The effectiveness of physical activity in preventing type 2
Anuncio

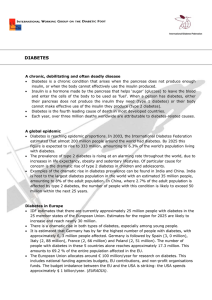
Journal of Diabetology, June 2012; 2:1 http://www.journalofdiabetology.org/ Review Article: The effectiveness of physical activity in preventing type 2 diabetes in high risk individuals using well -structured interventions: a systematic review A.M . M alk aw i Abstract: The aim of this systematic review was to evaluate the effectiveness of well-structured interventions which promote physical activity in high risk individuals with type 2 diabetes. Using ISI web of knowledge and PubMed data bases in addition to snowballing, a total of 19 articles met the inclusion and exclusion criteria. Five articles were related to diabetes prevention interventions in USA. Four articles were related to diabetes prevention interventions in the UK. Five were related to diabetes prevention interventions in Finland. Five interventions were identified in Netherlands, India, China, Brazil and Australia. The review found strong evidence regarding the effectiveness of well-structured physical activity interventions in reducing the incidence of type 2 diabetes. Moreover, well-structured interventions were also found to be effective in restoring glucose measures including fasting plasma glucose and 2h plasma glucose. However, there was weak evidence regarding the effectiveness of well-structured interventions in increasing the level of physical activity. The review suggests using well-structured lifestyle interventions which include both physical activity and dietary advice. More research regarding the effectiveness of single physical activity interventions in preventing type 2 diabetes is recommended. Key words: Physical activity, Exercise, Type 2 diabetes, Prevention *Corresponding author: (Current Details) Ahmad Mohammad Malkawi Schools of Health and Human Sciences, University of Essex, Wivenhoe Park, Colchester, United Kingdom. E-mail: m9malkawi@hotmail.com Introduction: Diabetes Mellitus is a growing public health problem worldwide and is considered as one of the main threats to human health in the 21st century [1]. The global prevalence of diabetes in adults aged 20 years or above was estimated as 171 million in the year 2000. This figure is expected to double by the year 2030 [2]. Type 2 diabetes mellitus (non-insulin dependent diabetes mellitus) is the most common type of diabetes and accounts for 9095% of overall diabetes cases [3]. Pre-diabetic conditions including impaired fasting glucose and impaired glucose tolerance [4,5], being overweight or obese (Body mass index ≥ 25 kg/m2) [6], family history (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 1 of diabetes [7], gestational diabetes [8] and negative lifestyle habits such as lack of exercise and smoking are considered the main risk factors for type 2 diabetes [9]. Once diabetes is diagnosed, it is expensive to treat as a result of medication costs, regular clinic visits, lab testing, glucose monitoring and treatment of complications [10]. Type 2 diabetes is associated with many complications such as cardiovascular diseases, renal diseases [11], advanced skin, muscle, bone infections [12], impaired quality of life [13] and psychological effects such as depression or anxiety. Type 2 diabetes is caused by both genetic and life style factors. However, the predisposition of the genetic factor requires the presence of environmental and life style factors. Moreover, most of the dramatic increase in type 2 diabetes occurred within populations that witnessed rapid and major life style changes [14]. Physical activity can be helpful in the primary and secondary prevention of diabetes [15]. There is robust evidence regarding the protective effect of physical activity in the development of type 2 diabetes. Studies Journal of Diabetology, June 2012; 2:1 conducted by Manson et al., (1992), FultonKehoe et al., (2001) and Engberg et al., (2009) observed that people with a high level of physical activity were less likely to develop type 2 diabetes in the future [16,17,18]. There is good evidence that physical activity has many other desirable effects including better health related quality of life in addition to the primary and secondary prevention of many chronic diseases such as cardiovascular disease, diabetes and cancer [19,20]. However, few randomized control trials (RCTs) were conducted regarding the effect of physical activity in reducing morbidity and mortality [21]. Brisk walk (for at least 150 minutes per week or 30 minutes per day) [22,23], progressive resistance training such as weight lifting [24] and yoga exercises [25] have potential benefits in terms of prevention of type 2 diabetes. It is already known that physical activity can prevent diabetes, but it is not known how much these interventions are successful in prevention of type 2 diabetes. The aim of this review was to evaluate the effectiveness of well-structured interventions which promote physical activity in prevent type 2 diabetes in high risk individuals. Methodology The rationale for this systematic review One relevant systematic review identified by Yates et al., assessed the independent effect of exercise on diabetes risk for people who have impaired glucose tolerance [26]. Review by Yates et al., was excellent in terms of its results synthesis. For instance, the review differentiated between the interventions which investigated the effect of exercise alone and those who used both diet and exercise. However, Yates et al., included only eight studies in the final results. He excluded simple intervention studies which included only a brief written or verbal physical activity advice [26]. Also, he only included studies which recruited people with pre-diabetes (IGT and/or IFG). The current review can be more comprehensive as it includes more number of studies (see the results section). It clearly defines well-structured interventions and includes all types of high risk individuals such as obese people, those who have IGT and/or IFG and people with family (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 2 http://www.journalofdiabetology.org/ history of diabetes. Moreover, this review is updated and includes many studies from 2006 till 2011 (the date when Yates et al., limited his findings) [26]. Search Strategy An electronic search was undertaken through PubMed and ISI web of knowledge database. The search terms used were “Prevent* diabetes 2” and “promote* physical