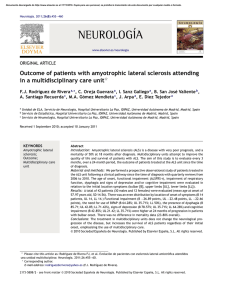
Accepted Manuscript Title: The combined use of conventional MRI and MR SpectroscopIC imaging increases the diagnostic accuracy in amyotrophic lateral sclerosis Author: Amedeo Cervo Sirio Cocozza Francesco Saccà Sara M.d.A. Giorgio Vincenzo Brescia Morra Enrico Tedeschi Angela Marsili Giovanni Vacca Vincenzo Palma Arturo Brunetti Mario Quarantelli PII: DOI: Reference: S0720-048X(14)00503-8 http://dx.doi.org/doi:10.1016/j.ejrad.2014.10.019 EURR 6923 To appear in: European Journal of Radiology Received date: Revised date: Accepted date: 27-8-2014 21-10-2014 28-10-2014 Please cite this article as: Cervo A, Cocozza S, Saccà F, Giorgio SMdA, Morra VB, Tedeschi E, Marsili A, Vacca G, Palma V, Brunetti A, Quarantelli M, The combined use of conventional MRI and MR SpectroscopIC imaging increases the diagnostic accuracy in amyotrophic lateral sclerosis, European Journal of Radiology (2014), http://dx.doi.org/10.1016/j.ejrad.2014.10.019 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. THE COMBINED USE OF CONVENTIONAL MRI AND MR SPECTROSCOPIC IMAGING INCREASES THE DIAGNOSTIC ACCURACY IN AMYOTROPHIC LATERAL SCLEROSIS ip t Amedeo Cervo1*, Sirio Cocozza1*, Francesco Saccà2, Sara M.d.A. Giorgio1, Vincenzo Brescia Morra2, Enrico Tedeschi1, Angela Marsili2, Giovanni Vacca2, Vincenzo Palma3, Arturo Brunetti1, us These authors contributed equally to this work. an * cr Mario Quarantelli4 M Highlights We assessed in ALS the diagnostic accuracy of MRI signal and MRS data used alone and in combination - We found that T2-hypointensity and NAA decrease in motor cortex are two independent phenomena - These two variables taken alone do not provide acceptable diagnostic accuracy in ALS te Ac ce p - d - The same variables , when used in combination, improve the diagnostic accuracy of MRI in ALS 1 Department of Advanced Biomedical Sciences, University “Federico II”, Naples, Italy 2 Department of Neurosciences, Reproductive Sciences and Odontostomatology, University “Federico II”, Naples, Italy 3 U.O.C. Neurofisiopatologia, PO S. Gennaro ASL Napoli 1, Naples, Italy 4 Biostructure and Bioimaging Institute, National Research Council, Naples, Italy 1 Page 1 of 39 Corresponding author: Sirio Cocozza, MD ip t Department of Advanced Biomedical Sciences University “Federico II” cr Via Pansini, 5 80131 - Naples - ITALY us E-mail: siriococozza@hotmail.it TEL +39 081 2203187 (ext -216) an FAX +39 081 2296117 Ac ce p te d M MP +39 333 6078796 2 Page 2 of 39 Abstract Purpose We aimed to assess, in amyotrophic lateral sclerosis (ALS), the diagnostic accuracy of the ip t combined use of conventional MRI signal changes (namely, hypointensity of the precentral cortex and hyperintensity of the corticospinal tracts on T2-weighted images), and N-Acetyl-Aspartate affected by limited diagnostic accuracy when used separately. us Methods cr (NAA) reduction in the motor cortex at Magnetic Resonance Spectroscopy (MRS), which are T2-hypointensity and NAA/(Choline+Creatine) ratio of the precentral gyrus and T2-hyperintensity an of the corticospinal tracts were measured in 84 ALS patients and 28 healthy controls, using a M Region-of-Interest approach. Sensitivity and specificity values were calculated using Fisher stepwise discriminant analysis, and Results d cross-validated using the leave-one-out method. te Precentral gyrus T2 signal intensity (p<10-4) and NAA peak (p<10-6) were significantly reduced in Ac ce p patients, and their values did not correlate significantly to each other both in patients and controls, while no significant differences were obtained in terms of T2-hyperintensity of the corticospinal tract. Sensitivity and specificity of the two discriminant variables, taken alone, were 71.4% and 75.0%, for NAA peak, and 63.1% and 71.4% for T2-hypointensity, respectively. When using these two variables in combination, a significant increase in sensitivity (78.6%) and specificity (82.1%) was achieved. Conclusions Precentral gyrus T2-hypointensity and NAA peak are not significantly correlated in ALS patients, suggesting that they reflect relatively independent phenomena. The combined use of these measures improves the diagnostic accuracy of MRI in ALS diagnosis. 