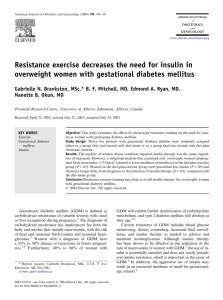
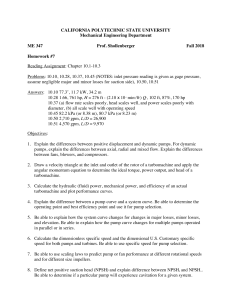
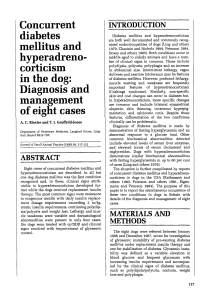
DIABETES TECHNOLOGY & THERAPEUTICS Volume 10, Number 6, 2008 © Mary Ann Liebert, Inc. DOI: 10.1089/dia.2007.0284 Review Bolus Calculator: A Review of Four “Smart” Insulin Pumps Howard Zisser, M.D.,1,2 Lauren Robinson, B.S.,1 Wendy Bevier, Ph.D.,1 Eyal Dassau, Ph.D.,1,2,3 Christian Ellingsen, B.S.,1,2 Francis J. Doyle III, Ph.D.,1,2,3 and Lois Jovanovic, M.D.1,2,3 Abstract The use of continuous subcutaneous insulin infusion (CSII) pumps has been gaining popularity since 1979, when the first research report on insulin pumps was published. Insulin pumps—small medical devices that are programmed to infuse insulin through a catheter placed under the skin—are a replacement for multiple daily injections of insulin. They are currently being used by 375,000 people with type 1 diabetes, many of whom prefer CSII to multiple daily injections because of the increased flexibility of diet and exercise, increased convenience and precision when dosing, and better predictability of blood glucose levels that insulin pumps can provide when used correctly. Recent pump manufacturers have engineered a new feature called a bolus calculator, which calculates bolus insulin doses based on input from the pump wearer, which functions to help patients obtain optimum control over blood glucose levels. The bolus calculator takes into account the patient’s current blood glucose, target blood glucose, amount of carbohydrate consumed, and other factors such as insulin sensitivity and insulin-to-carbohydrate ratio as well as duration of insulin action (“insulin on board”). Each pump company calculates insulin doses in a slightly different way. This article will review differences in bolus calculator recommendations between four insulin pumps, as well as errors that may occur when using bolus calculators. It will also include an in silico simulation of a meal followed by a snack using multiple insulin decay curves. I NSULIN PUMPS have become “smarter” in the past few years. Recent models can now calculate bolus insulin doses after receiving information from the user, which simplifies complicated calculations for the patient. Until the first “smart” insulin pump, the Deltec Cozmo® (Smiths Medical MD, Inc., St. Paul, MN), was made available in December 2002, pump users estimated insulin doses by counting carbohydrates and using insulin-to-carbohydrate ratios (number of grams of carbohydrate that would be covered by 1 unit of insulin) along with correction factors (a ratio used to calculate how much 1 unit of insulin will lower an elevated blood glucose value). Bolus calculators are now available in almost all pumps and are designed to make insulin-dosing calculations easier and more accurate and predictable for pump users. All bolus calculators take into account the amount of “insulin on board” (IOB) or the amount of insulin remaining in the body from previous insulin boluses. Bolus calculators can be programmed to predict or calculate an amount of insulin needed by taking into account the patient’s current blood glucose level, target blood glucose level, amount of carbohydrate to be consumed, insulin-tocarbohydrate ratio, and an approximation of the insulin action curve. Each pump company has a slightly different algorithm for calculating insulin doses. Gross et al.1 found that bolus calculators reduce the number of correction boluses required to correct postprandial hyperglycemia, as well as decrease the amount of carbohydrate required to treat hypoglycemia compared to standard bolus techniques, in terms of postprandial control. Although bolus calculators may simplify the math required of pump users, it is still important for patients to be well educated on the functionality of their calculator in order to avoid hyper- or hypoglycemia. Recommended calculations often need adjustment. Education is key for optimal control and preventing dependence on the calculator. This article reviews the differences in bolus calculators between four insulin pumps: MiniMed Paradigm® 515/715 (Medtronic MiniMed, Northridge, CA), Animas® IR 1250 (Animas Corp., West Chester, PA), Deltec Cozmo, and Insulet Omnipod® (Insulet Corp., Bedford, MA). 1Sansum Diabetes Research Institute, Santa Barbara, California. of Chemical Engineering, University of California at Santa Barbara. 3Biomolecular Science & Engineering Program, University of California at Santa Barbara. 2Department 441 442 ZISSER ET AL. All pump companies take into account the amount of IOB, or active insulin, when recommending insulin dosages in order to keep blood glucose levels within target range. IOB is calculated differently between the four pump companies, but all of them are based on insulin action plots, which predict the percentage of insulin remaining as a function of time. Animas and MiniMed use curvilinear “active insulin curves” (Fig. 1), whereas Deltec and Insulet use linear plots to predict the insulin on board (Fig. 2). Curvilinear plots are better approximations of the pharmacokinetic actions of insulin; linear plots make the concept of IOB easier for patients to understand. Several factors are considered when duration of insulin action is calculated, and these are shown in Table 1. Pump users can