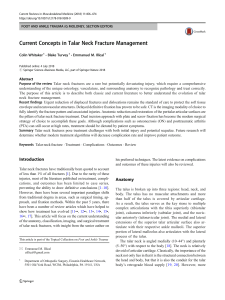
Review Article External Fixation: Principles and Applications Abstract Jesse E. Bible, MD, MHS Hassan R. Mir, MD The modularity and ease of application of modern external fixation has expanded its potential use in the management of fractures and other musculoskeletal conditions. In fracture care, it can be used for provisional and definitive fixation. Short-term provisional applications include “damage control” and periarticular fracture fixation. The risk:benefit ratio of added stability needs to be assessed with each fixator. Soft-tissue management is critical during pin insertion to lessen the risk of loosening and infection. Although provisional fixation is safe for early conversion to definitive fixation, several factors affect the timing of definitive surgery, including the initial injury, external fixator stability, infection, and the physiologic state of the patient. W From the Penn State Milton S. Hershey Medical Center, Hershey, PA (Dr. Bible) and Vanderbilt University Medical Center, Nashville, TN (Dr. Mir). Dr. Mir or an immediate family member serves as a paid consultant to Smith & Nephew, and serves as a board member, owner, officer, or committee member of the American Academy of Orthopaedic Surgeons, the Foundation for Orthopedic Trauma, and the Orthopaedic Trauma Association. Neither Dr. Bible nor any immediate family member has received anything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject of this article. J Am Acad Orthop Surg 2015;23: 683-690 http://dx.doi.org/10.5435/ JAAOS-D-14-00281 Copyright 2015 by the American Academy of Orthopaedic Surgeons. ith Hippocrates having used an external “shackle” device for maintaining a tibia fracture out to length, the concept of external fixation is more than 2,000 years old. Today, the principles and techniques of external fixation continue to be an essential component in every orthopaedic surgeon’s armamentarium. In acute fracture care, its use is separated into two categories: provisional and definitive. Provisional fixation is further subdivided into “damage control” and periarticular fracture stabilization. In both of these short-term applications, the surgeon must consider the impact of the fixator on the patient and any future needs for definitive management as well as the ability to adapt the provisional fixator into a definitive fixator if needed. Fixator Principles and Biomechanics Pins Pins, including half-pins and transfixion pins, serve a critical role in construct stability because of their direct link to the bone. Although the risk:benefit ratio of added stability needs to be assessed with each type of fixator, many of the options to increase stability involve the use of pins (Table 1). When using a fixator for definitive fixation, the ideal construct for stability consists of placing one pin as close to the fracture as possible, with another pin placed as far from the fracture as possible within the same bone. When using a fixator for provisional stabilization, potential areas for future definitive fixation should be considered and avoided, if possible, to prevent the occurrence of deep infection arising from pin tracts located within the zone of plate fixation. Pin bending strength is increased to the fourth power of the increase in the pin’s radius.1 This gain in stiffness is critical because decreased pin stiffness causes increased stress at the pin-bone interface, leading to micromotion and ultimate pin failure.2 Therefore, the largest diameter pin should be used; however, to minimize the risk of November 2015, Vol 23, No 11 Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. 683 External Fixation: Principles and Applications Table 1 Methods to Manipulate an External Fixator to Increase Stability Increase Diameter of pins Number of pins used Pin spread Number of planes pins are placed Diameter of rods Number of rods Decrease Pin-to-fracture distance Bone-to-rod distance creating a substantial stress riser that leads to a possible fracture, the pin should not exceed one-third diameter of the bone.1 Similarly, the advantage of using a smaller core diameter pin for added pullout strength must be weighed against its reduced bending strength. Of the various pin coatings and designs that have been developed, hydroxyapatite-coated pins provide a significantly improved pinbone interface and a greater extraction torque compared with uncoated pins.3-6 Tapered, or conical, pins were developed to obtain purchase on both cortices and to yield higher insertion and extraction torques as well as sound osteointegration.4 However, concern remains regarding their potential for loss of fixation; if the pins back out even minimally, their fixation significantly diminishes because of their shape. The weakest point