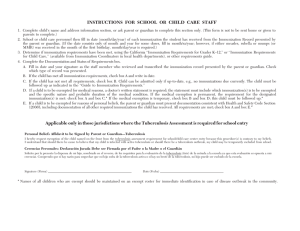
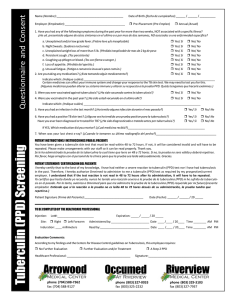
Articles Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data Lixia Wang*, Hui Zhang*, Yunzhou Ruan*, Daniel P Chin*, Yinyin Xia, Shiming Cheng, Mingting Chen, Yanlin Zhao, Shiwen Jiang, Xin Du, Guangxue He, Jun Li, Shengfen Wang, Wei Chen, Caihong Xu, Fei Huang, Xiaoqiu Liu, Yu Wang Summary Background China scaled up a tuberculosis control programme (based on the directly observed treatment, short-course [DOTS] strategy) to cover half the population during the 1990s, and to the entire population after 2000. We assessed the effect of the programme. Methods In this longitudinal analysis, we compared data from three national tuberculosis prevalence surveys done in 1990, 2000, and 2010. The 2010 survey screened 252 940 eligible individuals aged 15 years and older at 176 investigation points, chosen by stratified random sampling from all 31 mainland provinces. All individuals had chest radiographs taken. Those with abnormal radiographs, persistent cough, or both, were classified as having suspected tuberculosis. Tuberculosis was diagnosed by chest radiograph, sputum-smear microscopy, and culture. Trained staff interviewed each patient with tuberculosis. The 1990 and 2000 surveys were reanalysed and compared with the 2010 survey. Findings From 1990 to 2010, the prevalence of smear-positive tuberculosis decreased from 170 cases (95% CI 166–174) to 59 cases (49–72) per 100 000 population. During the 1990s, smear-positive prevalence fell only in the provinces with the DOTS programme; after 2000, prevalence decreased in all provinces. The percentage reduction in smear-positive prevalence was greater for the decade after 2000 than the decade before (57% vs 19%; p<0·0001). 70% of the total reduction in smear-positive prevalence (78 of 111 cases per 100 000 population) occurred after 2000. Of these cases, 68 (87%) were in known cases—ie, cases diagnosed with tuberculosis before the survey. Of the known cases, the proportion treated by the public health system (using the DOTS strategy) increased from 59 (15%) of 370 cases in 2000 to 79 (66%) of 123 cases in 2010, contributing to reduced proportions of treatment default (from 163 [43%] of 370 cases to 35 [22%] of 123 cases) and retreatment cases (from 312 [84%] of 374 cases to 48 [31%] of 137 cases; both p<0·0001). Interpretation In 20 years, China more than halved its tuberculosis prevalence. Marked improvement in tuberculosis treatment, driven by a major shift in treatment from hospitals to the public health centres (that implemented the DOTS strategy) was largely responsible for this epidemiological effect. Lancet 2014; 383: 2057–64 Published Online March 18, 2014 http://dx.doi.org/10.1016/ S0140-6736(13)62639-2 See Comment page 2026 *Authors contributed equally Chinese Center for Disease Control and Prevention, Beijing, China (L Wang MS, H Zhang PhD, Y Ruan PhD, Y Xia PhD, S Cheng BS, M Chen MS, Y Zhao PhD, S Jiang BS, X Du BS, G He PhD, J Li MS, S Wang PhD, W Chen PhD, C Xu MS, F Huang MS, X Liu MS, Y Wang MD); and China Office, The Bill & Melinda Gates Foundation, Beijing, China (D P Chin MD) Correspondence to: Dr Yu Wang, Chinese Center for Disease Control and Prevention, Beijing, 102206, China wangyu@chinacdc.cn Funding Chinese Ministry of Health. Introduction In 2010, China had an estimated 1 million new tuberculosis cases, accounting for 11% of global tuberculosis incidence.1 The country began to address its tuberculosis problem on a large scale in the 1990s when a tuberculosis control project, containing key elements of the internationally recommended directly observed treatment, short-course (DOTS) strategy (hereafter called the DOTS programme), was implemented in 13 provinces containing half the country’s population.2 Two national surveys of the prevalence of tuberculosis— done in 1990 and 2000—showed a 30% increased reduction in tuberculosis prevalence in areas that implemented this project.3 However, the national tuberculosis prevalence fell by less than 20% in 10 years;3 this slight reduction could be because, at its peak, the project treated only 30% of the estimated new smearpositive tuberculosis cases in the country.4 To accelerate the national tuberculosis control effort, the State Council of China issued a new 10-year tuberculosis control plan in 2001, which expanded the DOTS programme to the entire country by 2005. A previous www.thelancet.com Vol 383 June 14, 2014 report detailed the measures developed and implemented by the government to increase the number of tuberculosis patients treated in the DOTS programme.5 Through these efforts, China achieved the 2005 global tuberculosis control targets of detecting at least 70% of all estimated new smear-positive tuberculosis cases and successfully treating more than 85% of these patients—the only country with a high tuberculosis burden to achieve this.1,6 To re-evaluate China’s tuberculosis burden, a national tuberculosis prevalence survey was done in 2010. We report the main findings of the latest survey and compare the results with those from the 1990 and 2000 surveys;7,8 this analysis allowed us to assess the effects of 20 years of tuberculosis control. Methods Survey design We