adjust the calculation for duration of insulin action within certain limits and increments. MiniMed and Deltec pumps have insulin durations ranging from 2 to 8 h, Animas has insulin durations of 1.5–6.5 h, and Insulet has insulin durations ranging from 2 to 6 h. Each pump comes with a default duration of insulin action if the pump user chooses not to adjust the calculation. One potential problem with setting a fixed duration of insulin action is that the absorption of insulin analogs (the rapid-acting insulin used in external insulin pumps) can vary 10–30% within an individual and 20–50% between individuals.2 When an insulin action duration of 4 h is considered, a 10% variability translates to 4 h 24 min. Thirty percent variability translates to 4 h 72 min. Doctors and patients must have a best guess on the appropriate insulin duration. Setting the duration of insulin action time less than the actual time increases the patient’s risk of hypoglycemia since the pump will indicate there is less IOB than what is actually there. The patient may assume that he or she no longer has active IOB and ends up “stacking” insulin, potentially leading to hypoglycemia. On the other hand, setting the duration longer than actual increases the risk of hyperglycemia since the pump will say there is more IOB than there actually is. The patient will be told to take a smaller bolus than is necessary to bring his or her blood glucose back into target range. For these reasons, and for best possible results, FIG. 1. Duration of insulin action: curvilinear. FIG. 2. Duration of insulin action: linear. patients should test insulin action duration by administering a correction bolus when blood glucose is above 250 mg/dL, then checking glucose levels every hour (or half hour) for the next 6 h.3 It is also important that the patient wait 5 h since the last insulin bolus to eliminate the possibility that other insulin doses are exerting an effect on blood glucose levels. The time it takes for the blood glucose level to return to target level and remain steady is the correct duration of insulin action. This is similar to conducting a correction factor test and should be used for best results. Setting insulin action durations is one way of regulating how aggressive or conservative one’s pump therapy will be. Another factor that makes a pump more or less aggressive is how it calculates a suggested insulin dose. Current pumps manufactured by MiniMed, Animas, Deltec, and Insulet all contain “smart” features that include suggested bolus recommendations/suggestions. Although they are quite similar, each deals with the problem in a unique fashion. Deltec is the only pump that subtracts IOB from meal boluses from subsequent meal boluses of meals eaten within the defined duration of insulin action. When a correction bolus is calculated, all pumps subtract IOB from the amount of insulin needed to bring blood glucose levels back to target if the IOB resulted from a previous correction bolus. Insulet does not currently track insulin from meal boluses, so any correction bolus will not take into account meal bolus insulin. The manufacturers will continue to refine these algorithms as time goes by. When it comes to calculating meal boluses, different rules come into play. If a blood glucose level within target range is entered into the calculator, MiniMed, Animas, and Insulet recommend the full meal dosage of insulin. Deltec, on the other hand, subtracts all of the IOB from the meal bolus and suggests the difference between the two to cover the meal. All four pumps will recommend the full meal insulin dose if no blood glucose reading is entered. The amount of IOB when using extended boluses also varies across pumps. An extended bolus is a bolus given over a prolonged period of time, anywhere from 15 min to 8 h, and are used for a high fat or protein-rich meal, for a very slowly eaten meal, or for patients with gastroparesis. Insulet does not consider extended boluses when calculating new BOLUS CALCULATOR REVIEW TABLE 1. 443 FACTORS USED FOR CALCULATING DURATION OF INSULIN ACTION Insulin pump manufacturer Pump model Range of insulin action Default insulin action Shape of insulin action plot Increment adjustment MiniMed Deltec Animas Insulet Paradigm 515/715 2–8 h 6h Curvilinear Cozmo 2–8 h 6h Linear; simply to make graph more convenient to understand 15 min IR 1250 1.5–6.5 h 4h Curvilinear Omnipod 2–6 h 3h Linear 30 min 30 min 1h insulin dosages since it is assumed that extended boluses are used only for covering meals. MiniMed, Animas, and Deltec track insulin once it has been delivered in small increments; thus the pump user knows how much insulin is active whether it properly covers the meal or not. An example of an in silico simulation demonstrating how decisions related to how smart pumps are set up is presented here. The idea of dosing insulin based on the use of IOB curves is demonstrated by a simulation model based on a modification of the oral glucose meal simulation model of Dalla Man et al.4 The simulated subject’s body weight is 51.8 kg. The insulin-to-carbohydrate ratio for meals is 1 unit of insulin for every 24 g of carbohydrate, and the correction factor is 1 unit of insulin for 80 mg/dL. A steady-state value of 120 mg/dL is defined as the target glucose and the