of a pin is the thread-shank junction, which forms a large stress riser. Therefore, placing the pin’s junction at the pin-bone interface, at the site of the highest stress, should be avoided. If possible, the shank should be buried into the proximal cortex, doubling the pin’s stiffness.1 In addition, soft tissues become less irritated and inflamed 684 when only the smooth shank is exposed. Bars Sidebars, or rods, form the link between bony fragments in the fixator construct. Originally, stainless steel and aluminum alloy materials were used. The use of carbon fiber rods has since become more common, and compared with stainless steel rods, they are 15% stiffer in loading to failure.7 However, when carbon fiber rods are used in an entire fixator construct, it is only 85% as stiff as one created using stainless steel rods. This finding is attributed to the clamps being less effective (ie, limited by clamp tightening) in connecting to carbon fiber rods versus stainless steel rods. Clamps and Rings Clamps allow for multiple degrees of freedom and adaptability in their connection of pins and wires to bars and rings. Simple (ie, single) clamps connect one pin to a rod, whereas modular (ie, universal) clamps allow multiple pins to be connected to a rod. In the latter, distributing the pins symmetrically within the clamp provides the best pin fixation strength within the clamp.8 With the use of modular clamps, there is the possibility of uneven holding strength on multiple pins within the clamp, thus interfering with the rigidity of the fixation. This problem is avoided with the use of simple clamps. Ring fixators are especially useful in fractures around the joint and in those with significant bone loss. They allow for dynamic axial loading (ie, weight bearing) and joint motion during treatment. However, their application and utility require a substantial learning curve. Although best popularized by their limb-lengthening ability using multiplanar fixators, more straightforward ring constructs can be applied, such as the hybrid frame. This frame combines the advantages of ring fixators in the periarticular region and the simplicity of planar half-pins in the diaphyseal region. Construct Design Fixator configurations are subdivided according to whether they are unilateral/bilateral or uniplanar/multiplanar. Although bilateral frames (ie, placed on both sides of the bone) are stiffer, they can be cumbersome to apply and hold a higher potential for pin infection compared with unilateral frames. Similarly, uniplanar frames are less obstructive for softtissue access but are four to seven times weaker when stressed in the plane orthogonal to the pins.1 In addition to increasing the number of planes to increase construct stability, other methods can be employed (Table 1). Although anatomic safe zones may be a limiting factor, the pins and bars should be aligned with the bending axis of the bone. Likewise, when a ring fixator is used for oblique fractures, placing angled pins parallel to the fracture line to create a structural parallelogram is more effective at reducing shear than is the use of transverse pins.9,10 MRI Compatibility Surgeons should be familiar with the MRI compatibility of the external fixation systems used in their hospitals. Although most modern external fixation systems are MRI-compatible, some older systems are not. Paperwork from the device manufacturer should be readily available online to confirm compatibility and to minimize delays in the acquisition of MRIs for other injuries, such as spinal injuries. Application Technique Significant debate exists regarding techniques for pin insertion. Soft-tissue Journal of the American Academy of Orthopaedic Surgeons Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. Jesse E. Bible, MD, MHS, and Hassan R. Mir, MD management is critical and should entail choosing an anatomic site without a large soft-tissue sleeve, making an adequate skin incision, spreading tissues to bone, using cannulation during drill/pin insertion with the use of protective sleeves, and stabilizing soft tissues around the pin to prevent motion. It is thought that excessive motion of muscle and skin around bone results in local inflammation, thus leading to pintract infections.11 The most common method of reducing motion is the use of a gentle compressive dressing around the pin to create a bolster between the skin and the clamp, such as a roll of gauze wrapped around the pin. Thermal damage to bone is thought to play a potential role in pin loosening. The severity of damage is related to the maximum temperature and the amount of time that bone is exposed to increased temperatures during pin insertion.12 Irreversible changes, including osteocyte death and alkaline phosphatase inactivation, are seen at 