undertook a longitudinal analysis of data from 1990, 2000, and 2010 national tuberculosis prevalence surveys in China. For the 2010 survey, we used multistage, stratified sampling to randomly select 176 investigation points from within the 31 mainland provinces, municipalities, and 2057 Articles autonomous regions (hereafter termed provinces). We sampled urban and rural sites separately to ensure the survey had 77 urban and 99 rural investigation points, in line with the urban:rural ratio of the national population. All people aged 15 years or older and a local resident (defined as residing in the survey area for at least 6 months) were eligible for the survey. Each investigation point averaged 1503 people. The survey was done from April, 2010, to July, 2010. The survey design is consistent with global guidelines.9 The study was reviewed and approved by the Tuberculosis Operational Research Ethics Review Committee of Chinese Ministry of Health; the need for individual informed consent was waived by the committee. Patients and procedures All participants had chest radiographs taken. Those with cough for greater than 2 weeks or haemoptysis were classified as having symptoms of tuberculosis (figure 1). We collected sputum from individuals with any of the four following characteristics: tuberculosis symptoms, an abnormal chest radiograph, a diagnosis of tuberculosis before the survey, and a pregnant woman or person with restricted mobility who were not examined by chest radiography. Three sputum specimens (spot, night, and morning) were collected for smear microscopy and two specimens were cultured on Löwenstein–Jensen medium. The selection of specimens for culture was based on the level of smear positivity and appearance. Individuals 15 years or older, resident at investigation point Clinical history/chest x-ray Abnormal chest radiograph or tuberculosis symptoms Known tuberculosis patient Pregnant women or individuals with restricted mobility (no chest radiograph) Normal chest radiograph and no tuberculosis symptoms Sputum smear and culture Positive smear and negative culture Mycobacterium tuberculosis Positive culture ± positive smear Non-tuberculous mycobacteria Negative smear and culture Expert panel re-read chest radiograph A positive smear had at least one acid-fast bacillus identified during examination of 100 fields. Slides were reviewed by a central team of experts, and only those identified as positive on both initial and repeat examinations were classified as positive. A positive culture had at least one colony of Mycobacterium tuberculosis complex isolated. Bacteriologically positive cases were those with at least one positive smear or culture. Smear and culture were done at a tuberculosis laboratory in either the city or county closest to the investigation site. These laboratories had technicians trained to undertake tuberculosis testing according to national guidelines and participated in internal and external quality assurance programmes for smear microscopy. During the survey period, a provincial tuberculosis reference laboratory closely monitored the quality of the sputum culture and provided assistance to laboratories whenever culture contamination exceeded 5% or the percentage of negative culture in the smearpositive specimens exceeded 10%. Cultures with growing colonies were sent to the National Tuberculosis Reference Laboratory for identification. Patients with active tuberculosis included those with bacteriologically-positive sputum and those diagnosed only by changes on their chest radiographs. Therefore, individuals with active tuberculosis included patients with smear-positive and culture-negative sputum, smearnegative but culture-positive sputum, and smear-negative and culture-negative sputum. Survey staff were trained to diagnose active tuberculosis cases on the basis of patient symptoms and clinical history, radiographic findings, bacteriological results, and response to antibiotics, in accordance with national guidelines. A national expert group reviewed the data from each patient to confirm the diagnosis. Newly identified cases were separated from known, or previously diagnosed, cases that were still active at the time of the survey. The sampling approach and the clinical and laboratory methods for diagnosis of tuberculosis in the 2010 survey were the same as those used in the 1990 and 2000 surveys, but were done at different investigation sites and by different survey teams than those in 2010. Trained staff administered a standard questionnaire to every person with tuberculosis. People with a previous diagnosis of tuberculosis, were classified as known cases and were asked questions about their past and present diagnosis and treatment. For the known cases, we checked the tuberculosis registry of the public health system to establish whether the patient had been reported to, and registered in, the Chinese Center for Disease Control and Prevention (CDC) system. Previous surveys Tuberculosis Figure 1: Diagnostic algorithm used during the 2010 prevalence survey 2058 Not tuberculosis Although the 1990 and 2000 surveys had similar designs, they differed in some areas.7,8 First, both the 1990 and 2000 surveys included testing for individuals aged