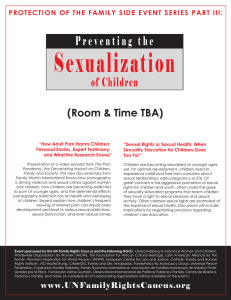
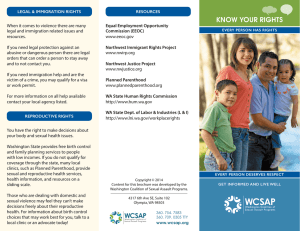
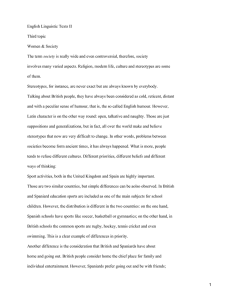
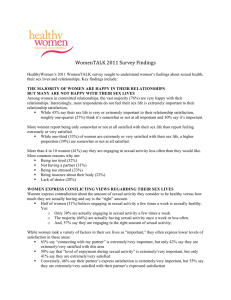
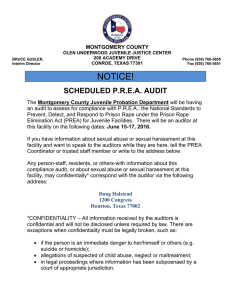
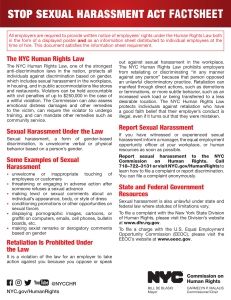
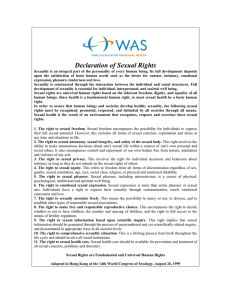
CHAPTER 20 Sexual Dysfunction in Men and Women SHALENDER BHASIN • ROSEMARY BASSON Human Sexual Response Cycle, 787 Physiologic Mechanisms of Human Sexual Response, 788 The Role of Testosterone in Regulating Sexual Function in Men, 794 Physiology of Physical Sexual Arousal in Women: Genital Congestion, 795 Physiology of Orgasm, 796 The Revised Definitions of Sexual Dysfunction in Men, 797 Current Definitions of Sexual Disorders in Women, 799 Sexual Dysfunction in the Context of Endocrine Disease, 800 Assessment of Sexual Dysfunction, 804 Management of Sexual Dysfunction in Men, 807 Management of Sexual Dysfunction in Women, 816 KEY POINTS • In contrast to the earlier sexual response model, depicting a linear progression of discrete phases, current research conceptualizes sexual response as a motivation/ incentive-based cycle comprising phases of physiologic response. These phases of the cycle overlap and their order is variable. • In middle-aged and older men, sexual dysfunction is often related to comorbid conditions, such as diabetes, coronary artery disease, or a hormonal problem. • Penile erection results from biochemical and hemodynamic events that are associated with activation of central nervous system sites, cavernosal smooth muscle relaxation, increased blood flow into cavernosal sinuses, and venous occlusion. • Corporal smooth muscle tone is regulated by transmembrane and intracellular calcium flux, which in turn is regulated by potassium channels, connexin43-derived gap junctions, and cholinergic, adrenergic, and noradrenergic noncholinergic mediators, including nitric oxide. • Testosterone regulates sexual thoughts and desire, sexual arousal, attentiveness to erotic stimuli, and sleep-entrained erections. Testosterone deficiency is a treatable cause of hypoactive sexual desire in men. • Selective phosphodiesterase 5 inhibitors are safe and effective and have emerged as first-line therapy for men with erectile disorder (ED). • Sexual response is understood to be incentive based: multiple reasons for sex motivate receptivity to sexual stimuli that can be appraised as sexually arousing. • Physical and subjective arousal may diverge. Women complaining of low sexual arousal usually physically respond to sexual stimuli in a laboratory setting. In contrast, men with ED from endothelial or neurologic deficit—the most common cause of men’s arousal complaints—typically still experience mental sexual arousal/excitement. • Women’s sexual dysfunctions do not link to androgen deficit. • Psychological therapies predominate in the treatment of women’s sexual dysfunctions with emerging evidence of benefit from mindfulness-based cognitive therapy. • About 10% to 15% of women have dyspareunia from provoked vestibulodynia—a chronic pain disorder associated with central sensitization of the nervous system and occasionally precipitated by low-dose combined contraceptives. Endocrine disease and its treatment can frequently disturb sexual function in men and women.1 In addition, patients may believe, often incorrectly, that their sexual dysfunction must necessarily be due to hormonal imbalance and seek management from endocrinologists.2 Patients consider their sexual lives to be important; recognizing the importance of sexual function as a determinant of quality of life, the World Health Organization declared sexual health a fundamental right of men and women. For much of human history, the common beliefs about human sexuality were shaped largely by religious dogma, whose vehemence was rarely justified by the scientific evidence. Alfred C. Kinsey’s pioneering epidemiologic investigations provided the first evidence of the considerable variability in sexual practices of American men and women.3 Excellent epidemiologic surveys, such as the Massachusetts Male Aging Study (MMAS) by Feldman and associates4 and the National Health and Social Life Survey (NHSLS) by Laumann and colleagues,5,6 using modern sampling techniques, revealed high prevalence rates of sexual dysfunction among community-dwelling middle-aged and older men. Ongoing and distressing sexual dysfunction affects 10% of people; prevalence rates are even higher in older men.2,6,7 Temporary or nondistressing dysfunction is frequently reported by up to 40% of the population. 