122°F (50°C).12-14 Methods to decrease temperatures during pin insertion include predrilling, irrigation during drilling, and power insertion of the pin. A significantly longer duration of temperatures $131°F (55°C) was seen when a hand technique was used for pin insertion versus a power technique, both at 300 and 700 rpm.12 However, all techniques easily reached temperatures $194°F (90° C). Although this study was based on older pins without advance flutes that are commonly in use today, it suggests that time in contact with bone, which causes frictional heat, plays a significant role and should be limited by using a power technique. More importantly, the study revealed that predrilling before manual pin insertion lowered temperatures by more than half compared with pin insertion without predrilling.12 The dogma of predrilling has been lessened by recent pin designs that incorporate a modified drill point with flutes and cut lead for tapping. Additionally, the new modified thread pitch theoretically allows for the advancement speed of the pin to be controlled, thus avoiding stripping the near cortex when the cutting tip hits the far cortex. However, Seitz et al15 reported a 22% reduction in bone purchase of self-drilling pins compared with predrilled pins. The authors also observed a visible “wobble factor” when predrilled pins were inserted by hand. This wobble leads to conical deformation and subsequent instability of the near cortex, causing increased stress in the far cortex.11 Fixator Configurations Most external fixators placed in the United States today are for provisional stabilization. As discussed, these frames should be simple constructs and should be applied with consideration of their impact on the patient’s physiology and care, any future definitive fixation, and implant cost. Additionally, during the insertion of any external fixation device within the pediatric population, care must be taken to avoid the epiphysis and open physis. Humerus Placement of an external fixator on the humerus can be especially useful after revascularization, in patients with burns or grossly contaminated open fractures, and in obese patients when splinting is unlikely to hold the fracture in acceptable alignment. Pins (5 mm) are placed anterolaterally in the proximal humerus, taking care to avoid damage to the axillary and radial nerves, and posterolaterally (4 to 5 mm) in the distal humerus, avoiding the olecranon fossa (Figure 1). Elbow “Floating elbows” can be stabilized with posterolateral distal humerus pins (4 to 5 mm) and subcutaneous proximal ulna pins (4 mm). A hinged fixator can be used for definitive treatment of certain periarticular fractures or ligament instability. The details involved in its application and management are beyond the scope of this article but can be referenced at Chen and Julka16 and Wegmann et al.17 Forearm Given its subcutaneous placement, the ulna is best used for forearm stabilization. Pins measuring 4 mm and 3 mm are subcutaneously placed proximally and distally, respectively. Proximal radius pin placement should be avoided because of the variable location of the posterior interosseous nerve. Similarly, the superficial radial nerve is at risk during distal radius pin insertion. Distal Radius For distal radius fractures, restoration of alignment can be achieved with spanning and nonspanning external fixation of the wrist. The proximal pins (3 to 4 mm) should be placed posterior to the radial artery, with the superficial radial nerve protected. Distal pins (3 mm) are inserted into the base of the second metacarpal using a small incision to identify the terminal branches of the superficial radial nerve and to sharply elevate off the first dorsal interosseous muscle. When tightening the construct, overdistraction of the wrist joint should be avoided because this can cause difficulty with finger flexion as well as potentially play a role in the development of complex regional pain syndrome.18 Pelvis An anteriorly placed fixator can be used to close an anterior-posterior compression injury, open a lateral November 2015, Vol 23, No 11 Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. 