www.thelancet.com Vol 383 June 14, 2014 Articles Prevalence per 100 000 population Change (%)* 1990 2000† 2010† 1990–2000 2000–2010 1990–2010 All pulmonary 611 (603 to 619) 414 (390 to 439) 442 (417 to 469) –32% (–36 to –28) 7% (–2 to 16) –28% (–32 to –23) Bacteriologically positive 221 (216 to 226) 178 (163 to 195) 116 (101 to 132) –19% (–27 to –12) –35% (–45 to –23) –48% (–55 to –40) Smear positive 170 (166 to 174) 137 (123 to 153) 59 (49 to 72) –19% (–28 to –10) –57% (–66 to –46) –65% (–72 to –58) All provinces Provinces that implemented DOTS in 1990s‡ All pulmonary 665 (653 to 677) 364 (335 to 395) 462 (423 to 505) –45% (–50 to –40) 27% (12 to 44) –31% (–37 to –24) Bacteriologically positive 239 (232 to 246) 154 (135 to 174) 110 (93 to 130) –36% (–44 to –27) –29% (–43 to –12) –54% (–62 to –46) Smear positive 176 (170 to 182) 113 (96 to 133) 63 (50 to 80) –36% (–46 to –24) –44% (–59 to –26) –64% (–72 to –55) Provinces that implemented DOTS after 2000‡ All pulmonary 663 (652 to 674) 499 (459 to 542) 443 (411 to 478) –25% (–31 to –18) –11% (–21 to 0) –33% (–38 to –28) Bacteriologically positive 225 (219 to 231) 219 (194 to 248) 124 (101 to 152) –3% (–15 to 10) –43% (–56 to –28) –45% (–56 to –33) Smear positive 180 (174 to 186) 174 (151 to 201) 59 (43 to 79) –3% (–17 to 12) –66% (–76 to –53) –67% (–77 to –56) Data are mean (95% CI) for individuals aged 15 years and older. DOTS=direct observed treatment, short-course. *Negative values show decrease in prevalence. †Data analysed with 1990 diagnostic protocol, except chest radiograph used in initial screening instead of fluoroscopy in 2010; results unstandardised for age or other variables. ‡Provinces that implemented DOTS in 1990s include Chongqing, Gansu, Guangdong, Hainan, Hebei, Heilongjiang, Hubei, Hunan, Liaoning, Ningxia, Shandong, Sichuan, and Xinjiang; provinces that implemented DOTS after 2000 include Anhui, Fujian, Guangxi, Guizhou, Henan, Jiangsu, Jiangxi, Jilin, Neimeng, Qinghai, Shaanxi, Shanxi, Tibet, Yunnan, and Zhejiang. The three municipalities of Beijing, Shanghai, and Tianjin are excluded from this analysis because, for more than 30 years, they have had high economic development, substantial expertise in tuberculosis control, and organised tuberculosis control programmes similar to the DOTS programme. Table 1: Comparison of tuberculosis prevalence over time in provinces that implemented DOTS in 1990s and after 2000 younger than 15 years; the 2010 survey did not do this. In this study, we reanalysed the 1990 and 2000 surveys with only results from individuals aged 15 years or older. Second, chest fluoroscopy was used to screen individuals in 1990 and 2000; chest radiographs were used in 2010. Third, in 1990, only symptomatic individuals were examined by chest fluoroscopy and asked to provide sputum if the fluoroscopic examination was abnormal. In 2000 and 2010, individuals with tuberculosis symptoms but normal fluoroscopic examinations (or normal chest radiographs) were also asked to provide sputum. Finally, in 1990, two sputum smears were used instead of three, and in both 1990 and 2000 only one specimen was cultured. The diagnostic protocol used in 2000 was therefore more sensitive than that used in 1990, and the protocol used in 2010 was more sensitive than that used in 2000. For comparisons involving all three surveys, we calculated prevalences according to the 1990 diagnostic protocol. With this protocol, only individuals with tuberculosis symptoms were further assessed. In symptomatic patients with abnormal radiographic examination, we used the results of two sputum smears and one culture to establish each patient’s bacteriological status. For comparisons involving only the 2000 and 2010 surveys, we used the 2000 diagnostic protocol. This protocol differed from the 1990 protocol in only one aspect: three sputum smears were used instead of two. Statistical analysis The survey was designed to detect an annual decline of 3·2% in national prevalence of smear-positive tuberculosis between 2000 and 2010 with a probability of www.thelancet.com Vol 383 June 14, 2014 greater than 95% and power of 95%. This rate of decline was observed in areas implementing the DOTS strategy from 1990 to 2000.3 We calculated the sample size to be 264 630 with simple random sampling, a design effect of 1·8 from the 2000 survey, and 90% participation rate. Although the survey was not designed a priori to compare subpopulations within China, we stratified the data in several ways: sex, age, urbanisation (urban and rural), region (western, central, and eastern parts of the country), and provinces that implemented the DOTS programme in the 1990s and after 2000. We calculated the overall prevalence rates and the stratum-specific rates for various subpopulations and analysed patient information using the complex survey module in SPSS Statistics 17.0. This module takes into account the clustered sampling design of the survey. CIs were adjusted for the cluster design by the Taylor series linearisation. When comparing prevalences in different subpopulations and over time, we adjusted p values using the second-order correction of Rao–Scott for the χ² test. The difference or change in prevalence was assumed to follow a beta distribution. Two