3 Page 3 of 39 Introduction Amyotrophic lateral sclerosis (ALS) is an idiopathic neurodegenerative disorder characterized by selective degeneration of brain and spinal motor neurons controlling voluntary muscle movements . mimicking conditions, particularly when bulbar onset occurs. ip t In ALS diagnosis, brain Magnetic Resonance Imaging (MRI) is often performed to exclude other cr In the past years, several studies have shown different findings at conventional MRI in ALS patients. These include increased signal of corticospinal tracts (CST) on T2-weighted images [1-4] us (Figure 1) and reduced signal intensity of motor cortex on T2-weighted images [2, 5-7] (Figure 2). Beside conventional MRI, advanced MR techniques have been introduced to investigate ALS an patients, such as Magnetic Resonance Spectroscopy (MRS) or Diffusion Tensor Imaging (DTI). M MRS consistently showed a reduction of N-Acetyl-Aspartate (NAA) in the primary motor cortex and along the CST [8-11]. d More recently, 3D MRS acquisitions have allowed MRS measurements across the entire brain te during a single scan, showing the possibility to follow neuronal loss along the CST [12]. On the other hand DTI measures have shown not only to be able to discriminate between controls Ac ce p and ALS patients, but even among different phenotypes, showing also a correlation with disease severity [13]. Alongside with brain imaging in ALS, few studies investigated spinal cord abnormalities in ALS patients (reviewed in [14]), showing alteration in both conventional (reduced cross-sectional area and T1 hyperintensities in the antero-lateral columns) and DTI (lower mean fractional anisotropy) acquisitions in the cervical spinal cord. However, both conventional and advanced MR techniques do not provide a satisfactory level of confidence about the diagnosis of ALS, and the few studies assessing the combined use of these parameters were limited to small groups of patients [1, 15]. In the present study, we apply a multiparametric MR approach to assess the relationship between these measures and the sensitivity and specificity of their combined use in ALS diagnosis. Our 4 Page 4 of 39 approach includes the evaluation, in the precentral gyrus (PCG), of the presence of T2 hypointensity (PCG-hypo) and of the NAA/(Choline+Creatine) ratio (PCG-NAA), and, along the ip t CST, of the T2 hyperintensity (CST-hyper). Methods cr Subjects We retrospectively collected the MRI scans performed within the standard workup for ALS at our us Institution from 2006 to 2013. Only patients fulfilling the criteria for a diagnosis of probable or definite ALS according to El Escorial were included in the analysis. an Additionally, a group of 28 healthy controls (HC) of comparable age and sex, who underwent an M MRI study over the same time period and with the same acquisition protocol, was analysed. Disease duration (DD) was measured based on the first occurrence of motor symptoms clearly d related to the disease, as reported in clinical records. te The revised ALS functional rating scale (ALSFRS-R) score, a measure of disease severity [16], collected within two weeks from the MRI study, was available for all patients. Ac ce p Subjects with no history of neurological disorders or any other medical condition that could affect the central nervous system were included in the HC group. Demographic information of patients and HC data included in the study are listed in Table 1. This study was approved by the local Ethics Committee. MRI data acquisition All MRI studies were acquired with identical protocol on a 3 Tesla MRI scanner (Trio, Siemens Medical Systems, Erlangen, Germany). The sequences used for the analysis included Fast Spin-Echo T2-weighted axial images and MRS imaging, acquired with the same orientation. 5 Page 5 of 39 T2-weighted images had the following parameters: 25 axial slices, slice thickness = 4 mm, TE = 105 ms, TR = 4500 ms, echo train length= 13, acquisition matrix = 3842, FOV = 230x230 mm2. 2D multivoxel 1H-MRSI was performed using a spin-echo (point-resolved spectroscopy) sequence ip t with water suppression by means of selective excitation (TE = 270ms, FOV = 160x160 mm2, acquisition matrix = 16x16, thickness = 15mm, zero-filled to a voxel size of 5x5x15mm), acquiring cr a single axial slice, centered at the same level of the T2-weighted slice where hand “knobs” of the motor cortex was best seen. us During the MRI study the subjects were laying supine with the head fixed by straps and foam pads an to minimize head movement. M Conventional MRI analysis T2-weighted images were analysed to assess PCG hypointensity and CST hyperintensity by using a d set of pre-defined ROIs (see Figure 3 and Figure 4), placed in consensus by three trained raters (SC, PCG-hypointensity evaluation te AC, SMDAG), blinded to the clinical diagnosis. Ac ce p Pre- and post-central cortices were sampled on the T2-weighted axial slice in which the hand knob of the motor cortex was best represented. For each exam, two