685 External Fixation: Principles and Applications anterolateral femur and the anteromedial tibia (Figure 3, A). Proximal tibia pins should be placed at least 14 mm distal to the articular surface to avoid joint penetration. A single long bar or smaller crossing bars from each segment can be used to span the knee joint, ensuring that no radiopaque clamps overlie the joint line. The fixator should be locked into a slight amount of flexion, measuring approximately 5° to 15°. A posterior splint may be used to provide additional stability. Figure 1 Tibia The plane of insertion for fixator pins into the distal humerus. compression injury, or translate a vertical injury (Figure 2). A small incision and dissection 2 cm posterior to the anterior-superior iliac spine is carried down to bone to avoid injury to the lateral femoral cutaneous nerve. Pins are directed posteromedially between the inner and outer tables of the gluteal pillar. If needed, a second pin on each side can be placed more posterior on the crest and angled more horizontally. It may be advantageous to use a pin with a blunt tip to avoid penetration of the inner and outer tables. The placement of subcristal pins into the iliac crest in an anteroposterior fashion is a newer technique that does not require the use of fluoroscopy.19 Supra-acetabular pins have become more commonly used in the acute setting as well as in situations that require long-term anterior external fixation because they allow for more powerful control of the hemipelvis.20,21 These pins require the use of fluoroscopic imaging for safe placement. Additional anterior constructs have also been described that combine iliac wing and supraacetabular pins to provide multiplanar stability.22 686 Posterior pelvic external fixation has been described with the use of pelvic C-clamps applied to the posterior ilium above the greater sciatic notch; however, this procedure has been associated with complications related to errant pin placement if done without fluoroscopy. An alternative construct with the use of the pelvic C-clamp is to place the pins into the greater trochanters so that the C-clamp acts in the same fashion as a pelvic binder or sheet, and the pins can be placed relatively safely.23 Femur Femoral shaft fractures are stabilized using pins (5 mm) placed anterolaterally or directly lateral, both proximally and distally. The distal pins must be placed with consideration to avoid the suprapatellar pouch. Lateral pin placement does not interfere with future prone positioning during the treatment of other concurrent injuries. Knee Knee dislocations, distal femur fractures, and tibial plateau fractures are all stabilized using pins (5 mm) in the The subcutaneous anteromedial surface of the tibia is used to place pins perpendicular to either the anteromedial or posterior faces of the tibial cortex. Distal pins should be placed using blunt dissection to avoid injury to the anterior tibial vessels and the deep peroneal nerve. Periarticular Ankle The configuration most commonly used for significantly swollen ankle and pilon fractures involves a delta frame with anteromedially placed tibial shaft pins and a transcalcaneal pin (Figure 3, B). The insertion of a transfixation pin, compared with a half-pin, into the calcaneus aids in fracture reduction and stabilization. It is inserted distal and posterior to the neurovascular bundle. The safest medial calcaneus placement is posterior to the halfway point from the posteroinferior calcaneus to the inferior medial malleolus and posterior to the one-third mark from the posteroinferior calcaneus to the navicular tuberosity24 (Figure 4). Blunt dissection should be carried down to bone to avoid injury to the lateral plantar and medial calcaneal nerves. To provide for additional stability and to prevent equinus, a posterior splint may be applied. Alternatively, additional pins may be placed medially into the talar neck, Journal of the American Academy of Orthopaedic Surgeons Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. Jesse E. Bible, MD, MHS, and Hassan R. Mir, MD cuneiforms, or first metatarsal base, or laterally into the cuboid or fifth metatarsal base. For cuneiform pin placement, the pin should enter the dorsal half of the medial cuneiform to avoid the structures plantar to the midfoot arch. Figure 2 Calcaneus A medially placed spanning external fixator can facilitate restoration of anatomic height and length of the calcaneus while awaiting definitive treatment. Half-pins (5 mm) are placed medial to lateral in the distal tibia, medial cuneiform, and calcaneal tuberosity. After bar placement, a laminar spreader and/or compressordistractor device is used to strategically reestablish length as well as correct the varus and translation deformity.25 Conversion to Definitive Treatment Several factors that must be considered in the timing of conversion from external fixation to definitive treatment include (1) condition of the soft tissues, (2) the initial injury, (3) the need for further surgical débridement, (4) fasciotomy wounds, (5) the condition of external fixator pins, (6) external fixator stability, (7) bone or soft-tissue loss, (8) vascular injury, (9) infection, and (10) the physiologic state of the patient. With so many variables affecting timing, there is a paucity of data regarding the safety and optimal timing of delayed conversion. For femoral shaft fractures, early