activity”. The same research term combination was used for PubMed and ISI web of knowledge database. Inclusion and exclusion criteria Time and language The search was restricted to English language with primary source articles published until the 1st of June 2011. Participants The review included studies which recruited people who were at higher risk of developing type 2 diabetes in the future (as discussed in the introduction). Studies which recruited people who already had diabetes were excluded as the review was concerned about the primary prevention of type 2 diabetes. In addition, participants were not under medications which alter blood glucose tolerance or had certain medical conditions such as cardiovascular diseases which prevented them from taking part in the intervention. There was no restriction regarding the sample size. Interventions This review included interventions which promote physical activity either separately or as part of a lifestyle or dietary intervention. Any intervention which was based on medications only to prevent diabetes such as metformin and acarbose was excluded. The intervention should have aimed at preventing type 2 diabetes. Only well-structured interventions which promoted exercise or physical activity were included. Glanz et al., argued that sustained behavioral change could be achieved by using more tools, strategies and better understanding of psychological theories [27]. Brief advice was unlikely to achieve the desired behavioral change. An intervention was considered well-structured if it contained at least two of the following criteria: Journal of Diabetology, June 2012; 2:1 Curriculum based (interventions delivered certain syllabus). interventions according to Interventions which contained individual (face to face) sessions. Interventions which used additional supportive materials or equipment including advice leaflets and pedometer. Theory based interventions or interventions which used a counseling approach for changing behaviors (this should be clearly stated by the author). Interventions which included teaching behavior change strategies such as goal setting, action planning and self-monitoring. Interventions which included clearly defined exercise recommendations including exercise type, frequency and duration (such as 30 minutes brisk walk per day) or detailed specific supervised exercise sessions. Interventions which were developed or delivered by experts or trained facilitator. Outcome measures The study should have assessed the change of at least one of the following measures as a result of the intervention; glucose measure, the level of physical activity and the incidence of diabetes. Study design The review included quantitative studies including randomized control trials, cohort, longitudinal pretest and posttest and pilot studies. The control group should have received placebo or mini intervention (general lifestyle advice). There was no restriction regarding the follow up period of participants. The process of articles refining Using ISI web of knowledge data base with the previously mentioned search terms, 110 articles were initially identified. This number was identified when the search was refined to academic journals, English language and public, environmental and occupational health as subject areas. Regarding PubMed database, 418 articles were initially identified. After reading the paper’s titles and abstracts (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 3 http://www.journalofdiabetology.org/ and application of inclusion and exclusion criteria, 19 articles were initially selected from ISI web of knowledge and 38 articles from Pub Med. A total of 55 articles were potentially selected from ISI web of knowledge and PubMed database. Eight articles were selected by snowballing from the 55 potential articles. Twelve articles were selected from the potential 55 articles and a total of 19 articles met the inclusion criteria (see appendix 1). Results As mentioned previously, 19 articles were finally selected. Five articles were related to diabetes prevention programs in USA [23,28,29,30,31]. Four articles were identified related to interventions in the UK [32,33,34,35]. Five papers were related to interventions conducted in Finland [22,36,37,39,40]. One paper each evaluated interventions in: China [41], Brazil [42], India [43], Netherland [44] and Australia [38]. Brief description of the study design and outcome measurement To achieve the aim of this systematic review, the result section focused on two parameters regarding glucose measures including fasting plasma glucose and 2-hour plasma glucose. Moreover, the incidence or cumulative incidence of diabetes was mentioned if it was measured by the selected studies. In addition, three parameters were used to assess the change in physical activity level among participants including self-reported physical activity, aerobic fitness (VO2 max) and the ambulatory activity. Finally, syntheses of the results were done using glucose and physical activity parameters according to the follow up period (3 months to 10 years). The effect of well-structured interventions on reducing glucose measures Yang et al., (2009) and Thompson et al., (2008) found no significant improvement in fasting plasma glucose after three and six months respectively [28,31]. However, Allen et al., (2008) found a significant improvement in fasting plasma glucose after six months follow up [29]. The process of recruitment in the three previously mentioned studies was done through voice mail messages, flyers posted in hospitals and advertisements in local newspapers. This Journal of Diabetology, June 2012; 2:1 facilitated targeting different kinds of people and advertisements in local newspapers. This facilitated targeting different kinds of people and reduced the possibility of selection bias. However, Yang et al., (2009) et al., and Allen et al., (2008) recruited small number of participants [29,31]. Kinmonth et al., (2008) and Thompson et al., (2008) found no significant improvement in fasting plasma glucose after one year follow up [28,32]. Sartorelli et al., (2005) and Absetz et al., (2007) found no significant improvement both in 2-hour glucose and fasting plasma glucose measures during the same period [39,42]. Absetz et al., (2007), Sartorelli et al., (2005) and Kinmonth et al., (2008) recruited participants from general practices or health centers [32,39,42]. Therefore, these studies were prone