shape parameters needed to define the β distribution were computed using the method of moments. The upper and lower 2·5% of the resulting distribution were used to determine the 95% CI. We did these computations using R statistical package (2.15.1). Role of the funding source The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The Chinese CDC operates under the general guidance of the Ministry and was responsible for the design, implementation, and analysis of the 2010 2059 Articles survey. LW, HZ, YR, YX, and DPC had complete access to the data and were responsible for submitting the Article for publication. Results Of 263 281 individuals eligible in 2010, 252 940 (96%) participated in the survey, 4541 (2%) refused to participate, 3709 (1%) were not at the investigation site during the survey, and 2091 (1%) did not participate for other reasons. Of 9825 people eligible for sputum examination, 9716 (99%) had examination results, and 109 (1%) did not submit sputum samples. With the 2010 diagnostic protocol, 1310 cases of active pulmonary tuberculosis were detected, of which 347 were bacteriologically positive (119 per 100 000 population; 95% CI 103–135) and 188 were sputum smear-positive (66 per 100 000 population; 95% CI 53–79). From 1990 to 2010, smear-positive prevalence fell by 65%, bacteriologically positive prevalence declined by 48%, and prevalence of all pulmonary cases declined by 28% (table 1). 70% of the reduction in smearpositive prevalence and 59% of the reduction in bacteriologically-positive prevalence occurred after 2000. Smear-positive prevalence (per 100 000 population) 250 New cases Known cases From 1990 to 2000, provinces that implemented the DOTS programme had a significant reduction in the prevalence of smear-positive and bacteriologically positive tuberculosis cases; other provinces did not have this reduction (table 1). From 2000 to 2010, these prevalences decreased in both groups of provinces, reaching roughly the same level by 2010; this resulted from a greater (although not statistically significant) reduction in provinces that implemented DOTS after 2000. The reduction in prevalence of smear-positive and bacteriologically positive tuberculosis cases was largely due to a reduction in the prevalence of known cases (figure 2). From 2000 to 2010, the prevalence of smearpositive tuberculosis among known cases decreased by 88% (from 77 to 9 per 100 000 population). This decrease accounted for 87% of the total reduction in smear-positive prevalence (68 of 78 per 100 000 population). From 2000 to 2010, the prevalence of bacteriologically positive tuberculosis decreased significantly in all subpopulations examined, including men, women, all age groups, urban and rural areas, and all regions except western China (table 2). The reduction in prevalence was significantly less in western than in eastern China (p=0·0026), but not significantly different between strata in other subpopulations. 200 Prevalence per 100 000 population* 150 100 Change, 2000–2010 (%)† 2000 2010 Male 304 (275 to 337) 183 (157 to 215) –40% (–51 to –27) Female 115 (96 to 139) 64 (52 to 79) –44% (–58 to –26) Sex 50 Age group (years) 0 Bacteriologically positive prevalence (per 100 000 population) 250 200 92 (72 to 116) 59 (40 to 86) –36% (–61 to 0) 30–44 119 (96 to 146) 73 (54 to 99) –39% (–59 to –11) 45–59 213 (174 to 260) 133 (106 to 168) –38% (–55 to –15) ≥60 596 (510 to 698) 346 (294 to 407) –42% (–54 to –27) Urbanisation 150 Urban 152 (115 to 202) Rural 225 (206 to 246) 163 (143 to 185) 73 (51 to 105) –52% (–71 to –23) –28% (–38 to –15) Region‡ 100 50 0 1990 2000 Year 2010 Figure 2: Prevalence of smear-positive and bacteriologically positive tuberculosis stratified by new and known cases, 1990–2010 Analysed by use of 1990 diagnostic protocol and unstandardised for age or other variables. Error bars show the 95% CI. Prevalence of smear-positive or bacteriologically positive tuberculosis in known cases was significantly lower in 2010 than in 1990 or 2000. Prevalence of smear-positive tuberculosis in new cases was significantly lower in 2010 than in 1990; this difference is not seen in bacteriologically positive new cases. 2060 15–29 Eastern 158 (137 to 183) 66 (52 to 84) –58% (–69 to –45) Central 241 (203 to 285) 124 (92 to 166) –49% (–64 to –28) Western 262 (228 to 302) 212 (180 to 249) –19% (–35 to 1) Data are mean (95% CI) for individuals aged 15 years and older. *Data analysed with 2000 diagnostic protocol, except chest radiograph used in initial screening instead of fluoroscopy in 2010, and unstandardised for age or other variables. †Negative values show decrease in prevalence. ‡Eastern provinces include Beijing, Fujian, Guangdong, Hainan, Heibei, Jiangsu, Liaoning, Shandong, Shanghai, Tianjin, and Zhejiang; central provinces include Anhui, Heilongjiang, Henan, Hunan, Hubei, Jiangxi, Jilin, and Shanxi; western provinces include Chongqing, Gansu, Guangxi, Guizhou, Neimeng, Ningxia, Qinghai, Shaanxi, Sichuan, Tibet, Xinjiang, and Yunnan. Table 2: Change in the prevalence of bacteriologically positive tuberculosis in subpopulations, 2000 and 2010 www.thelancet.com Vol 383 June 14, 2014 Articles Hospitals Cases classified by where they were diagnosed Reported and registered in