problem (such as asthma, seizures, ear infections, diabetes, etc.) illness, hospitalization, or concerns with development. ______ None ______ Please describe _________________________________________________________________________________________ Comments: (include instructions to the child card providers(s) _________________________________________________________________________________________ Date of most recent examination of child (within the last 12 months): ______________________________ Weight __________ Height: __________ Vision: __________ Hearing: __________ Dental Screening: __________ Health Care Provider Name: ______________________________________ Phone #: ________________ Health Care Provider Signature: ___________________________________ Date: ________________ Health Care Provider Stamp I ________________________________________ give consent for my child’s health care provider and First United Methodist Church MMO provider to discuss my child’s health concerns. Parent/Guardian Name: ___________________________________________________________________ Signature: ________________________________________________________ Date: _________________ GENERAL HEALTH APPRAISAL FORM PARENT please complete AND SIGN Child’s Name:_______________________________________________________ Birthdate: _____________________ Allergies: q None or Describe___________________________________________________________________________________________ Type of Reaction ____________________________________________________________________________________________________ Diet: q Breast Fed q Formula _______________________ qAge Appropriate qSpecial Diet ________________________________________________________________________________________________ Sleep: Your health care provider recommends that all infants less than 1 year of age be placed on their back for sleep. q Preventive creams/ointments/sunscreen may be applied as requested in writing by parent unless skin is broken or bleeding. I, ________________________________________ give consent for my child’s care health provider, school child care or camp personnel to discuss my child’s health concerns. My child’s health provider may fax this form (& applicable attachments) to my child’s school, child care or camp personnel. FAX #: _____________________________ DATE: _____________________________ Parent/Guardian Signature___________________________________________________________________ HEALTH CARE PROVIDER: Please Complete After Parent Section Completed Date of Last Health Appraisal: _____________________________ Weight @ Exam: _______________________________________ Physical Exam: q Normal q Abnormal (Specify any physical abnormalities)_____________________________________________________ Allergies: q None or Describe__________________________ Type of Reaction __________________________________________________ Significant Health Concerns: qSevere Allergies qReactive Airway Disease qAsthma qSeizures qDiabetes qHospitalizations qDevelopmental Delays qBehavior Concerns qVision qHearing qDental qNutrition q Other ________________________________ Explain above concern (if necessary, include instructions to care providers): ______________________________________________________ Current Medications/Special Diet: q None or Describe ______________________________________________________________________ Separate medication authorization form is required for medications given in school, child care or camp For Fever Reducer or Pain Reliever (for 3 consecutive days without additional medical authorization) PLEASE CHOOSE ONE PRODUCT OR qAcetaminophen (Tylenol) may be given for pain or fever over 102 degrees every 4 hours as needed Dose ____________________ or see the attached age-appropriate dosage schedule from our office qIbuprofen (Motrin, Advil) may be given for pain or for fever over 102 degrees every 6 hours as needed Dose ____________________ or see the attached age-appropriate dosage schedule from our office Immunizations: qUp-to-Date q See attached immunization record qAdministered today: _____________________________________________ Health Care Provider: Complete if Appropriate **ONLY REQUIRED BY EARLY HEAD START AND HEAD START PROGRAMS PER STATE EPSDT SCHEDULE** ** Height @ Exam _____ ** B/P _____ **Head Circumference (up to 12 months) _______ ** ** HCT/HGB _____ ** Lead Level qNot at risk or Level _____ **TB qNot at risk or Test Results q Normal q Abnormal **Screenings Performed: qVision: qNormal qAbnormal qHearing: qNormal qAbnormal qDental: qNormal qAbnormalRecommended Follow-up________________________________________________________________________________________ Provider Signature Next Well Visit: q Per AAP guidelines* or q Age__________ This child is healthy and may participate in all routine activities in school sports, child care or camp program. Any concerns or exceptions are identified on this form. Office Stamp Or write Name, Address, Phone, # _____________________________________________________ Signature of Health Care Provider (certifying form was reviewed) Date: _______________ The Colorado Chapter of the American Academy of Pediatrics (AAP) and Healthy Child Care Colorado have approved this form. 04/07 *The