to selection bias. On the other hand, Yates et al., (2009), Laatikainen et al., (2007), Tuomilehto et al., (2001) and Lindström et al., (2003 b) found that fasting plasma glucose and 2 h plasma glucose were decreased significantly after one year follow up [22,34,36,38]. Allen et al., (2008) found that the mean change of fasting blood glucose was significantly reduced after 18 months follow up [29]. The studies which were carried out by Yates et al., (2009), Lindström et al., (2003 b), Tuomilehto et al., (2001) and Laatikainen et al., (2007) were also prone to selection bias [22,34,36,38]. For example, Yates et al., (2009) recruited participants from diabetes screening program in Leicester [34]. Studies conducted by Yates et al., (2009), Lindström et al., (2003 b), Tuomilehto et al., (2001), Sartorelli et al., (2005) and Kinmonth et al., (2008) were partly blinded randomized trials [22,32,34,36,42]. It was difficult to conduct a double blinded trial because trainers who lead well-structured physical activity sessions had to know group allocation. Lindström et al., (2003 b) and Mensink et al., (2003) found a significant improvement in 2-hour glucose after 2 years follow up [36,44]. Yates et al., (2011) found significant improvement in both fasting plasma glucose and 2 h glucose after 2 years follow up in the group which received both structured education and pedometer [35]. Lindström et al., (2003 a) found no significant improvement in fasting plasma glucose and 2 hour plasma glucose after 3 years follow up [37]. Knowler et al., (2002) found a significant reduction in fasting plasma glucose after 4 years follow up (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 4 http://www.journalofdiabetology.org/ [23]. The US diabetes prevention program provided a longer term results and found that the mean of fasting glucose improved after 10 years follow up [30]. However, a long follow up period had a problem of high number of participants who dropped out during the study. In summary, there is good evidence that effectiveness of well-structured interventions can improve glucose measures. Most of the positive results came from the US and Finnish diabetes prevention programs which have larger sample size and long follow up period (see the results table). The effect of well-structured interventions on reducing the incidence of type 2 diabetes All studies which were identified found a significant reduction in the cumulative incidence of diabetes including Tuomilehto et al., (2001), Ramachandran et al., (2006), Knowler et al., 2002, Pan et al., 1997, Diabetes Prevention Program Research Group et al., 2000 and Lindström et al., (2003 b) [22,23,30,36,41,43]. For example, the US diabetes prevention program recorded that the incidence of diabetes was 58% lower in the intervention than that of the control group after an average of three years follow up [23]. The studies which measured the incidence of type 2 diabetes gave better indication regarding the effectiveness of these programs because studies may find significant improvement in fasting plasma glucose or 2 hour plasma glucose measures among participants, but it was difficult to determine if there was an actual reduction in the number of patients with diabetes. The effect of well-structured interventions on increasing the level of physical activity Thompson et al., (2008), Greaves et al., (2008), Kinmonth et al., (2008), Sartorelli et al., (2005) and Allen et al., (2008) found no significant improvement in self-reported physical activity after a follow up period that ranged between six and 18 months [28,29, 32,33,42]. On the other hand, Laatikainen et al., (2007), Lindstr ِm et al., (2003a), Tuomilehto et al., (2001), Yates et al., (2009) and Lindstrِm et al., (2003 b) found that self-reported physical activity significantly improved after one year follow up [22,34,36,37,38]. Kinmonth et al., (2008), Allen Journal of Diabetology, June 2012; 2:1 et al., (2008) and Thompson et al., (2008) found no significant improvement in cardio respiratory fitness (VO2max) after one year and 16 months follow up period [28,29,32]. Yates et al., (2009) found that the ambulatory activity improved after one year follow up [34]. Mensink et al., (2003) found that the aerobic fitness significantly improved after 2 years [44]. Ramachandran et al., (2006) found significant improvement in self-reported physical activity after 30 months follow up [43]. Lindstrِm et al., (2003 a), Knowler et al., (2002), Laaksonen et al., (2005) and Pan et al., (1997) found a significant increase in selfreported physical activity after three and four years follow up [23,37,40,41]. In summary, there is weak evidence regarding the effectiveness of well-structured interventions in increasing the level of physical activity as the majority of studies relied only on self-reported data in addition to the fact that it is difficult to measure physical activity in general. Can physical activity alone be enough to prevent type 2 diabetes? Four studies which were carried out by Kinmonth et al., (2008), Yates et al., (2009), Yang et al., (2009) and Yates et al., (2011) were single physical activity interventions [31,32,34,35]. Only Yates et al., (2009) and Yates et al., (2011) who assessed PREPARE program found effectiveness in restoring glucose measures [34,35]. Interestingly, the Chinese diabetes intervention allocated participants into four groups: control, diet, exercise and diet + exercise groups. After an average of six years follow up, there was no significant difference in the incidence of diabetes between the three intervention groups which means that physical activity intervention has a similar effect to both diet and physical activity intervention [41]. However, most of the positive results were recorded from lifestyle interventions which included both diet and lifestyle counseling. Therefore, it is difficult to confirm that physical activity alone is enough to prevent type 2 diabetes and there is still a need for more research in this area. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 5 http://www.journalofdiabetology.org/ Discussion The results found a potential effectiveness of well-structured interventions which include promoting physical activity especially in terms of reducing diabetes incidence and improving glucose measures. The quality and strength of each paper included in this review can lead to different results. Moreover, other factors can play an important role including the nature of the control group and the accuracy of glucose tests. Regarding the nature of the control group, it differed from one study to another. Most of the trials provided the control group with a mini intervention for ethical reasons. For example, the trial which was carried out by Tuomilehto et al., (2001) to assess the effectiveness of the Finnish diabetes prevention program provided the participants of the control group with only annual oral and written information based on diet and exercise advices without individual counseling [22]. Whereas, Knowler et al., (2002) who assessed the US program provided participants of the control group with 20-30 minutes of annual individual session [23]. Regarding the accuracy of glucose tolerance tests, some studies such as Knowler et al., (2002) conducted more than one glucose test to validate their results, while others such as Allen et al., (2008) conducted only one test [29]. Most of the studies which found positive results regarding the effect of well-structured interventions were conducted according to the Finnish, US, Chinese and Indian diabetes prevention programs in addition to PREPARE intervention (the UK program). The most common themes between all these interventions are that they were conducted at national level, had clearly defined physical activity objectives (such as 30 minutes of daily walking) and were more likely to provide personal counseling sessions. In addition, most of them were lifestyle programs (included both dietary and exercise interventions). Lifestyle interventions were considered too expensive as a result of the cost of delivering the intervention including trained health care educators, the cost of exercise equipment and the cost of participant’s time [45]. On the other hand, lifestyle interventions have multiple positive health outcomes including reducing the body mass index, improving blood pressure, prevention of Journal of Diabetology, June 2012; 2:1 hypertension and many chronic illnesses [46]. These results can be partly agreed with Rutter and Quine (2002) who said that good interventions must be theory driven, tackle an important health issue and have a clearly defined process of outcome evaluation [47]. The IMAGE toolkit provides clear recommendations regarding effective diabetes prevention programs. The toolkit recommends using both diet and physical activity counseling to prevent diabetes. Moreover, it suggests clearly defining the targeted group and use different counseling approaches during counseling. Counseling can include teaching participants many important skills such as goal setting, action plan and problem solving to identify barriers and give solutions to these barriers. In addition, counseling can include raising awareness regarding the benefits of physical activity. This toolkit suggests using many supportive materials such as audio visual equipment, illustrations and nutritional diaries. Finally, it IMAGE recommends using a structured evaluation sheet to facilitate evaluating the intervention [48]. There are a lot of challenges regarding the implementation of well-structured interventions. At first, it is important to apply more effective approaches to identify high risk people rather than targeting people from GPs or health centers. Therefore, it is important to use various ways to recruit participants such as mass media, health centers and emails [48]. Moreover, a special consideration should be given when applying well-structured intervention in countries where there is lack of adequate infrastructure and sport facilities. To achieve sustainable results, it is important to provide sidewalks and bike paths to encourage walking and cycling and collaborate with nonprofit organizations and policy makers in order to target the social environment [48,49]. Furthermore, it is important to consider the context in addition to the cultural and religious barriers to ensure that the intervention is acceptable and suitable to the target population [50]. One of the issues which should be considered before implementing physical activity interventions is the assessment and recording of physical activity during patient follow up. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 6 http://www.journalofdiabetology.org/ Physical activity can be assessed subjectively using self-reported questionnaire or objectively (directly measured) using certain equipment’s such as pedometers [51]. Self-reported questionnaires are commonly used because they are cheap and easy to use [52]. However, both methods have drawbacks and are subjected to potential bias [53]. Self-reported questionnaires do not account for less than 10 minutes physical activity and may not be able to capture all types of physical activity. Whereas, using certain devices to measure physical activity may not be worn in activities such as swimming [51, 53]. Troiano (2012) recommended using both objective and subjective measurements to validate our results and get better measurement and recording of physical activity [54]. Limitations This systematic review has many limitations. It only included English language articles. Many high quality articles which are written in German, French and Swedish may not included and this may affect the final results. This review included only published articles, excluding grey literature (unpublished literature) can make the review prone to publication bias. Hopewell et al., (2009) found that trials which show a positive effect are more likely to be published rather than interventions which show a negative or no effect at all [55]. Moreover, including only published literature may ignore hidden evidences which could be relevant to this review. Factors related to time restraints in addition to that it is based on a single novice researcher effort the thing which makes it not as thorough as an experienced research team [56]. Most of the interventions which were included in this review excluded participants with certain medical conditions such as cardiovascular diseases for ethical reasons. This may lead to exclusion of a large population who are at risk of developing type 2 diabetes. Conclusion Type 2 diabetes mellitus is a significant public health problem. It has significant burden at the individual and national level. There is strong evidence that physical activity is effective in the primary prevention of type 2 diabetes and Journal of Diabetology, June 2012; 2:1 its associated diseases as well as