CDC system CDC 2000 2010 329 77 50 (15%) 34 (50%) p value ·· <0·0001 All institutions 2000 2010 45 60 43 (95%) 56 (95% p value ·· 0·6948 2000 2010 374 137 93 (23%) 90 (69%) p value ·· <0·0001 Classified as retreatment case during most recent diagnosis 281 (86% 30 (33%) <0·0001 31 (67%) 18 (28%) <0·0001 312 (84%) 48 (31%) <0·0001 Started tuberculosis treatment after recent diagnosis 325 (99%) 66 (87%) <0·0001 45 (100%) 57 (96%) <0·0001 370 (99%) 123 (91%) <0·0001 311 44 59 79 370 123 Cases started on treatment classified by where they were treated* Regularity of drug intake‡ ·· <0·0001 ·· <0·0001 ·· <0·0001 Regular 62 (21%) 14 (41%) ·· 36 (57%) 59 (82%) ·· 98 (26%) 73 (68%) ·· Intermittent (on and off) 99 (34%) 9 (17%) ·· 10 (17%) 6 (7%) ·· 109 (31%) 15 (10%) ·· Defaulted from treatment 150 (46%) 21 (42%) ·· 13 (26%) 14 (12%) ·· 163 (43%) 35 (22%) Reasons for defaulting from treatment‡ 0·0335 0·0002 ·· <0·0001 Felt better, self discontinued 69 (45%) 13 (60%) ·· 3 (20%) 3 (22%) ·· 72 (42%) 16 (47%) ·· Financial difficulties 65 (45%) 3 (17%) ·· 6 (46%) 1 (11%) ·· 71 (45%) 4 (15%) ·· 6 (5%) 2 (8%) ·· 0 (0%) 8 (57%) ·· 6 (4%) 10 (25%) ·· 10 (6%) 3 (14%) ·· 4 (33%) 2 (9%) ·· 14 (8%) 5 (13%) ·· Side-effects Others Data are N or n (%). CDC=Centers for Disease Control. Calculation of percentages takes into account the multistage, stratified sampling design, therefore the percentages presented in the table might not be reproducible simply from data in the table. *Few patients were not treated in the type of institution where they were diagnosed. ‡Denominator for regularity of drug intake is the number of patients started on treatment; denominator for reasons for defaulting is the number of patients defaulted from treatment. Table 3: Reporting and treatment of previously diagnosed tuberculosis cases by where patients were diagnosed and treated, 2000 and 2010 From 2000 to 2010, substantial programmatic improvements occurred. More patients were reported to, and registered with, the CDC system. The percentage of patients defaulting from treatment decreased from 43% (163 of 370) to 22% (35 of 123), and the percentage of retreatment cases decreased from 84% (312 of 374) to 31% (48 of 137; both p<0·0001). This resulted from an increase in the proportion of patients treated by the CDC system and, to a lesser extent, from treatment improvement in both the CDC and the hospital systems (table 3). Among known cases, the proportion treated by the CDC system (using the DOTS strategy) increased from 59 (15%) of 370 in 2000 to 79 (66%) of 123 in 2010. However, in 2010, half of the patients diagnosed in the hospital system still had not been reported to the CDC and nearly half of those treated by hospitals had defaulted from treatment. The programmatic improvements from 1990 to 2000 were fairly minor. The proportion of tuberculosis cases reported to the CDC system increased from 460 (19%) of 2453 to 93 (23%) of 374 (p=0·0055); the proportion of patients who received tuberculosis treatment increased from 2313 (94%) of 2453 to 370 (99%) of 374 (p=0·00014), and the proportion of patients who defaulted from treatment decreased from 1118 (51%) of 2202 to 163 (43%) of 370 (p=0·0168). Calculation of the above percentages took into account the sampling design and therefore might not be reproducible simply from the numbers presented. Discussion From 1990 to 2010, for individuals aged 15 years and older in China, the prevalence of smear-positive tuberculosis fell by 65% and the prevalence of bacteriologically positive tuberculosis fell by 48% (panel). By 2010, China had thus achieved one of the key global www.thelancet.com Vol 383 June 14, 2014 tuberculosis targets set by the Stop TB Partnership: to reduce the prevalence of smear-positive tuberculosis by 50%.6 This reduction was achieved 5 years before the target date of 2015. This analysis did not include data from individuals younger than 15 years; however, the absence of such data is unlikely to change the major findings because less than 2% of laboratory confirmed tuberculosis cases come from this age group.7,8 The reduction in tuberculosis prevalence occurred concurrently with the scale-up of the DOTS programme in China. This scale-up, which was implemented by the CDC system through its local public health clinics, occurred in two distinct phases. During the 1990s, the country expanded the DOTS programme to cover half of its population, and increased the tuberculosis case detection rate—the percentage of all estimated new smear-positive tuberculosis patients detected—to roughly 30%.1,5 Concurrently, the prevalence of smear-positive tuberculosis fell by 19%. From 2001 to 2005, China scaled up the DOTS programme nationwide and used a series of public health interventions to increase the tuberculosis case detection rate to nearly 80%.5 The prevalence of smear-positive tuberculosis fell by 57% for the decade after 2000—tripling the reduction of the previous decade. 