definitive stabilization is thought to reduce the risks of decubitus ulcers, pneumonia, and venous thromboembolic disease. Nowotarski et al26 retrospectively reviewed 59 femoral shaft fractures (19 open) that were initially stabilized using an external fixator and later converted to intramedullary nailing (IMN) at an average of 7 days Possible pelvic external fixation options include supra-acetabular pin (A and B), orthogonal pin construct (both iliac crest and supra-acetabular pins) (C), or subcristal pin (D). (range, 1 to 49 days). Overall, observational studies have reported similar satisfactory results of early (4 to 7 days) conversion to IMN.27,28 Blachut el al29 reported on 41 open tibia shaft fractures initially managed with external fixation and conversion to IMN with an average of 17 days (range, 6 to 52 days) for fixator placement. Two infections, two nonunions, and one delayed union were seen. Bhandari et al30 combined data from prior studies in which patients underwent provisional external fixation followed by IMN of the femur or tibia. Based on these studies, the authors found an average plausible infection rate of 3.6% and 9% for acute conversion of femur and tibia fractures, respectively. They also reported average plausible union rates of 98% and 90%, respectively. It was determined that a length of fixation of #28 days reduced the risk of infection by 83%. This study has many limitations: it combined several level IV retrospective studies, and many patients undergoing later conversion likely had other confounding medical conditions, thus increasing the infection rate. Although conversion to IMN is most frequently performed as a single procedure, a staged conversion, or “pin holiday,” before definitive fixation is sometimes warranted. The November 2015, Vol 23, No 11 Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. 687 External Fixation: Principles and Applications Figure 3 External Fixation for Definitive Management A, Anterolateral femur and anteromedial tibia half-pins can be used to span the knee in a tibial plateau fracture. Note that the tibia pins are placed distal to the position of the future incision and plate placement. B, An anteromedial tibia half-pin and a calcaneal transfixation pin can be used to create a delta frame for tibial pilon fractures. Figure 4 Besides the use of formal open reduction and internal fixation or IMN, other fixation options include limited internal fixation supplemented with external fixation and solely definitive external fixation. Early limited internal fixation with external fixation can be a successful strategy in the acute management of difficult periarticular fractures; this approach greatly aids in later definitive open reduction and internal fixation (Figure 5). This is especially true in pilon fractures with a long oblique fracture extension into the diaphysis that can involve significant reduction difficulties at the time of definitive fixation (ie, 7 to 21 days from injury).31 If external fixation is used solely for definitive management, callus formation (ie, secondary bone healing) around the fracture should be expected because of the relative stability imparted by the external fixator. However, if supplemented with internal fixation, a component of absolute stability can be added, allowing for primary bone healing. Pin-site Care and Infections Illustration demonstrating the nerves most at risk during medial calcaneal pin placement. Note the small window for safe placement in the posteroinferior portion of the calcaneus, although the medial calcaneal nerve (MCN) is still at risk of injury. LPN = lateral plantar nerve, MPLPN = most posterior lateral plantar nerve, MPN = medial plantar nerve, PTA = posterior tibial artery, PTN = posterior tibial nerve most notable circumstance is concern for pin-site infection. A common practice involves removing the fixator, débriding the pin sites, placing 688 the extremity in a splint or traction, and administering antibiotics before returning to the operating room for definitive IMN. Pin-site infections have a reported incidence ranging from zero to 66.7%.32-37 Mahan et al38 reported on 214 pins examined at time of pin removal; 74.8% had bacteria present on them, including 37.5% with virulent Staphylococcus aureus and 9.4% with Escherichia coli. The authors also found a significant correlation between loose pins and infection, supporting the belief that soft-tissue motion is an important factor leading to infection. Methods of pin-site care vary considerably. Lethaby et al39 looked at all studies since 1950 regarding pin-site care. The authors found insufficient Journal of the American Academy of Orthopaedic Surgeons Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. Jesse E. Bible, MD, MHS, and Hassan