other chronic diseases. Although we know that physical activity can prevent type 2 diabetes, we still need to know and evaluate the effectiveness of the interventions which promote physical activity in the real world. This review found that there is a good evidence of the effectiveness of well-structured interventions in reducing glucose measures and stronger evidence regarding reduction in the incidence of type 2 diabetes. However, it found weak evidence regarding the effectiveness of well-structured interventions in increasing the level of physical activity because most of the studies rely on selfreported questionnaires. Therefore, it is recommended for future studies to measure physical activity subjectively and objectively to support their findings. Moreover, this review cannot give any recommendations regarding the type, duration and intensity of physical activity which is more effective in prevention of diabetes. There is need of more research to answer many questions. For instance, can six sessions per day (five min per session) achieve the same benefit as single daily 30 minutes session? [57]. Can various amounts of moderate and vigorous intensity of physical activity below the recommended threshold be combined to meet the recommended level? [21]. There is need for more research to confirm if physical activity alone can be enough to prevent type 2 diabetes. Moreover, it is recommended to implement lifestyle interventions because most of the positive results were recorded from them and they have many other health benefits. Before implementing a physical activity intervention anywhere, it is important to ensure that it has clearly defined objectives and process of evaluation in addition to implementing culturally accepted interventions. It is important to apply more effective ways to identify people who are at high risk of type 2 diabetes rather than relying on GPs. In addition, it is recommended to support these interventions with adequate infrastructure. Acknowledgements The author is grateful to Dr. Vale Thurtle who supervised him in his dissertation and provided valuable feedbacks for this literature review. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 7 http://www.journalofdiabetology.org/ References: 1. Zimmet P, Alberti K, Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414: 782-787. 2. Wild S, Roglic G, Green A, Sicree R, King H. Global Prevalence of Diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27: 1047–1053. 3. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2008; 31: S55-S60. 4. Kadowaki T, Miyake Y, Hagura R, Akanuma Y, Kajinuma H, Kuzuya N, et al. Risk factors for worsening to diabetes in subjects with impaired glucose tolerance. Diabetologia 1984; 26: 44-49 5. Nichols G, Hillier T, Brown J. Progression from newly acquired impaired fasting glucose to type 2 diabetes. Diabetes Care 2007; 30: 228-233. 6. Wannamethee S, Shaper A. Weight change and duration of overweight and obesity in the incidence of type 2 diabetes. Diabetes Care 1999; 22: 1266-1272. 7. Bjørnholt J, Erikssen G, Liestøl K, Jervell J, Thaulow E, Erikssen J. Type 2 diabetes and maternal family history: an impact beyond slow glucose removal rate and fasting hyperglycemia in low-risk individuals? Results from 22.5 years of follow-up of healthy nondiabetic men. Diabetes Care 2000; 23: 1255-1259. 8. Kim C, Newton K, Knopp R. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 2002; 25: 1862-1868. 9. Hu F, Manson J, Stampfer M, Colditz G, Liu S, Solomon C, et al. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. The New England Journal of Medicine 2001; 345: 790-797. Journal of Diabetology, June 2012; 2:1 10. Dagogo-Jack S. Primary prevention of type 2 diabetes in developing countries. Journal of the National Medical Association 2006; 98: 415-419. 11. Brown J, Pedula K, Bakst A. The Progressive Cost of Complications in Type 2 Diabetes Mellitus. Archives Internal Medicine 1999; 159: 1873-1880. 12. Williams R, Van Gaal L, Lucioni C. Assessing the impact of complications on the costs of Type II diabetes. Diabetologia 2002; 45: S13– S17. 13. Rubin R, Peyrot M. Quality of life and diabetes. Diabetes/Metabolism Research and Reviews 1999; 15: 205-218. 14. Alberti K, Zimmet P, Shaw J. International Diabetes Federation: a consensus on type 2 diabetes prevention. Diabetic Medicine 2007, 24: 451–463. 15. Sato Y. Diabetes and life-styles: role of physical exercise for primary prevention. British Journal of Nutrition 2000; 84: S187S190. 16. Manson J, Nathan D, Krolewski A, Stampfer M, Willett W, Hennekens C. A Prospective Study of Exercise and Incidence of Diabetes Among US Male Physicians. The Journal of the American Medical Association 1992; 268: 63-67. 17. Fulton-Kehoe D, Hamman RF, Baxter J, Marshall J. A case-control study of physical activity and non-insulin dependent diabetes mellitus (NIDDM). The San Luis Valley Diabetes Study. Annals of Epidemiology 2001; 11: 320-327. 18. Engberg S, Glumer C, Witte D, Jurgensen T, Borch-Johnsen K. Differential relationship between physical activity and progression to diabetes by glucose tolerance status: the Inter99 Study. Diabetologia 2009; 53: 70–78. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 8 http://www.journalofdiabetology.org/ 19. Penedo F, Dahn J. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry 2005; 18: 189193. 20. Warburton D, Nicol C, Bredin S. Health benefits of physical activity: the evidence. Canadian Medical Association Journal 2006; 174: 801-809. 21. Haskell W, Lee I, Pate R, Powell K, Blair S, Franklin B, et al. American College of Sports Medicine; American Heart Association. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007; 116: 1081-1093. 22. Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hsmslsinen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. The New England Journal of Medicine 2001; 344: 1343-1350. 23. Knowler W, Barrett-Connor E, Fowler S, Hamman R, Lachin J, Walker E, et al. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine 2002; 346: 393-403. 24. Willey K, Singh M. Battling insulin resistance in elderly obese people with type 2 diabetes: bring on the heavy weight. Diabetes Care 2003; 26: 1580-1588. 25. Bijlani R, Vempati R, Yadav R, Ray R, Gupta V, Sharma R, et al. A brief but comprehensive lifestyle education program based on yoga reduces risk factors for cardiovascular disease and diabetes mellitus. Journal of Alternative and Complementary Medicine 2005; 11: 267274. Journal of Diabetology, June 2012; 2:1 26. Yates T, Khunti K, Bull F, Gorely T, Davies M. The role of physical activity in the management of impaired glucose tolerance: a systematic review. Diabetologia 2007; 50: 1116-1126. 