70% of the absolute reduction in smear-positive prevalence in two decades occurred during the second decade when tuberculosis control efforts intensified. Even though the prevalence of smear-positive tuberculosis decreased significantly during the 1990s, the change was only seen in areas of China where the DOTS programme was implemented. After adjustments for changing age structure and other factors, a previous analysis attributed a 30% reduction in tuberculosis prevalence to the DOTS programme,3 supporting a 2061 Articles Panel: Research in context Systematic review We searched PubMed from Jan 1, 1995, to Aug 31, 2013, for English publications that measured tuberculosis prevalence at a national level. We used the search terms “tuberculosis” and “prevalence”. We included studies with serial national tuberculosis prevalence surveys, which allowed an assessment of changes in tuberculosis prevalence with time. Studies with subnational data that were not representative of the entire country were not included. We identified only two studies—from China and the Philippines—that contained data from serial national tuberculosis prevalence surveys during the period when the directly observed treatment, short-course (DOTS) strategy was being implemented.3,10 Interpretation Aside from China, no other country with high burden of tuberculosis has done more than two tuberculosis prevalence surveys during the period when the DOTS strategy was being implemented. The Philippines is the only other high tuberculosis-burden country with more than one survey. After 10 years of DOTS implementation, the second Philippines survey showed a 31% reduction in prevalence of bacteriologically positive tuberculosis and a 27% reduction in prevalence of smear-positive tuberculosis.9 However, the decrease in smear-positive prevalence was not significant. One of the key global tuberculosis targets aims to reduce tuberculosis prevalence by 50% between 1990 and 2015. This study in China is the first to show the feasibility of achieving such a target, and China achieved this 5 years earlier than the target date. In fact, China achieved a 57% reduction in prevalence of smear-positive tuberculosis from 2000 to 2010—a mere 10 years, coincident with a massive scale up of the DOTS programme. Additionally, the study linked the epidemiological effect to huge improvements in tuberculosis treatment at a population level, showing the importance of addressing of poor tuberculosis treatment in the hospital system. causal llinkage between DOTS implementation and reduced tuberculosis prevalence; however, information from the two most recent surveys provides even stronger support for this link. A national tuberculosis prevalence survey can identify an unbiased, cross-sectional sample of existing tuberculosis patients in a country, including those with a previous diagnosis of tuberculosis—ie, known cases at time of survey. By collecting information on the status of their tuberculosis treatment, we can learn about the quality of treatment at a population level. More than 40% of all patients known to have tuberculosis in the 2000 survey had defaulted from their treatment. More than 80% of these known patients were treated by the hospital system and, of those, half had defaulted from their treatment. The 2010 survey identified substantial improvements in tuberculosis treatment. Compared with the 2000 survey, an increased percentage of known patients were taking their drugs regularly and a reduced percentage of patients had defaulted from treatment. Notably, the percentage of known patients with one or more previous courses of treatment for tuberculosis—an indicator of poor treatment quality—decreased from more than 80% to around 30%. After 2000, two major changes played an important part in improving tuberculosis treatment. First, the government 2062 expanded the DOTS programme nationwide, providing standard short-course chemotherapy throughout the country’s network of local CDC.5 Second, the DOTS programme expanded its free treatment policy to all patients with active pulmonary tuberculosis.5 Before 2000, when the free treatment policy applied only to smearpositive cases, an estimated 30% of new smear-positive cases were treated in the DOTS programme. These patients corresponded roughly to 15% of all patients with tuberculosis—the percentage identified in the 2000 survey. The expansion of free treatment allowed many more patients to access the CDC for treatment. With these two changes, the percentage of patients treated by the CDC system increased from 15% in 2000 to 66% in 2010. Without these changes, most patients would have continued to access the hospital system for treatment, but only a small proportion of those treated would have continued their treatment. This shift in where patients were treated—from hospitals to the CDCs—accounted for most of the treatment improvement for the entire patient population. Improved tuberculosis reporting and referral by hospitals to the CDC system, coupled with active follow-up by the CDC system, helped with this shift.11,12 The population-based improvements in tuberculosis treatment can be directly linked to the reduction in tuberculosis prevalence. Nearly all the decrease in tuberculosis prevalence was due to a reduction in the prevalence of tuberculosis among known cases—ie, cases already diagnosed before the survey. A decrease in disease prevalence can result from a reduced disease incidence, or duration of illness, or both. If the 90% reduction in prevalence in known cases