AAP recommends that children from 0-12 years have health appraisal visits at: 2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. Copyright 2007 Colorado Chapter of the American Academy of Pediatrics Certificate of Immunization 6 CCR 1009—The Infant Immunization Program and Immunization of Students Attending School Schools shall have on file an official Certificate of Immunization for every student enrolled. COLORADO LAW REQUIRES THAT THIS FORM BE COMPLETED FOR EACH STUDENT ATTENDING COLORADO SCHOOLS Name_________________________________________________________________ Date of Birth _______________________________________ Parent/Guardian __________________________________________________________________________________________________________ COLORADO DEPARTMENT OF PUBLIC HEALTH AND ENVIRONMENT—CERTIFICATE OF IMMUNIZATION Hep B Vaccine Hepatitis B DTaP Diphtheria, Tetanus, Pertussis (pediatric) Tdap Tetanus, Diphtheria, Pertussis Hib Haemophilus influenzae type b PCV Pneumococcal Conjugate DT Diphtheria, Tetanus (pediatric) Td Tetanus, Diphtheria IPV/OPV Measles, Mumps, Rubella Mumps Mumps Measles Measles Rubella Rubella Varicella Chickenpox HPV Human Papillomavirus MCV4/MPSV 4 Meningococcal Flu Influenza Hep A Titer Date Polio MMR Rota Enter the month, day and year each immunization was given Provider Documentation Date of Disease Positive Screen Date ______________________________ _____________________________ Vaccines recorded below this line are recommended. Recording of dates is encouraged. Rotavirus Hepatitis A Other THIS SECTION CAN BE COMPLETED BY CHILD CARE/SCHOOL/HEALTH CARE PROVIDER A) Child Care Up to Date Up to date through 6 months of age for Colorado School Immunization Requirements B) Child Care Up to Date Up to date through 18 months of age for Colorado School Immunization Requirements C) Child Care/Pre-school/Pre-K* Up to date for Child Care/Pre-School/Pre-K for Colorado School Immunization Requirements D) Complete for K–5th Grade Up to date for K–5th Grade for Colorado School Immunization Requirements ______________________________________________________________ Update Signature Date Update Signature Date Update Signature Date Update Signature Date ______________________________________________________________ ______________________________________________________________ ______________________________________________________________ * If age 4 years and fulfills Requirements for Pre-School & Kindergarten, check BOTH Boxes C and D. CDPHE-IMM CI RC Rev. 1/16 Name_________________________________________________________________ Date of Birth _______________________________________ Parent/Guardian __________________________________________________________________________________________________________ STATEMENT OF EXEMPTION TO IMMUNIZATION LAW (DECLARACIÓN RESPECTO A LAS EXENCIONES DE LA LEY DE VACUNACIÓN) IN THE EVENT OF AN OUTBREAK, EXEMPTED PERSONS MAY BE SUBJECT TO EXCLUSION FROM SCHOOL AND TO QUARANTINE. SI SE PRESENTA UN BROTE DE LA ENFERMEDAD, ES POSIBLE QUE A LAS PERSONAS EXENTAS SE LES PONGA EN CUARENTENA O SE LES EXCLUYA DE LA ESCUELA. MEDICAL EXEMPTION: The physical condition of the above named person is such that immunization would endanger life or health or is medically contraindicated due to other medical conditions. EXENCIÓN POR RAZONES MÉDICAS: El estado de salud de la persona arriba citada es tal que la vacunación significa un riesgo para su salud o incluso su vida; o bien, las vacunas están contraindicadas debido a otros problemas de salud. Medical exemption to the following vaccine(s): La exención por razones médicas aplica a la(s) siguiente(s) vacuna(s): Hep B DTaP Tdap Hib IPV PCV MMR VAR Signed (Firma) _______________________________________________________________ Physician (Médico) Date (Fecha) ______________________________ RELIGIOUS EXEMPTION: Parent or guardian of the above named person or the person himself/herself is an adherent to a religious belief opposed to immunizations. EXENCIÓN POR MOTIVOS RELIGIOSOS: El padre o tutor de la persona arriba citada, o la persona misma, pertenece a una religión que se opone a la inmunización. Religious exemption to the following vaccine(s): Exención por motivos religiosos de la(s) siguiente(s) vacuna(s): Hep B DTaP Tdap Hib IPV PCV MMR VAR Signed (Firma) _______________________________________________________________ Parent, guardian, emancipated student/consenting minor (Padre, tutor, estudiante emancipado o consentimiento del menor) Date (Fecha) ______________________________ PERSONAL EXEMPTION: Parent or guardian of the above named person or the person himself/herself is an adherent to a personal belief opposed to immunizations. EXENCIÓN POR CREENCIAS PERSONALES: Las creencias personales del padre o tutor de la persona arriba citada, o la persona misma, se oponen a la inmunización. Personal exemption to the following vaccine(s): Exención por creencias personales de la(s) siguiente(s) vacuna(s): Hep B DTaP Tdap Hib IPV PCV MMR VAR Signed (Firma) _______________________________________________________________ Parent, guardian, emancipated student/consenting minor (Padre, tutor, estudiante emancipado o consentimiento del menor) Date (Fecha) ______________________________