27. Glanz K, Rimer B, Viswanath K. Health behavior and health education theory, research and practice. San Francisco: John Wiley & Sons, 2008 28. Thompson J, Allen P, Helitzer D, Qualls C, Whyte A, Wolfe V, et al. Reducing diabetes risk in American Indian women. American Journal of Preventive Medicine 2008; 34 : 192-201. 29. Allen P, Thompson J, Herman C, Whyte A, Wolfe V, Qualls C, et al. Impact of periodic follow-up testing among urban American Indian women with impaired fasting glucose. Preventing Chronic Diseases 2008; 5: 1-10. 30. Diabetes Prevention Program Research Group, Knowler W, Fowler S, Hamman R, Christophi C, Hoffman H, Brenneman A, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 2009; 374: 1677-1686. 31. Yang K, Bernardo L, Sereika S, Conroy M, Balk J, Burke L. Utilization of 3-month Yoga Program for Adults at High Risk for Type 2 Diabetes: A Pilot Study. Evidence Based Complementary and Alternative Medicine 2009; 2011: 1-6. 32. Kinmonth A, Wareham N, Hardeman W, Sutton S, Prevost T, Fanshawe T, et al. Efficacy of a theory-based behavioural intervention to increase physical activity in an at-risk group in primary care (ProActive UK): a randomised trial. Lancet 2008; 371: 41–48. 33. Greaves C, Middlebrooke A, O'Loughlin L, Holland S, Piper J, Steele A, Motivational interviewing for modifying diabetes risk: a randomised controlled trial. British Journal of General Practice 2008; 58: 535-540. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 9 http://www.journalofdiabetology.org/ 34. Yates T, Davies M, Gorely T, Bull F, Khunti K. Effectiveness of a pragmatic education program designed to promote walking activity in individuals with impaired glucose tolerance: a randomized controlled trial. Diabetes Care 2009; 32: 1404–1410. 35. Yates T, Davies M, Sehmi S, Gorely T, Khunti K. The Pre-diabetes Risk Education and Physical Activity Recommendation and Encouragement (PREPARE) programme study: are improvements in glucose regulation sustained at 2 years? Diabetic Medicine 2011; 28: 1268–1271. 36. Lindstrom J, Louheranta A, Mannelin M, Rastas M, Salminen V, Eriksson J, et al. The Finnish Diabetes Prevention Study (DPS): Lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 2003; 26: 3230-3236. 37. Lindstrom J, Eriksson JG, Valle TT, Aunola S, Cepaitis Z, Hakumaki M, et al. Prevention of diabetes mellitus in subjects with impaired glucose tolerance in the Finnish Diabetes Prevention Study: results from a randomized clinical trial. Journal of American Society and Nephrology 2003; 14: S108-S113. 38. Laatikainen T, Dunbar J, Chapman A, Kilkkinen A, Vartiainen E, Heistaro S, et al. Prevention of type 2 diabetes by lifestyle intervention in an Australian primary health care setting: Greater Green Triangle (GGT) Diabetes Prevention Project. BioMed Central Public Health 2007; 19: 1-7. 39. Absetz P, Valve R, Oldenburg B, Heinonen H, Nissinen A, Fogelholm M, et al. Type 2 diabetes prevention in the "real world": oneyear results of the GOAL Implementation Trial. Diabetes Care 2007; 30: 2465-2470. 40. Laaksonen D, Lindstrom J, Lakka T, Eriksson J, Niskanen L, Wikstrom K, et al. Physical Activity in the Prevention of Type 2 Diabetes, the Finnish Diabetes Prevention Study. Diabetes 2005; 54: 158 –165. Journal of Diabetology, June 2012; 2:1 41. Pan X, Li G, Hu Y, Wang J, Yang W, An Z, et al. Effect of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 1997; 20: 537-544. http://www.journalofdiabetology.org/ 49. Edwards P, Tsouros A. Promoting physical activity and active living in urban environments. Turkey: World Health Organization; 2006. 42. Sartorelli D, Sciarra E, Franco L, Cardoso M. Beneficial effects of short-term nutritional counselling at the primary health-care level among Brazilian adults. Public Health Nutrition 2005; 8: 820-825. 50. Caperchione C, Kolt G, Tennent R, Mummery W. Physical activity behaviours of culturally and Linguistically Di verse (CALD) women living in Australia: a qualitative study of socio-cultural influences. BioMed Central Public Health 2011; 11: 1-10. 43. Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar A, Vijay V. The Indian Diabetes Prevention programme shows the lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006; 49: 289-297. 51. Prince S, Adamo K, Hamel M, Hardt J, Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. The International Journal of Behavioral Nutritional and Physical Activity 2008; 5: 1-24. 44. Mensink M, Blaak E, Corpeleijn E, Saris W, de-Bruin T, Feskens E. Lifestyle intervention according to general recommendations improves glucose tolerance. Obesity Research 2003; 11: 15881596. 52. Vanhees L, Lefevre J, Philippaerts R, Martens M, Huygens W, Troosters T, et al. How to assess physical activity? How to assess physical fitness? Eureopean Journal of Cardiovascular Prevention and Rehabilitation 2005; 12: 102-114. 45. Centers for Disease Control and Prevention Primary Prevention Working Group. Primary Prevention of Type 2 Diabetes Mellitus by Lifestyle Intervention: Implications for Health Policy. Annals of Internal Medicine 2004; 140: 951-957. 53. Luke A, Dugas L, Durazo-Arvizu R, Cao G, Cooper R. Assessing physical activity audits Relationship to Cardiovascular Risk Factors: NHANES 2003-2006. BioMed Central Public Health 2011; 11: 1-11. 46. Blue C, Black D. Synthesis of intervention research to modify physical activity and dietary behaviors. Research and Theory Nursing for Practice 2005; 19: 25-61. 47. Rutter D, Quine L. Changing Health Behaviors intervenrtion and research with social cognition models. USA: Philadelphia Open University Press; 2002. 48. IMAGE toolkit working group. Take action to prevent diabetes. A toolkit for the prevention of type 2 diabetes in Europe. Exeter: Brightsea press; 2010. 54. Troiano R. Can there be a single best measure of reported physical activity? American Journal of Clinical Nutrition 2009; 89: 862-70. 55. Hopewell S, Loudon K, Clarke M, Oxman A, Dickersin K. Publication bias in clinical trials due to statistical significance or direction of trial results (Review). UK: John Wiley & Sons; 2008. 56. Aveyard H. Doing a literature Review in Health and Social Care, a practical guide. USA: Open University Press; 2010. 