R. Mir, MD Figure 5 A pilon fracture definitively treated with limited internal fixation and external fixation in a patient with uncontrolled diabetes. Preoperative AP (A) and lateral (B) radiographs, AP (C) and lateral (D) radiographs following external fixator placement during initial hospitalization, and postoperative AP (E) and lateral (F) radiographs after definitive treatment with limited internal fixation and external fixation. evidence that any particular strategy of pin-site care minimizes infection rates. Given the high incidence of pin-site complications, any problematic pin site should raise suspicion of a pinsite infection and be dealt with accordingly. Checketts et al40 devised a classification system for pin-site infection that aids in the formulation of treatment options (Table 2). It should be stressed that if a pin is found to be loose, it should be removed and replaced depending on the effect on overall construct stability. Summary External fixation has a vital role in both provisional and definitive fracture fixation. In provisional stabilization, the surgeon must consider the impact of the fixator on the patient’s care and definitive management, as well as the ability to adapt the provisional fixator into a definitive fixator if needed. The basic principles and techniques of external fixation should be applied to maximize the fixator’s potential to promote Table 2 Pin-tract Infection Classification and Treatment40 Grade 1 2 3 4 5 6 Appearance Treatment Slight erythema, little discharge Erythema, discharge, and pain in soft tissue Grade 2 but no improvement with antibiotics Soft-tissue infection involving several pins Grade 4 and radiographic evidence of bone involvement Infection after fixator removal (clinical and radiographic) fracture healing and potential complications. minimize References Evidence-based Medicine: Levels of evidence are described in the table of contents. In this article, references 33, 35, and 39 are level I studies. References 32, 34, and 36 are level II studies. References 18, 19, 26-30, and 38 are level III studies. References 1-17, 20-24, 31, 37, and 40 are level V expert opinion. Improved pin care Topical and/or oral antibiotics Remove pin and change antibiotic regimen Remove any loose pins Remove entire fixator construct and curettage pin tract Débridement, irrigation, and systemic antibiotics References printed in bold type are those published within the past 5 years. 1. Behrens F, Johnson WD, Koch TW, Kovacevic N: Bending stiffness of unilateral and bilateral fixator frames. Clin Orthop Relat Res 1983;178:103-110. 2. Huiskes R, Chao EY, Crippen TE: Parametric analyses of pin-bone stresses in external fracture fixation devices. J Orthop Res 1985;3(3):341-349. 3. Moroni A, Vannini F, Mosca M, Giannini S: State of the art review: Techniques to avoid pin loosening and infection in external fixation. J Orthop Trauma 2002;16(3):189-195. November 2015, Vol 23, No 11 Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited. 689 External Fixation: Principles and Applications 4. Moroni A, Faldini C, Pegreffi F, Giannini S: Fixation strength of tapered versus bicylindrical hydroxyapatite-coated external fixation pins: An animal study. J Biomed Mater Res 2002;63(1):61-64. 5. Moroni A, Aspenberg P, Toksvig-Larsen S, Falzarano G, Giannini S: Enhanced fixation with hydroxyapatite coated pins. Clin Orthop Relat Res 1998;346:171-177. 6. Moroni A, Toksvig-Larsen S, Maltarello MC, Orienti L, Stea S, Giannini S: A comparison of hydroxyapatite-coated, titanium-coated, and uncoated tapered external-fixation pins: An in vivo study in sheep. J Bone Joint Surg Am 1998;80(4):547-554. 17. Wegmann K, Lappen S, Pfau DB, Neiss WF, Müller LP, Burkhart KJ: Course of the radial nerve in relation to the center of rotation of the elbow: The need for a rational safe zone for lateral pin placement. J Hand Surg Am 2014;39(6): 1136-1140. 18. Kaempffe FA, Wheeler DR, Peimer CA, Hvisdak KS, Ceravolo J, Senall J: Severe fractures of the distal radius: Effect of amount and duration of external fixator distraction on outcome. J Hand Surg Am 1993;18(1):33-41. 19. Solomon LB, Pohl AP, Sukthankar A, Chehade MJ: The subcristal pelvic external fixator: Technique, results, and rationale. J Orthop Trauma 2009;23(5):365-369. 7. Kowalski M, Schemitsch EH, Harrington RM, Chapman JR, Swiontkowski MF: Comparative biomechanical evaluation of different external fixation sidebars: Stainless-steel tubes versus carbon fiber rods. J Orthop Trauma 1996;10(7):470-475. 20. Calafi LA, Routt ML: Anterior pelvic external fixation: Is there an optimal placement for the supra-acetabular pin? Am J Orthop (Belle Mead NJ) 2013;42(12): E125-E127. 8. Aro HT, Hein TJ, Chao EY: Mechanical performance of pin clamps in external fixators. Clin Orthop Relat Res 1989;248:246-253. 