was primarily due to decreased tuberculosis incidence, then one would expect to see a similar reduction in prevalence among new cases; but this reduction did not happen. Therefore, a substantial shortening in the duration of illness after tuberculosis diagnosis—a result of more effective tuberculosis treatment—must have played an important part in reducing the prevalence among known cases. This study provides insights into how the country can further reduce its tuberculosis burden. First, increased focus should be placed on western China because this region has the highest prevalence of tuberculosis and is lagging behind in reducing its tuberculosis burden.3,7,8 Our study showed that, between 2000 and 2010, the decrease in prevalence of bacteriologically positive tuberculosis—measured in both absolute and percentage changes—was greater in the eastern-central region than in the western region. As a result, the gap between nonwestern and western areas in tuberculosis prevalence has widened. Rural areas have consistently higher tuberculosis prevalence than urban areas,3,7,8 and we see a similar trend toward a widening urban–rural gap in tuberculosis prevalence although this finding is not significant. With slower economic development, these lagging areas have less financial resources, fewer well www.thelancet.com Vol 383 June 14, 2014 Articles trained health-care workers, and weaker public health infrastructure to address a problem such as tuberculosis. Increased governmental inputs are needed to improve tuberculosis control efforts in these areas. Second, the reporting and treatment of patients with tuberculosis in the hospital system should be improved. In 2010, fewer than half of the cases diagnosed in hospitals were reported to, and registered in, the CDC system, and only 41% of patients started on treatment in hospitals were taking their drugs regularly when in the community. Furthermore, use of improper treatment regimens in hospitals is widespread.13 Third, the DOTS programme has been much more effective in reducing the prevalence of tuberculosis in known cases than in new cases. Because the prevalence in known cases is already very low, future reduction in tuberculosis prevalence is likely to slow substantially unless control efforts in addition to the DOTS strategy are implemented, especially in earlier case detection and treatment and use of new instruments.14,15 Future studies can help to identify populations at high risk of tuberculosis and assess the feasibility and effectiveness of active case-finding or preventive treatment. China already has a policy to screen individuals with HIV for tuberculosis, and the use of preventive treatment is being evaluated. Although more should be done to prevent HIV-associated tuberculosis, such efforts will not have a major effect on the overall reduction in tuberculosis prevalence given the fairly small and concentrated HIV epidemic in the country.16,17 An intriguing finding is the absence of reduction in the prevalence of all pulmonary cases between 2000 and 2010. We believe this absence is due to the use of chest radiography as the initial screening instrument in 2010 instead of chest fluoroscopy in the earlier surveys. This change in instrument probably increased the sensitivity of case detection in 2010, thus masking any real decrease in the prevalence of pulmonary cases. There are several limitations to our study. First, chest radiographs were used to screen the survey population in 2010, whereas fluoroscopy was used in earlier surveys. The 2010 survey was therefore more sensitive in identifying patients with tuberculosis. However, the reductions in this study would have been greater if fluoroscopy had been used in 2010 instead of chest radiographs. Second, we excluded individuals younger than 15 years from this analysis. Because the proportion of the Chinese population in this age group has been decreasing, to include them in our analysis would have reduced (albeit by a very small amount) the decrease of tuberculosis prevalence in the entire population. Third, socioeconomic development probably contributed to the reduction in tuberculosis prevalence, but its effects cannot be distinguished from tuberculosis control efforts. However, its contribution was unlikely to have varied greatly with time because the annual growth in gross domestic product per head adjusted for purchasing www.thelancet.com Vol 383 June 14, 2014 power parity was 10% between 1990 and 2000 and 11% between 2000 and 2010. During this 20 years of steady economic growth, the observed correlation between intensity of tuberculosis control efforts and greater reduction in tuberculosis prevalence supports a causal linkage between the two. Finally, our results have implications for the present discussion about a new agenda for global tuberculosis control and elimination after the UN Millennium Development Goals expire in 2015.18–22 Of the new tuberculosis targets that will probably be considered by the World Health Assembly is a 50% reduction in tuberculosis incidence between 2015 and 2025. Achievement of such a target would be an important milestone toward tuberculosis elimination. Our results show the feasibility of such a target when a programme is put