57. Lamonte M, Blair S, Church T. Physical activity and diabetes prevention. Journal of Applied Physiology 2005; 99: 1205–1213. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 10 Journal of Diabetology, June 2012; 2:1 http://www.journalofdiabetology.org/ Appendix 1: Flow chart showing article search, inclusion criteria and selection process Search engine: PubMed and ISI web of knowledge Main Search terms: “Prevent* diabetes 2” AND “promote* physical activity” Refining the ISI research with: Academic journals, English language and public, environmental and occupational health as subject areas 418 articles were initially identified by Pub Med 110 articles were initially identified by ISI web of Knowledge ledge According to inclusion and exclusion criteria and after reading titles and abstracts 18 articles were potentially relevant from ISI web of Knowledge 38 articles were potentially selected from Pub Med 55 overall articles were potentially relevant from the two databases 8 articles were identified by snowballing (Pag e n u m b er n o t f o r cit at io n p u rp o ses) 19 articles were finally selected and met all the inclusion criteria Page 11 Journal of Diabetology, June 2012; 2:1 http://www.journalofdiabetology.org/ Appendix 2: Summary of the results of the final selected studies Author/date Aim of study Type of the study Main findings/conclusion Strengths and limitations Knowler et al., (2002) To assess the effectiveness of intensive lifestyle intervention (The US diabetes prevention program) in prevention of diabetes Randomized control trial Significantly lower incidence of diabetes cases and higher leisure time physical activity in the intervention group after an average of 2.8 years follow up. Representative sample There was a significant reduction in fasting plasma glucose in the intervention group during 2.8 years follow up. Diabetes Prevention Program Research Group et al., (2009) To assess the effectiveness of intensive lifestyle intervention (The US diabetes prevention program) against general lifestyle recommendations in prevention of diabetes Cohort study After 10 years follow up, the incidence rate did not differ significantly between the lifestyle intervention and the control group. However, the cumulative incidence rate (overall new diabetes cases over 10 years) of diabetes was the least in lifestyle intervention The mean of fasting glucose concentration in the lifestyle intervention was less than the control group (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 12 Good sample size (3234) Partly blinded study Unclear process of follow up including the number of participants who dropped out Exercises were assessed by self-reported questionnaire. This study was designed similar to (Knowler et al., 2002), but the follow up period was extended to 10 years. Possibility of other confounding factors as a result of long follow up period Journal of Diabetology, June 2012; 2:1 Allen et al., (2008) To evaluate lifestyle intervention which was conducted to prevent type 2 diabetes among American Indian women with impaired glucose tolerance http://www.journalofdiabetology.org/ Randomized control trial The mean change of fasting blood glucose was significantly reduced among participants (in comparison to baseline) after 6, 12 and 18 months follow up. Small sample size (42) Less prone to selection bias Exercise were assessed by self-reported questionnaire No significant improvement in the total leisure time physical activity during the same period. Thompson et al., (2008) Yang et al., (2009) To evaluate lifestyle intervention which was conducted to prevent type 2 diabetes among American Indian women with impaired glucose tolerance To evaluate the feasibility of 3 months yoga program in preventing type 2 diabetes for people at risk Randomized control trial (with 18 months follow up for American Indian women) No significant change in the mean of fasting blood glucose among participants during 6, 12 and 18 months follow up. A sample size of 200 Participants were randomized by tow computer generated lists Less prone to selection bias No significant improvement in the total leisure time physical activity and aerobic fitness (VO2) during the same period. Randomized control trial (with 3 months follow up) The intervention group showed improvement in exercise self-efficacy. No significant improvement in fasting glucose level. Exercise was assessed by self-reported questionnaire and aerobics fitness (VO2) Including subjects from different ethnicity Less prone to selection bias Small sample size (23) Unclear process of randomization The questionnaire which used for assessing exercise cannot be reliable in terms of measuring the change exercise practicing because it asses perceived self-efficacy to participate in physical activity (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 13 Journal of Diabetology, June 2012; 2:1 Yates et al., (2009) To evaluate the effectiveness of (PREPARE) program, which promote walking activity with or without pedometer, in improving impaired glucose tolerance http://www.journalofdiabetology.org/ Randomized control trial A structured education program with pedometer use (PREPARE) is effective in reducing fasting plasma glucose and 2 h glucose after one year follow up. Small sample size (87) More men than women participated Partly blinded study Short follow up period Clear process of randomization Physical activity was measured subjectively (by questionnaire) and objectively (by pedometer) Greaves et al., (2008) To assess the effectiveness of simplified intervention based on motivational interviewing, in changing weight and physical activity among people at high risk of diabetes. Randomized control trial A higher proportion of participants achieved the recommended physical activity (150 minute of moderate physical activity per week), but the difference was not significant, after 6 months follow up Small sample size (144) Partly blinded study Short follow up periods (6 months) Only included people who speak English fluently Exercise were assessed by self-reported questionnaire Yates et al., (2011) To evaluate the effectiveness of (PREPARE) program, which promote walking activity with or without pedometer, in improving impaired glucose tolerance (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Randomized control trial Page 14 A structured education program with pedometer use (PREPARE) is effective in reducing fasting glucose tolerance and 2 h glucose after 2 years follow up. No glucose measurement