Instant Replay—A Quarterback`s View of Care Coordination
Anuncio

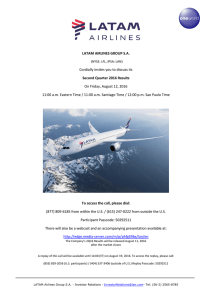
The NEW ENGLA ND JOURNAL of MEDICINE Perspective august 7, 2014 Instant Replay — A Quarterback’s View of Care Coordination Matthew J. Press, M.D. A s a general internist, I often serve as the quarterback for my patients’ care — helping them navigate the system, advocating on their behalf, and coordinating their evaluation and treatment. But for one of my patients, the game was played on a whole different level. Mr. K. was a stoic 70-year-old with a few minor medical problems. His care was fairly straightforward — I was the only doctor he saw regularly — until the day he came into my office with flank pain and fever. A CT scan of his abdomen revealed a kidney stone — and a 5-cm mass in his liver, which a subsequent MRI indicated was probably a cholangiocarcinoma. Over the 80 days between when I informed Mr. K. about the MRI result and when his tumor was resected, 11 other clinicians became involved in his care, and he had 5 procedures and 11 office visits (none of them with me). As the complexity of his care increased, the tasks involved in coordinating it multiplied. I kept a running list and, at the end, created an “instant replay” of Mr. K.’s care (see diagram; also see animation, available with the full text of this article at NEJM.org). In total, I communicated with the other clinicians 40 times (32 e-mails and 8 phone calls) and with Mr. K. or his wife 12 times. At least 1 communication occurred on 26 of the 80 days, and on the busiest day (day 32), 6 communications occurred. This instant replay offers a chronicle of the coordination that was required to help ensure that Mr. K.’s ambulatory care was delivered safely and effectively. Care coordination is now a high priority in health care and is the backbone of new models of care, such as accountable care organizations, that aim to improve quality and reduce costs. But it remains an abstract concept to many people who are not on the front lines of clinical care, as well as to some on the front lines who lack (or don’t want to have) the quarterback’s view of the field. In replaying the highlights, we can learn some important lessons about care coordination. The first is that care coordination is not just a value proposition (higher quality, lower costs) but a patient-safety issue. Patients can be harmed when the many moving parts of their care are out of sync.1 We owe it to them to coordinate the care we provide and n engl j med 371;6 nejm.org august 7, 2014 The New England Journal of Medicine Downloaded from nejm.org on November 20, 2016. For personal use only. No other uses without permission. Copyright © 2014 Massachusetts Medical Society. All rights reserved. 489 PERS PE C T IV E Instant Replay — a view of Care Coordination Phone call E-mail Procedure Office visit Surgeon Hematologist Neurologist Urologist PCP Patient Gastroenterologist Interventional radiologist Lab Social worker Oncologist Cardiologist Pathologist Ambulatory Care Coordination for One Patient. Over an 80-day period, 12 clinicians were involved in the care of the patient. The patient’s primary care physician (PCP) communicated with the other clinicians 40 times (32 e-mails and 8 phone calls) and with the patient (or his wife) 12 times. The patient underwent 5 procedures and had 11 office visits (none of them with his PCP). (An animated “instant replay” is available with the full text of this article at NEJM.org.) prevent this type of medical error. For example, on day 32 of Mr. K.’s care, a Friday, I noticed some new electrolyte abnormalities on laboratory tests done before an interventional radiology procedure. First I called the cardiologist who had seen Mr. K. earlier that week, after I learned from An animation the electronic medical is available at record (EMR) that he NEJM.org had prescribed a new antihypertensive. Then I called Mr. K. to arrange to have his electrolytes rechecked, which had to be done at an outside laboratory because by then it was the weekend (this took two calls to the laboratory — one to schedule and one for the results). On Sunday, I had Mr. K. change medications and on Monday asked the interventional radiology nurse practitioner to recheck the labs again before the procedure (two more calls). On day 490 36, she did, and the electrolytes had normalized. The second lesson is that the way we’ve viewed health care teamwork in the past (in single clinical settings, such as operating rooms, intensive care units, and primary care offices) needs an update. Given changes in the way health care is delivered and financed, teamwork today must encompass multiple clinical settings, where team members might not see or know each other. For example, on day 76 of Mr. K.’s care, I sent an e-mail to his urologist (cc-ing his surgeon) to alert him about kidney stones on a recent CT scan and about Mr. K.’s upcoming tumor resection. On day 79, the urologist let me know that he and the surgeon had communicated and made a plan to stage their procedures (first ureteral stent placement, then re- n engl j med 371;6 nejm.org section). Both procedures went smoothly on day 80, and Mr. K. did well postoperatively. Teamwork spanning health care settings is particularly challenging. Research from the field of organizational science has shown that conflict is greater within “distributed teams” than within co-located teams because their members are less familiar with one another and don’t necessarily have a shared context or shared norms.2 Overcoming these challenges requires a system designed to support and facilitate collaboration.3 Health information technology (e.g., shared EMRs and electronic messaging) is part of the solution (I used e-mail far more often than the phone), but it is not a panacea. Similarly, assigning care coordination to nonphysician staff members, such as care managers, is appropriate for some tasks and may benefit patients, but in many instances — including my e-mail to Mr. K.’s urologist and surgeon — communication must be physician to physician. Therefore, our workflow needs to be structured to allow time for communication with each other, and our reimbursement system should recognize the value of this aspect of care. I was able to play the role I did in Mr. K.’s care largely because, as a clinician-researcher, I had a patient panel about one tenth the size of the average primary care panel. The goal should be to make coordination and collaboration feasible for full-time clinicians, too.4 But even a perfectly designed system will not make up for one ingredient that’s essential to effective teamwork across care settings: relationships. Having a relationship with another clinician makes it easier to communicate because the social barrier is lower and august 7, 2014 The New England Journal of Medicine Downloaded from nejm.org on November 20, 2016. For personal use only. No other uses without permission. Copyright © 2014 Massachusetts Medical Society. All rights reserved. PE R S PE C T IV E opportunities to communicate are more frequent. But some changes in health care may be causing relationships to deteriorate. EMRs and the use of hospitalists probably have led to fewer personal interactions among physicians, and the consolidation of physician practices and changes in insurance participation can affect referral networks. I did not have relationships with most of Mr. K.’s other clinicians when his care began, so I reached out to them early and often to establish connections. I believe these connections instilled a sense of mutual accountability, helping to mitigate the potential for a bystander effect.5 Part of Instant Replay — a view of Care Coordination my job as quarterback is to make sure the other players know where the ball is and what routes each player is running. But everyone has to come to the huddle willingly. Fortunately, providing care collaboratively is more enjoyable than staying alone in our silos. I considered it a mark of successful teamwork when Mr. K.’s surgeon sent me an e-mail on day 80 saying, “Tumor is out!” No one knows for sure how Mr. K.’s case would have played out without effective care coordination. But this instant replay reveals that there is only one way for physicians to confront the perilous nature of complex care: together. Disclosure forms provided by the author are available with the full text of this article at NEJM.org. From the Departments of Healthcare Policy and Research and Medicine, Weill Cornell Medical College, New York. 1. Improving America’s hospitals: the Joint Commission’s annual report on quality and safety, 2007 (http://www.jointcommission .org/assets/1/6/2007_Annual_Report.pdf). 2. Hinds PJ, Bailey DE. Out of sight, out of sync: understanding conflict in distributed teams. Organization Sci 2003;14:615-32. 3. Press MJ, Michelow MD, MacPhail LH. Care coordination in accountable care organizations: moving beyond structure and incentives. Am J Manag Care 2012;18:778-80. 4. Bodenheimer T. Coordinating care — a perilous journey through the health care system. N Engl J Med 2008;358:1064-71. 5. Stavert RR, Lott JP. The bystander effect in medical care. N Engl J Med 2013;368:8-9. DOI: 10.1056/NEJMp1406033 Copyright © 2014 Massachusetts Medical Society. Toward Increased Adoption of Complex Care Management Clemens S. Hong, M.D., M.P.H., Melinda K. Abrams, M.S., and Timothy G. Ferris, M.D., M.P.H. M any observers of U.S. health care are now convinced that improved management of the care of patients with complex, high-cost conditions is an essential part of the solution to our health care cost problem. Increasing evidence supports the use of specially trained, primary care– integrated, complex care management (CCM) teams to improve outcomes and reduce costs by addressing the needs of the small proportion of patients who account for a majority of health care expenditures.1 For example, for successive cohorts of highrisk patients from 2006 through 2012, Massachusetts General Hospital achieved savings of 4%, 8%, and 19% by pursuing a CCM approach.2 CCM is a nearly universal element of the strategies used by providers accepting financial risk under Medicare’s account- able care organization contracts.3 Even as the momentum builds, however, substantial financial and nonfinancial barriers to more widespread adoption remain. The fee-for-service payment system is the most significant barrier to CCM adoption. CCM services are not easily separated into discrete, reimbursable units. Even when these services are disaggregated, most are not currently reimbursed. Providers, therefore, have little incentive to adopt CCM. In fact, when these programs are affiliated with hospitals, the fact that effective CCM reduces the rate of hospitalization creates a financial disincentive. Although it might be possible to pay for CCM on a fee-for-service basis, global-payment or shared-savings approaches that reward reductions in avoidable health care utilization are clearly preferable. Providers that are reimbursed through contracts that hold them accountable for costs of care (either total medical expenses or changes in total medical expenses) have an incentive to implement CCM. Many providers, however, remain unable to commit to such contracts. Fortunately, incremental payments used in conjunction with traditional fee-for-service systems can feasibly support CCM. In such a hybrid model, payers provide a care management fee (typically a per-member-per-month payment) to cover the costs of the CCM, and the provider is at risk only for the management fee. This approach provides an incentive to reduce avoidable use of services without requiring the provider to take on risk for the total costs of care for its patient population. Contracts under which providers take on risk for care n engl j med 371;6 nejm.org august 7, 2014 The New England Journal of Medicine Downloaded from nejm.org on November 20, 2016. For personal use only. No other uses without permission. Copyright © 2014 Massachusetts Medical Society. All rights reserved. 491