initial condition for the simulation. One hour into the simulation a 60-g carbohydrate meal is consumed with an optimal bolus of 2.6 U to cover the meal. Three hours post-meal the subject consumes a 20-g carbohydrate snack when the glucose measurement is 212 mg/dL. To cover the snack and to correct to the target value the patient will need a total of 1.97 U of insulin (0.82 U for the snack and 1.15 U as a correction to the current glucose level). Figure 3 shows the result of the simulation when different IOB curves are selected. If the subject is using a 2-h curve, FIG. 3. Results of an in silico simulation using multiple IOB decay curves for a 20-g carbohydrate snack, 3 h after a 60-g carbohydrate meal. the bolus calculator will suggest that the subject take the full amount for the snack and for the correction for hyperglycemia, since it thinks that there is no residual IOB, resulting in a glucose level below target. If the subject is using an 8-h curve, the bolus calculator will suggest that the subject take only 0.25 U (total calculated insulin [1.97 U] minus IOB [1.72 U]), resulting in hyperglycemia. A wise selection of the appropriate curve is needed by the patient in order to prevent over- and undercorrection for meals and high blood glucose. Note that the simulated results are only for one in silico subject using these parameters and this model. Results will vary depending on insulin sensitivity. Also, these results are only representative of bolus calculators that carry mealrelated insulin forward. Other possible errors associated with bolus calculators arise because the calculators do not take into account bolus size, exercise, or heat; these variables can influence the amount of insulin on board. Larger boluses remain in one’s system longer than small boluses, and will lower blood glucose levels for extended periods of time.2 Exercise and heat decrease the time it takes to absorb insulin. An ambient temperature of 30°C causes insulin to be absorbed three to five times faster than at a temperature of 10°C, indicating that temperature can significantly influence blood glucose levels. Exercise increases insulin absorption and decreases its duration of action. In cool weather, exercise can increase absorption by 22%; this is increased to 28% in warm weather.5 These factors are not considered when calculating IOB. Thus, the boluses recommended could be higher or lower than what is needed. It is therefore important for pump users to be well-educated and take extra precaution when using their bolus calculators under these conditions. Transcription errors can occur when the pump user enters his or her own blood glucose value into the pump, rather than using automatic meter–pump communication. The MiniMed Paradigm 515/715 is supplied with a meter that communicates with the pump via radio waves. The Deltec Cozmo can have a small meter attached to the pump. The Animas IR 1250 does not have a meter–pump communication system, but the user is able to dial his or her blood glucose level into the pump. The Insulet Omnipod comes with a Personal Diabetes Manager containing a Freestyle® meter (Abbott Diabetes Care, Alameda, CA), which calculates insulin dosages and sends information to the pump. When the automatic meter–pump communication system is used, less potential error will arise than when glucose values are manually entered. 444 Lastly, it is important to note that pump users should not become entirely dependent on their bolus calculators. Sometimes patients forget how to calculate manual boluses if they are not able to use the calculator. Thus, basal rates, insulinto-carbohydrate ratios, and correction factors should be memorized and written down so that patients do not become dependent on the bolus calculator. Since bolus calculators are still subject to error and the suggested boluses calculated are not always appropriate, patients must be educated on the functionality of their pump so they know when and if they should adjust the bolus calculator recommendations. Author Disclosure Statement Drs. Zisser, Bevier, Dassau, Doyle, and Jovanovic receive support from Insulet Corp., Medtronic Diabetes, Smiths Medical, and Animas Corp. Dr. Jovanovic sits on the advisory boards at Insulet and Medtronic. References 1. Gross T, Kayne D, King A, Rother C, Juth S: A bolus calculator is an effective means of controlling postprandial ZISSER ET AL. 2. 3. 4. 5. glycemia in patients on insulin pump therapy. Diabetes Technol Ther 2003;5:365–369. Heinemann L, Weyer C, Rauhaus M, Heinrichs S, Heise T: Variability of the metabolic effect of soluble insulin and the rapid-acting insulin analog insulin aspart. Diabetes Care 1998;11:1910–1914. Walsh J, Roberts R: Pumping Insulin—Everything You Need for Success on a Smart Insulin Pump, 4th ed. San Diego, CA: Torrey Pines Press, 2006. Dalla Man C, Rizza RA, Cobelli C: Meal simulation model of the glucose-insulin system. IEEE Trans Biomed Eng 2007;54: 1740–1749. Ronnemaa T, Koivisto VA: Combined effect of exercise and ambient temperature on insulin absorption and postprandial glycemia in type I patients. Diabetes Care 1988;11:769–773. Address reprint requests to: Howard Zisser, M.D. Director of Clinical Research Sansum Diabetes Research Institute 2219 Bath Street Santa Barbara, CA 93105 E-mail: hzisser@sansum.org