21. Stahel PF, Mauffrey C, Smith WR, et al: External fixation for acute pelvic ring injuries: Decision making and technical options. J Trauma Acute Care Surg 2013; 75(5):882-887. 9. Lowenberg DW, Nork S, Abruzzo FM: Correlation of shear to compression for progressive fracture obliquity. Clin Orthop Relat Res 2008;466(12):2947-2954. 10. Metcalfe AJ, Saleh M, Yang L: Techniques for improving stability in oblique fractures treated by circular fixation with particular reference to the sagittal plane. J Bone Joint Surg Br 2005;87(6):868-872. 11. Ziran BH, Smith WR, Anglen JO, Tornetta P III: External fixation: How to make it work. J Bone Joint Surg Am 2007; 89(7):1620-1632. 12. Matthews LS, Green CA, Goldstein SA: The thermal effects of skeletal fixation-pin insertion in bone. J Bone Joint Surg Am 1984;66(7):1077-1083. 13. Bonfield W, Li CH: The temperature dependence of the deformation of bone. J Biomech 1968;1(4):323-329. 14. Eriksson A, Albrektsson T, Grane B, McQueen D: Thermal injury to bone: A vital-microscopic description of heat effects. Int J Oral Surg 1982;11(2):115-121. 15. Seitz WH Jr, Froimson AI, Brooks DB, Postak P, Polando G, Greenwald AS: External fixator pin insertion techniques: Biomechanical analysis and clinical relevance. J Hand Surg Am 1991;16(3):560-563. 16. Chen NC, Julka A: Hinged external fixation of the elbow. Hand Clin 2010;26 (3):423-433. 690 22. Archdeacon MT, Arebi S, Le TT, Wirth R, Kebel R, Thakore M: Orthogonal pin construct versus parallel uniplanar pin constructs for pelvic external fixation: A biomechanical assessment of stiffness and strength. J Orthop Trauma 2009;23(2): 100-105. 23. Archdeacon MT, Hiratzka J: The trochanteric C-clamp for provisional pelvic stability. J Orthop Trauma 2006;20(1):47-51. 24. Casey D, McConnell T, Parekh S, Tornetta P III: Percutaneous pin placement in the medial calcaneus: Is anywhere safe? J Orthop Trauma 2004;18(suppl 8)S39-S42. 25. Brennan ML: Calcaneus fractures, in Gardner MJ, Harley MB, eds: Harborview Illustrated Tips and Tricks in Fracture Surgery. Philadelphia, PA, LWW, 2010, pp 388-402. 26. Nowotarski PJ, Turen CH, Brumback RJ, Scarboro JM: Conversion of external fixation to intramedullary nailing for fractures of the shaft of the femur in multiply injured patients. J Bone Joint Surg Am 2000;82(6):781-788. 27. Lavini F, Carità E, Dall’oca C, et al: Internal femoral osteosynthesis after external fixation in multiple-trauma patients. Strategies Trauma Limb Reconstr 2007;2(1):35-38. 28. Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13(2):78-84. 29. Blachut PA, Meek RN, O’Brien PJ: External fixation and delayed intramedullary nailing of open fractures of the tibial shaft: A sequential protocol. J Bone Joint Surg Am 1990;72(5):729-735. 30. Bhandari M, Zlowodzki M, Tornetta P III, Schmidt A, Templeman DC: Intramedullary nailing following external fixation in femoral and tibial shaft fractures. J Orthop Trauma 2005;19(2): 140-144. 31. Dunbar RP, Barei DP, Kubiak EN, Nork SE, Henley MB: Early limited internal fixation of diaphyseal extensions in select pilon fractures: Upgrading AO/OTA type C fractures to AO/OTA type B. J Orthop Trauma 2008;22(6):426-429. 32. Patterson MM: Multicenter pin care study. Orthop Nurs 2005;24(5):349-360. 33. W-Dahl A, Toksvig-Larsen S, Lindstrand A: No difference between daily and weekly pin site care: A randomized study of 50 patients with external fixation. Acta Orthop Scand 2003;74(6):704-708. 34. Camilo AM, Bongiovanni JC: Evaluation of effectiveness of 10% polyvinylpyrrolidoneiodine solution against infections in wire and pin holes for Ilizarov external fixators. Sao Paulo Med J 2005;123(2):58-61. 35. Egol KA, Paksima N, Puopolo S, Klugman J, Hiebert R, Koval KJ: Treatment of external fixation pins about the wrist: A prospective, randomized trial. J Bone Joint Surg Am 2006;88(2):349-354. 36. Grant S, Kerr D, Wallis M, Pitchford D: Comparison of povidone-iodine solution and soft white paraffin ointment in the management of skeletal pin-sites: A pilot study. J Orthop Nurs 2005;9:218-225. 37. Henry C: Pin sites: Do we need to clean them? Practice Nursing 1996;7(4):12-17. 38. Mahan J, Seligson D, Henry SL, Hynes P, Dobbins J: Factors in pin tract infections. Orthopedics 1991;14(3):305-308. 39. Lethaby A, Temple J, Santy J: Pin site care for preventing infections associated with external bone fixators and pins. Cochrane Database Syst Rev 2008;4: CD004551. 40. Checketts R, MacEachem A, Otterbum M: Pin tract infection and the principles of pin site care, in DeBastiani A, Graham Apley A, Goldberg D, eds: Orthofix External Fixation in Trauma and Orthopaedics. Berlin, Springer, 2000, pp 97-103. Journal of the American Academy of Orthopaedic Surgeons Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.