linear ROIs were bilaterally handdrawn on the PCG and the postcentral gyrus of the selected slice using a 2-mm brush tool of a commercial biomedical image processing software (Osirix 5.6 Pixmeo, Geneva, Switzerland; www.osirix-viewer.com) (Figure 3). These ROIs were placed within the cortical rim along the entire length of the central sulcus, avoiding CSF. As a measure of PCG hypointensity, the minimum pixel value in the corresponding ROI, normalized by the mean value of the post-central ROI, was used. The use of ROI’s minimum value, rather than the average value over the PCG ROI, has been chosen to assess the grade of PCG 6 Page 6 of 39 hypointensity, in order to avoid the confounding effect of both CSF and subcortical white matter hyperintensities (e.g. gliosis) that could affect ROI mean values. CST-hyperintensity evaluation ip t To sample CST signal intensity, three circular ROIs (6 mm of diameter each) were bilaterally placed along the course of each CST (one at the level of the cerebral peduncles, one in the posterior cr limb of the internal capsule and one in the subcortical white matter adjacent to the PCG), centered on the relative local maxima. For each ROI, corresponding mean signal intensity was normalized by us the mean value of a control ROI placed in the same slice on a structure apparently unaffected by the disease [17] (Figure 4). For the evaluation of CST hyperintensity, we could not use a similar an approach (i.e. measuring the maximum value of the ROI) to the one used for the PCG-hypo M analysis, due to the presence of CST-neighboring structures with high-intensity signal, such as te MRS analysis d cisternal CSF, dilated Virchow-Robin spaces, and gliosis. Spectroscopy data were analyzed using the software available on the scanner (Syngo MR B17, Ac ce p Siemens, Erlangen, Germany). Processing included Fourier transformation, Gaussian filtering in the time domain, and phase and baseline correction, followed by peak identification of Choline (Cho, centered at 3.22 ppm), creatine and phosphocreatine (Crea, 3.02 ppm), and NAA (2.02 ppm), and fitting of the corresponding integrals under the curve. To assess upper motor neuron (UMN) density/integrity, spectra from voxels immediately anterior to the bilateral central sulci (Figure 5) were averaged. As the ratios of NAA to Crea and/or Cho have been proposed as markers of UMN loss/dysfunction, in the present work we selected the ratio that best discriminated the two populations for comparison with other MRI measures. Statistics 7 Page 7 of 39 Student’s t-test was used to assess differences in age between HC and patients. Between-group differences in gender were tested by the Chi-squared test. As an influence of age has been previously suggested on CST-hyper, PCG-hypo and PCG-NAA in ip t normal subjects [18-20], the significance of these correlations was tested in the HC group by Spearman’s correlation coefficient. AAO) was assessed in patients by Spearman's correlation coefficient. cr Correlation between the tested MR variables and the clinical data (ALSFRS, DD and age at onset - us Sensitivity and specificity values, as well as the mean classification accuracy, were calculated to show the predictive power of the combined MRI measures during the classification process, using an Fisher stepwise discriminant analysis, and cross-validated using the leave-one-out method. During remaining cases are treated as a new dataset M the leave-one-out cross-validation, each case is extracted once and treated as test data, while the te criterion. d Fisher stepwise discriminant analysis was performed using Wilk’s Lambda as the chosen selection All statistical analyses were performed using Statistical Package for Social Science (SPSS) package Ac ce p (SPSS Inc. Released 2007, Version 16.0. Chicago, SPSS Inc.). 8 Page 8 of 39 Results ALS and HC groups were not significantly different for age and gender. The NAA/(Cho+Crea) ratio proved to be the best measure to discriminate between the two ip t populations (p<10-6 at Student’s t-test), compared to NAA/Cho (p<10-3) and NAA/Crea (p<10-4) ratios. For this reason, this measure was used for the subsequent analysis as spectroscopic marker of cr neuronal loss. No significant correlation emerged between any pair of the three tested variables neither in the HC us nor in the ALS group, suggesting their relative independence. PCG-NAA, PCG-hypo and CST-hyper measures in HC and ALS patients are reported in Table 2. M misclassification of 7/28 HC (specificity 75.0%). an PCG-NAA alone correctly classified 60/84 ALS patients (sensitivity 71.4%), with a PCG-hypo