into place to substantially improve the quality of tuberculosis treatment. Countries can achieve this improvement with an aggressive scale-up of the DOTS programme if they have not done so already, but improvement of the treatment of patients diagnosed outside the DOTS programme, which is usually implemented only in the public sector, is essential. However, because many developing countries— including those with the highest tuberculosis burden— have already improved tuberculosis treatment in the past 10–15 years using the DOTS strategy, long-term, rapid reduction in the tuberculosis burden will need additional control efforts. These efforts include earlier detection and treatment of active tuberculosis and ultimately interventions and new instruments to reduce the risk of tuberculosis in the large global population with latent tuberculosis infection. For more on World Bank GDP per capita see http://data. worldbank.org/indicator/NY. GDP.PCAP.CD Contributors YW, LW, HZ, YR, SC, MC, YZ, SJ, XD, GH, and DPC participated in the design and planning of the study. JL, SW, WC, CX, FH, and XL collected the data. LW, HZ, YR, YX, DPC, and YW did the data analysis and prepared the report for publication. Declaration of interests We declare that we have no competing interests. Acknowledgments We thank members of the National Tuberculosis Epidemiological Investigation Steering Group (especially Yude Chen, Xiexiu Wang, Shuigao Jin, and Liya Wan), Ikushi Onozaki of the World Health Organization, and Zhongwei Jia of the Peking University Health Science Center for their valuable advice and assistance during the design or analysis of the 2010 National Tuberculosis Prevalence Survey. We also thank the tireless contributions of staff in the Ministry of Health, provincial health bureaus, provincial CDCs, and local CDCs in undertaking the tuberculosis prevalence surveys. References 1 Global tuberculosis control: WHO report 2011. Geneva: World Health Organization, 2011. 2 China Tuberculosis Control Collaboration. Results of directly observed short-course chemotherapy in 112 842 Chinese patients with smear-positive tuberculosis. Lancet 1996; 347: 358–62. 3 China Tuberculosis Control Collaboration. The effect of tuberculosis control in China. Lancet 2004; 364: 417–22. 4 Chen X, Zhao F, Duanmu H, et al. The DOTS strategy in China: results and lessons after 10 years. Bull World Health Organ 2002; 80: 430–36. 2063 Articles 5 6 7 8 9 10 11 12 13 2064 Wang L, Liu J, Chin DP. Progress in tuberculosis control and the evolving public-health system in China. Lancet 2007; 369: 691–96. Dye C, Maher D, Weil D, Espinal M, Raviglione M. Targets for global tuberculosis control. Int Tuberc Lung Dis 2006; 10: 460–62. Ministry of Public Health of the People’s Republic of China. Nationwide random survey for the epidemiology of tuberculosis in 1990. Beijing: Ministry of Public Health of the People’s Republic of China, 1990. Ministry of Public Health of the People’s Republic of China. Report on nationwide random survey for the epidemiology of tuberculosis in 2000. Beijing: Ministry of Public Health of the People’s Republic of China, 2000. WHO. Assessing tuberculosis prevalence through population-based surveys. Geneva: World Health Organization, 2007. Tupasi TE, Radhakrishna S, Chua JA, et al. Significant decline in the tuberculosis burden in the Philippines ten years after initiating DOTS. Int J Tuberc Lung Dis 2009; 13: 1224–30. Wang L, Cheng S, Xu M, et al. Model collaboration between hospitals and public health system to improve tuberculosis control in China. Int J Tuberc Lung Dis 2009; 13: 1486–92. Wan L, Cheng S, Chin DP, et al. A new disease reporting system and increases tuberculosis case detection in China. Bull World Health Organ 2007; 85: 401. He GX, van den Hof S, van der Werf MJ, et al. Inappropriate tuberculosis treatment regimens in Chinese tuberculosis hospitals. Clin Infect Dis 2011; 52: 153–56. 14 15 16 17 18 19 20 21 22 Raviglione M, Marais B, Floyd K, et al. Scaling up interventions to achieve global tuberculosis control: progress and new developments. Lancet 2012; 379: 1902–13. Li Y, Ehiri J, Tang S, et al. Factors associated with patient, and diagnostic delays in Chinese TB patients: a systematic review and meta-analysis. BMC Med 2013; 11: 156–170. UNAIDS. 2012 China AIDS response progress report. http://unaids. org.cn/pics/20120614140133.pdf (accessed Dec 1, 2013). Wu Z, Sullivan SG, Wang Y, Rotheram-Borus M, Detels R. Evolution of China’s response to HIV/AIDS. Lancet 2007; 369: 679–90. Lönnroth K, Castro KG, Chakaya JM, et al. Tuberculosis control and elimination 2010-50: cure, care, and social development. Lancet 2010; 375: 1814–29. Dye C, Raviglione M. Weigh all TB risks. Nature 2013; 502: S13. WHO. Developing the post-2015 TB strategy and targets. http:// ww.who.int/tb/post2015_strategy/en/index.html (accessed Dec 1, 2013). WHO. Report of the 13th Meeting of the Strategic and Technical Advisory Group for Tuberculosis. http://www.who.int/tb/advisory_ bodies/stag/en/index.html (accessed Dec 1, 2013). Diel R, Loddenkemper R, Zellweger J-P, et al. Old ideas to innovate TB control: preventive treatment to achieve elimination. Eur Respir J 2013; 42: 785–801. www.thelancet.com Vol 383 June 14, 2014