The study design is similar to that which was conducted by Yates et al., (2009) Journal of Diabetology, June 2012; 2:1 Tuomilehto et al., (2001) To assess the effect of exercise and dietary life style intervention (The Finnish diabetes prevention program) in preventing type 2 diabetes for people who are at risk. http://www.journalofdiabetology.org/ Randomized control trial The Finnish diabetes prevention program showed significant reduction in fasting plasma glucose and 2 h plasma glucose among the intervention group after one year follow up. Sample size of (523) Clear process of randomization Partly blinded study Exercise was assessed only by self-reported questionnaire Achieving the exercise goal (more than 4 hrs weekly) was significantly higher among the intervention group after one year follow up. The incidence of diabetes was lower and statistically significant in the intervention group than the control group after 2 years follow up. Lindström et al., (2003 a) To assess the effect of exercise and dietary life style intervention (The Finnish diabetes prevention program) in preventing type 2 diabetes for people who are at risk. (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Randomized trial Page 15 The Finnish diabetes prevention was effective in reducing fasting plasma glucose and 2 h plasma glucose only after one year (not after 3 years). In addition, it increased the level of moderate to vigorous leisure time physical activity after one and 3 years. The same design of Tuomilehto et al., (2001) The study showed results after 3 years follow up Journal of Diabetology, June 2012; 2:1 http://www.journalofdiabetology.org/ Lindström et al., (2003 b) To assess the effect of exercise and dietary life style intervention (The Finnish diabetes prevention program) in preventing type 2 diabetes for people who are at risk. Randomized control trial The Finnish diabetes prevention was effective in reducing diabetes risks such as fasting plasma glucose and 2 h plasma glucose after one and two years. In addition, achieving the physical activity goal was significantly higher among the intervention group after one year. The same design of Tuomilehto et al., (2001) Laaksonen et al., (2005) To assess the effect of exercise and dietary life style intervention (The Finnish diabetes prevention program) in preventing type 2 diabetes for people who are at risk. Randomized control trial Only moderate and vigorous in addition to strenuous structured physical activity showed significant difference among intervention group after an overall of 4 year follow up. The same design of Tuomilehto et al., (2001) To evaluate the effectiveness GOAL lifestyle intervention in prevention of type 2 diabetes Longitudinal pretest and posttest study design No improvements in fasting glucose and 2 hr oral glucose challenge after one year follow up. Prone to selection bias Absetz et al., (2007) The study provided detailed description of physical activity after longer period of follow up More female (265) than males (87) participated in the study Physical activity was assessed by selfreported questionnaire (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Page 16 Journal of Diabetology, June 2012; 2:1 Sartorelli et al., (2005) To evaluate the effectiveness of low cost lifestyle intervention in prevention of diabetes. http://www.journalofdiabetology.org/ Randomized control trial (with one year follow up) Only significant improvement in fasting plasma glucose after the first 6 months. No significant improvement in fasting plasma glucose after one year in addition to 2 h plasma glucose after 6 months and one year. No significant improvement in achieving the physical activity goal Laatikainen et al., (2007) Pan et al., (1997) To evaluate the feasibility of life style intervention which was conducted in Australian primary care in prevention of diabetes Longitudinal pretest and posttest study design To evaluate the effectiveness of diet and\or exercise intervention in reduction of the incidence of diabetes among people with impaired glucose tolerance. Randomized control trial Page 17 Exercise was assessed by self-reported questionnaire Partly blinded study Unclear process of randomization Large number of people lost during follow up Significant improvements in fasting glucose and 2 hr oral glucose challenge after one year follow up. Prone to selection bias Significant improvement in physical functioning after one year follow up After 6 years follow up, the incidence and cumulative incidence of diabetes was significantly lower in the intervention group, who received either diet or exercise or both, in comparison with the control group Physical activity was assessed by selfreported questionnaire Self-reported physical activity level was significantly higher in intervention groups (in comparison with baseline) (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Small sample size (104) More female (172) than males (65) participated in the study Good sample size (577) with long follow up period (6 years) Assessed the effect of physical activity alone in the reduction of diabetes cases Prone to selection bias Un clear process of randomization Journal of Diabetology, June 2012; 2:1 Ramachandran et al., (2006) Mensink et al., (2003) http://www.journalofdiabetology.org/ To assess the effectiveness of lifestyle intervention in reducing diabetes cases among Asian Indians with impaired glucose tolerance. Randomized control trial To assess the effect of diet and physical activity intervention (Dutch program) on glucose tolerance for people who are at risk of developing diabetes Randomized control trial The cumulative incidence of diabetes was significantly lower in the intervention groups Unclear process of randomization Blinding was not achieved The level of physical activity improved from baseline in both the lifestyle intervention group Page 18 More men (412) than women (110) participated in the study Only 2-h glucose was significantly lower in the intervention group after 2 years. Use of exercise test to measure physical activity Participants in the intervention group significantly improved their aerobic fitness. Prone to selection bias Subjects who received both diet and exercise intervention significantly improved their fasting insulin measures (2-h glucose was improved, but the improvement was not significant) (Pag e n u m b er n o t f o r cit at io n p u rp o ses) Sample size of (531) Small sample size (114) Partly blinded.