alone correctly classified 53/84 ALS patients (sensitivity 63.1%), with a d misclassification of 8/28 HC (specificity 71.4%). te CST-hyper alone correctly classified 35/84 ALS patients (sensitivity 43.8%), with a misclassification of 11/28 HC (specificity 60.7%). Ac ce p At Fisher stepwise discriminant analysis, only PCG-NAA and PCG-hypo were selected as able to discriminate between SLA and HC subjects. Leave-one-out cross validation showed that when PCG-NAA and PCG-hypo were used in combination, 66/84 subjects could be correctly classified as ALS patients, providing a substantial increase in sensitivity (78.6%), with 5/28 HC showing an abnormal value in at least one of the two measures (specificity 82.1%). Sensitivity and specificity for each measure, and the overall accuracy of the method, are reported in Table 3. Finally, when testing the relationship between MR measures and clinical variables, only PCG-hypo showed a significant correlation with ALSFRS-R (p<0.01; R=0.413). 9 Page 9 of 39 Discussion ALS diagnosis can be challenging, especially in patients without clear symptoms and signs related to the disease, or when other diseases/conditions (e.g. medullary compression due to spinal ip t pathology) are present. MRI is usually performed to exclude the possibility of other conditions known as “Motor neuron cr disease mimic” syndromes, including, but not limited to, cerebral or skull base lesions, cervical spondylotic myelopathy, foramen magnum lesions, and syringomyelia [21]. us It has been proposed that MRI could provide additional relevant information, including findings characteristic of ALS, although somewhat conflicting results have been reported. an Hyperintensity of CST in T2-weighted images has been described in several studies [1-4]. M However, this signal modification has been shown to be not sensitive for ALS, with a frequency ranging from 15% to 76% when compared to HC [22]and has been described not only in HC [4], d but also in other neurological disorders, such as X-linked Charcot-Marie Tooth neuropathies, te Krabbe disease, and adrenomyeloneuropathy [23-25]. Moreover, this finding does not correlate with the clinical impairment [3]. Ac ce p Cortical hypointensities located in the PCG in T2-weighted images have also been described in several studies in ALS [2, 6, 7, 26], showing a correlation with the severity of the disease [5, 6, 15]. This modification, taken alone, is neither sensitive nor specific for ALS [22], due to its presence both in normal aging [19] and in other neurological disorders, like Alzheimer’s disease, Parkinson’s disease and multiple infarctions [26, 27]. The cause of this T2 shortening is still unclear. Several studies have suggested a pathological iron accumulation in motor cortex microglia [6, 7], while other authors do not agree with this hypothesis [28]. MRS has been also proposed as a useful adjunct to conventional MR sequences, to detect UMN loss in ALS patients’ brains, resulting in a reduction of NAA. Several studies have detected a decreased NAA concentration in ALS, especially in PCG [8-11, 29], which appears to be correlated with the disease severity [9, 30]. 10 Page 10 of 39 In the present study MRS imaging data were analyzed. This approach was chosen, compared to single-voxel MRS, as the shape and the extension of the motor cortex makes it suitable for a technique that allows for convoluted sampling across the plane. In addition, given the bilaterality of ip t the disease, as multivoxel MRS allows to assess neuronal loss in different brain subregions simultaneously, the possibility to average left and right values allowed a substantial increase in the cr S/N ratio. Recently, MRS alterations in cervical cord have been shown in presymptomatic SOD1-positive us people, at risk for familial ALS [31], witnessing the potential of this approach to derive a biomarker for ALS diagnosis and progression. an Combination of different MR techniques is a promising way to increase confidence in ALS M diagnosis. To our knowledge, this is the first study that combines T2-weighted hypointensity of motor cortex and MRS data, with the aim of evaluating their diagnostic efficiency, both alone and d in combination, in a large group of ALS patients. te Few studies have assessed the combined use of conventional and advanced MR measures in ALS diagnosis. Sarchielli et al assessed both PCG-hypo and NAA in the motor cortex [15], although the Ac ce p specificity of PCG-hypo was not tested. Instead, Charil and colleagues reported a 100% sensitivity and specificity when combining CST hyperintensity on FLAIR images and NAA/Crea ratio, although these results were obtained in a group of only 11 patients [1]. We chose to combine PCG-hypo and PCG-NAA because, in our data sets, these two measures proved to be relatively independent and capable of discriminating the two groups. It is noteworthy that the lack of correlation between these two measures has been inconstantly reported. Previous works in smaller patient groups have either shown [15] or failed to detect [5] significant differences in NAA in the motor cortex between patients with and without cortical hypointensities in the PCG. As previous studies have linked PCG-hypo to iron accumulation mainly in the microglia [6], we speculate that this lack of correlation between PCG-hypo and PCG-NAA could be explained by the presence of a different time course of PCG-NAA decrease (an early phenomenon, reflecting UMN 11 Page 11 of 39 loss or dysfunction), compared to iron accumulation (possibly related to inflammatory phenomena secondary to microglial migration and activation), which leads to detectable PCG-hypo at a later time point. longitudinal studies with both techniques should be carried out. ip t To fully elucidate the temporal relationship between PCG-hypo and PCG-NAA over time, cr The sensitivity and specificity of PCG-hypo and PCG-NAA, which was low when the two variables were taken alone, significantly increased when they were used in combination. Therefore, in us patients undergoing an MRI study for possible ALS, beside the assessment of T2-hypointensity in the motor cortex, the use of MRS can ameliorate sensitivity, at the expenses of a limited increase in an scanning time. M In agreement with the high variability of CST-hyperintensity reported in the literature [22], we found no significant differences between ALS patients and HC; this could be explained both by the d low specificity of this finding, known to be present also in normal aging [20], and by the use of te FSE-T2-weighted images, whose sensitivity has been reported to vary from 14% to 63%[1]. To reduce the reportedly high variability of conventional MRI findings, probably due to the use of Ac ce p qualitative evaluation of absence/presence or grading of a specific sign based on subjective assessment [22], we chose a ROI-based semiquantitative approach, slightly more time-consuming, but more reproducible. The use of ROI’s minimum value for the analysis of PCG-hypo, although in general noisier than mean values, permitted to avoid the confounding effect of both CSF and subcortical white matter hyperintensities (e.g. gliosis) that could affect ROI mean values. A possible future expansion of the current approach may be the use of a measure of the skewness of the distribution of the values of the voxels in the ROI, which may provide a less noisy measure of the PCG hypointensity. Previous studies showed a correlation between the severity of the disease and PCG-NAA [9, 30]. Conversely, we did not find a significant relationship between clinical data and this variable, possibly due to methodological differences, such as the correction of our values for age (as it 12 Page 12 of 39 correlates both with clinical data and MRI findings), or the use of ALSFRS, which has been reported to be unrelated to MRS data [15, 32]. Finally, some limitations should be considered in the present report. First, the retrospective nature ip t of this study prevented the use of axial FLAIR images, which were not included in the standard workup for ALS patients at our institution. FLAIR images may be more sensitive in showing CST cr hyperintensity in ALS [3], although it is noteworthy that direct comparison of FSE-T2-weighted and FLAIR images has shown this to be at least partly compensated by a lower specificity of us FLAIR sequence [5]. Secondly, other advanced techniques proposed as promising instruments for ALS diagnosis have an not been included here. M In particular, DTI analysis has demonstrated microstructural alterations not only along the CST, specifically at the level of the posterior limb of the internal capsule, but also in other WM regions d [33, 34], including the cervical spinal cord, with significant correlation with the clinical scores [13, te 35]. Moreover, using magnetization transfer imaging, further microstructural modifications have been described both in the precentral gyrus and in extramotor areas [36]. However, as also these Ac ce p techniques appear to lack an acceptable diagnostic accuracy when taken alone [37], it remains to be tested whether they are relatively independent from the more diffuse MRI measures used in the present work, and to evaluate whether their inclusion in the proposed diagnostic setup could further increase MRI accuracy in ALS diagnosis. 13 Page 13 of 39 Conclusions In conclusion, our findings suggest that T2-hypointensity and NAA decrease in the motor cortex, assessed by a semiquantitative analysis, reflect two independent phenomena in ALS. These two Ac ce p te d M an us cr be combined to improve the diagnostic accuracy of MRI in ALS. ip t variables, which taken alone do not provide acceptable diagnostic accuracy in ALS diagnosis, can 14 Page 14 of 39 Conflict of Interest All authors do not have any financial and personal relationships with other people or organizations Ac ce p te d M an us cr ip t that could inappropriately influence (bias) our work. 15 Page 15 of 39 Role of the Funding Source The Funding Source had no involvement in study design, interpretation of data and in the writing of Ac ce p te d M an us cr ip t the article. 16 Page 16 of 39 REFERENCES [1] Charil A, Corbo M, Filippi M, et al. Structural and metabolic changes in the brain of patients with upper motor neuron disorders: a multiparametric MRI study. Amyotroph Lateral Scler 2009;10(5-6):269-79. ip t [2] Cheung G, Gawel MJ, Cooper PW, Farb RI, Ang LC, Gawal MJ. Amyotrophic lateral sclerosis: correlation of clinical and MR imaging findings. Radiology 1995;194(1):263-70. cr [3] Hecht MJ, Fellner F, Fellner C, Hilz MJ, Heuss D, Neundorfer B. MRI-FLAIR images of the head show corticospinal tract alterations in ALS patients more frequently than T2-, T1- and proton-density-weighted images. J Neurol Sci 2001;186(1-2):37-44. us [4] Mirowitz S, Sartor K, Gado M, Torack R. Focal signal-intensity variations in the posterior internal capsule: normal MR findings and distinction from pathologic findings. Radiology 1989;172(2):535-9. [5] Bowen BC, Pattany PM, Bradley WG, et al. MR imaging and localized proton spectroscopy of the precentral gyrus in amyotrophic lateral sclerosis. AJNR Am J Neuroradiol 2000;21(4):647-58. an [6] Kwan JY, Jeong SY, Van Gelderen P, et al. Iron accumulation in deep cortical layers accounts for MRI signal abnormalities in ALS: correlating 7 tesla MRI and pathology. PLoS One 2012;7(4):e35241. M [7] Oba H, Araki T, Ohtomo K, et al. Amyotrophic lateral sclerosis: T2 shortening in motor cortex at MR imaging. Radiology 1993;189(3):843-6. d [8] Gredal O, Rosenbaum S, Topp S, Karlsborg M, Strange P, Werdelin L. Quantification of brain metabolites in amyotrophic lateral sclerosis by localized proton magnetic resonance spectroscopy. Neurology 1997;48(4):878-81. te [9] Mitsumoto H, Ulug AM, Pullman SL, et al. Quantitative objective markers for upper and lower motor neuron dysfunction in ALS. Neurology 2007;68(17):1402-10. Ac ce p [10] Pioro EP, Antel JP, Cashman NR, Arnold DL. Detection of cortical neuron loss in motor neuron disease by proton magnetic resonance spectroscopic imaging in vivo. Neurology 1994;44(10):1933-8. [11] Kalra S, Hanstock CC, Martin WR, Allen PS, Johnston WS. Detection of cerebral degeneration in amyotrophic lateral sclerosis using high-field magnetic resonance spectroscopy. Arch Neurol 2006;63(8):1144-8. [12] Stagg CJ, Knight S, Talbot K, Jenkinson M, Maudsley AA, Turner MR. Whole-brain magnetic resonance spectroscopic imaging measures are related to disability in ALS. Neurology 2013;80(7):610-5. [13] Turner MR, Kiernan MC, Leigh PN, Talbot K. Biomarkers in amyotrophic lateral sclerosis. Lancet Neurol 2009;8(1):94-109. [14] Bede P, Hardiman O. Lessons of ALS imaging: Pitfalls and future directions - A critical review. Neuroimage Clin 2014;4:436-43. [15] Sarchielli P, Pelliccioli GP, Tarducci R, et al. Magnetic resonance imaging and 1H-magnetic resonance spectroscopy in amyotrophic lateral sclerosis. Neuroradiology 2001;43(3):189-97. [16] The Amyotrophic Lateral Sclerosis Functional Rating Scale. Assessment of activities of daily living in patients with amyotrophic lateral sclerosis. The ALS CNTF treatment study (ACTS) phase I-II Study Group. Arch Neurol 1996;53(2):141-7. [17] Filippini N, Douaud G, Mackay CE, Knight S, Talbot K, Turner MR. Corpus callosum involvement is a consistent feature of amyotrophic lateral sclerosis. Neurology 2010;75(18):1645-52. 17 Page 17 of 39 [18] Charles HC, Lazeyras F, Krishnan KR, et al. Proton spectroscopy of human brain: effects of age and sex. Prog Neuropsychopharmacol Biol Psychiatry 1994;18(6):995-1004. [19] Imon Y, Yamaguchi S, Katayama S, et al. A decrease in cerebral cortex intensity on T2-weighted with ageing images of normal subjects. Neuroradiology 1998;40(2):76-80. ip t [20] Ngai S, Tang YM, Du L, Stuckey S. Hyperintensity of the precentral gyral subcortical white matter and hypointensity of the precentral gyrus on fluid-attenuated inversion recovery: variation with age and implications for the diagnosis of amyotrophic lateral sclerosis. AJNR Am J Neuroradiol 2007;28(2):250-4. cr [21] Kato S, Shaw P, Wood-Allum C, Leigh P, Shaw C. Amyotrophic lateral sclerosis. In: Dickson W, editor. Neurodegeneration: The molecular pathology of dementia and movement disorders. Basel, Switzerland: ISN Neuropath Press, 2003: 350 - 71 us [22] Agosta F, Chio A, Cosottini M, et al. The present and the future of neuroimaging in amyotrophic lateral sclerosis. AJNR Am J Neuroradiol 2010;31(10):1769-77. [23] Kassubek J, Bretschneider V, Sperfeld AD. Corticospinal tract MRI hyperintensity in X-linked Charcot-MarieTooth Disease. J Clin Neurosci 2005;12(5):588-9. an [24] Satoh JI, Tokumoto H, Kurohara K, et al. Adult-onset Krabbe disease with homozygous T1853C mutation in the galactocerebrosidase gene. Unusual MRI findings of corticospinal tract demyelination. Neurology 1997;49(5):1392-9. M [25] Teriitehau C, Adamsbaum C, Merzoug V, Kalifa G, Tourbah A, Aubourg P. [Subtle brain abnormalities in adrenomyeloneuropathy]. J Radiol 2007;88(7-8 Pt 1):957-61. d [26] Waragai M. MRI and clinical features in amyotrophic lateral sclerosis. Neuroradiology 1997;39(12):847-51. te [27] Imon Y, Yamaguchi S, Yamamura Y, et al. Low intensity areas observed on T2-weighted magnetic resonance imaging of the cerebral cortex in various neurological diseases. J Neurol Sci 1995;134 Suppl:27-32. Ac ce p [28] Hecht MJ, Fellner C, Schmid A, Neundorfer B, Fellner FA. Cortical T2 signal shortening in amyotrophic lateral sclerosis is not due to iron deposits. Neuroradiology 2005;47(11):805-8. [29] Rule RR, Suhy J, Schuff N, Gelinas DF, Miller RG, Weiner MW. Reduced NAA in motor and non-motor brain regions in amyotrophic lateral sclerosis: a cross-sectional and longitudinal study. Amyotroph Lateral Scler Other Motor Neuron Disord 2004;5(3):141-9. [30] Ellis CM, Simmons A, Andrews C, Dawson JM, Williams SC, Leigh PN. A proton magnetic resonance spectroscopic study in ALS: correlation with clinical findings. Neurology 1998;51(4):1104-9. [31] Carew JD, Nair G, Andersen PM, et al. Presymptomatic spinal cord neurometabolic findings in SOD1-positive people at risk for familial ALS. Neurology 2011;77(14):1370-5. [32] Han J, Ma L. Study of the features of proton MR spectroscopy ((1)H-MRS) on amyotrophic lateral sclerosis. J Magn Reson Imaging 2010;31(2):305-8. [33] Senda J, Ito M, Watanabe H, et al. Correlation between pyramidal tract degeneration and widespread white matter involvement in amyotrophic lateral sclerosis: a study with tractography and diffusion-tensor imaging. Amyotroph Lateral Scler 2009;10(5-6):288-94. [34] Cirillo M, Esposito F, Tedeschi G, et al. Widespread microstructural white matter involvement in amyotrophic lateral sclerosis: a whole-brain DTI study. AJNR Am J Neuroradiol 2012;33(6):1102-8. [35] Nair G, Carew JD, Usher S, Lu D, Hu XP, Benatar M. Diffusion tensor imaging reveals regional differences in the cervical spinal cord in amyotrophic lateral sclerosis. Neuroimage 2010;53(2):576-83. 18 Page 18 of 39 [36] Cosottini M, Pesaresi I, Piazza S, et al. Magnetization transfer imaging demonstrates a distributed pattern of microstructural changes of the cerebral cortex in amyotrophic lateral sclerosis. AJNR Am J Neuroradiol 2011;32(4):704-8. Ac ce p te d M an us cr ip t [37] Foerster BR, Dwamena BA, Petrou M, Carlos RC, Callaghan BC, Pomper MG. Diagnostic accuracy using diffusion tensor imaging in the diagnosis of ALS: a meta-analysis. Acad Radiol 2012;19(9):1075-86. 19 Page 19 of 39 Figure legends ip t Figure 1. Corticospinal tract hyperintensities in ALS. Signal alterations along the corticospinal tracts in T2-weighted axial TSE images, in the ALS cr patient with the highest CST-Hyper value (bottom, 58yo male, 3 month disease duration), compared to a 55yo male HC (top). us Sections through cerebral peduncles (left) and internal capsule (right) are shown. an Hyperintensity of the corticospinal tract can be clearly appreciated at both levels in the patient. At Ac ce p te d M the same levels, only a mild hyperintensity can be also seen in the HC images. 20 Page 20 of 39 Figure 2. Precentral gyrus hypointensity in ALS. Hypointensities along the precentral cortex in T2-weighted axial TSE images, in two ALS patients, compared with an age/ and sex/ matched HC. ip t A significant hypointensity of the motor cortex can be clearly appreciated in the patient more severely impaired (on the right, 67yo female with 17 month disease duration, ALSFRS-R 19), cr compared to both the HC (on the left, 68yo female) and an early stage patient with shorter disease duration (in the middle, 68yo female with 3 month disease duration, ALSFRS-R 36). Ac ce p te d M an us Sections at the level of the hand knobs of the motor cortex are shown. 21 Page 21 of 39 Figure 3. Pre- and post-central gyrus ROIs for conventional MRI analysis. T2-weighted axial image at the level of the hand knob of the motor cortex with (A) and without (B) the two superimposed hand-drawn ROIs used for the assessment of PCG-hypo (red) and of the ip t mean post-central gyrus signal intensity (green). ROIs were drawn using a 2mm-brush tool along the entire length of the central sulcus, avoiding CSF. Relative T2-hypointensity of the PCG can be Ac ce p te d M an us cr appreciated. 22 Page 22 of 39 Figure 4. Corticospinal tract ROI positioning. Selected T2-weighted images at the level of the cerebral peduncles (A), posterior limb of the internal capsule (B) and the hand knob of the motor cortex (C), with superimposed ROIs placed on ip t the CST (in red), and the corresponding ROIs used for data normalization (in green), placed within the midbrain tegmentum (A), in the splenium of the corpus callosum (B) and in the postcentral Ac ce p te d M an us cr gyrus (C). 23 Page 23 of 39 Figure 5. Precentral gyri spectrum with corresponding MRS slab. Representative spectrum from the precentral regions at the level of the hand knobs in both a 50yo female HC (top) and a 48yo female ALS patient (bottom). ip t On the right, for each subject, the multivoxel MRS sampling grid is shown superimposed on the T2-weighted axial image corresponding to the center of the MRS slab, along with coronal and cr sagittal localizers for reference. Ac ce p te d M an us A clear reduction in the NAA/(Cho+Crea) ratio can be appreciated in the patient. 24 Page 24 of 39 Table 1. Subjects demographics and clinical variables. HC: healthy controls; ALS: amyotrophic lateral sclerosis; SD: standard deviation; ALSFRS-R: ip t amyotrophic lateral sclerosis functional rating scale revised; n/a: not applicable; DD: disease Ac ce p te d M an us cr duration; AAO: age at onset. Ages and DD are in years. 25 Page 25 of 39 Table 2. PCG-Hypo, PCG-Hyper and PCG-NAA values. PCG-NAA: NAA/Cho+Crea ratio in the precentral gyrus; PCG-hypo: signal intensity of the ip t precentral gyrus; PCG-hyper MC: signal intensity of the white matter at the level of the motor cortex; PCG-hyper IC: signal intensity of the white matter at the level of the posterior limb of the cr internal capsule; PCG-hyper CP: signal intensity of the white matter at the level of the cerebral peduncles. us For each measure, mean±standard deviation is reported, along with the significance of the difference between HC and ALS patients at Mann/Whitney test. Ac ce p te d M an n.s.: not significant 26 Page 26 of 39 ip t cr us Table 3. Diagnostic accuracies of PCG-NAA, PCG-hypo and their combined use in ALS patients. PCG-NAA: NAA/Cho+Crea ratio in the precentral gyrus; PCG-hypo: signal intensity of the precentral gyrus; CST-hyper: signal intensity along the Ac ce pt ed M an corticospinal tract. 27 Page 27 of 39 ip t cr Acknowledgements us This study was partly supported by the Italian Ministry of Education, University, and Research (MIUR) with a grant (PRIN 2010-2011 - Ac ce pt ed M an 2010XE5L2R_001) to E.T. 28 Page 28 of 39 Ac ce pt ed M an us cr i Table_1 Page 29 of 39 Ac ce pt ed M an us cr i Table_2 Page 30 of 39 Ac ce pt ed M an us cr i Table_3 Page 31 of 39 Ac ce pt ed M an us cr i Figure_1 Page 32 of 39 Ac ce pt ed M an us cr i Figure_2 Page 33 of 39 Ac ce pt ed M an us cr i Figure_3 Page 34 of 39 Ac ce pt ed M an us cr i Figure_4 Page 35 of 39 Ac ce p te d M an us cr ip t Figure_5 Page 36 of 39 Table 1. ALS Age (mean±SD) 57.5±13.9 (range 29-80) 61.1±11.2 (range 28-81) Sex (M/F) 12/16 ALSFRS-R (median) n/a DD (mean±SD) n/a AAO (mean±SD) n/a ip t HC 52/32 cr 38 (range 19-47) us 1.5±1.4 Ac ce p te d M an 59.6±11.3 (range 27-80) 1 Page 37 of 39 Table 2. PCG-NAA 1.35±0.13 1.19±0.14 PCG-hypo 0.65±0.7 0.56±0.10 PCG-hyper MC 0.99±0.6 1.02±0.15 PCG-hyper IC 1.25±0.15 1.26±0.14 PCG-hyper CP 0.85±0.09 0.81±0.09 p<10-6 ip t ALS p<10-4 n.s cr HC n.s n.s Ac ce p te d M an us Variable 2 Page 38 of 39 ip t cr Sensitivity Specificity Overall accuracy PCG-NAA 60/84 (71.4%) 21/28 (75.0%) 81/112 (72.3%) PCG-hypo 53/84 (63.1%) 20/28 (71.4%) 73/112 (65.1%) CST-hyper 35/84 (43.8%) 17/28 (60.7%) 52/112 (46.4%) Combined 66/84 (78.6%) 23/28 (82.1%) 89/112 (79.4%) Ac ce pt ed M an Variable us Table 3. 3 Page 39 of 39