785 786 SECTION V Reproduction William Masters and Virginia E. Johnson8 found that both men and women display predictable physiologic responses after sexual stimulation. These landmark descriptions of the human sexual response cycle by Masters and Johnson provided the basis for a rational classification of human sexual disorders8 (Fig. 20-1A). Sigmund Freud ascribed sexual problems in adult men and women to earlier difficulties in maturation of childhood sexuality and development of parent-child relationships. Recent advances in our understanding of the physiologic and biochemical mechanisms of penile erection and the development of mechanism-specific therapies for ED have largely supplanted Freud’s psychoanalytical theories. The 1980s and 1990s witnessed remarkable progress in our understanding of the physicochemical mechanisms that lead to penile tumescence and rigidity. It was recognized that penile erections are the result of cavernosal smooth muscle relaxation Orgasm and increased penile blood flow.9-11 The appreciation of nitric oxide as a key vasodilator in the vascular smooth muscle was a pivotal discovery, recognized later by awarding of the Nobel Prize in Physiology or Medicine to Robert F. Furchgott, Louis J. Ignarro, and Ferid Murad. The recognition that nitric oxide caused cavernosal smooth muscle relaxation by simulating guanylyl cyclase provided the foundation for the discovery of highly effective oral therapies for the treatment of ED. Historically, the classification and nomenclature for sexual disorders were based on the Diagnostic and Statistical Manual of Mental Disorders (DSM), which is primarily a psychiatric nomenclature, reflecting the belief that sexual disorders in men and women are psychogenic in their origin.12 The DSM and several other expert groups updated the definitions and classification of sexual disorders in the early 1990s.12,13 In May 2013, the DSM-5 (5th edition) Female Plateau Male Excitement Resolution A Multiple incentives for sex Other rewards— emotional intimacy, increased well-being Deliberate attention to stimuli Sexual satisfaction and absence of pain Biologic factors Arousal: Triggers/merges with desire B Arousal: Subjective + ANS response Appraisal of stimuli Psychological factors Figure 20-1 A, Four phases of the human sexual response cycle, as postulated by Masters and Johnson. The resolution phase is prolonged considerably in men such that men may experience refractoriness to further stimulation for varying lengths of time before they can achieve another orgasm. As discussed in the text, our views of the female response cycle have evolved substantially since then (see B). B, Circular human response cycle of overlapping phases. It is being increasingly recognized that there is a lot more complexity, circularity, and flexibility in the human sexual response than is reflected in Masters and Johnson’s original model (A). Human sexual response is depicted as a motivation/incentive-based cycle of overlapping phases of variable order. A sense of desire may or may not be present initially: it can be triggered alongside the sexual arousal resulting from attending to sexual stimuli. Psychological and biologic factors influence the brain’s appraisal of the sexual stimuli. Sexual arousal comprises subjective (pleasure/ excitement/wanting more of the same) and physical (genital and nongenital) responses. The merged desire and arousal influence the ongoing attention to and appraisal of further sexual stimulation. The sexual and nonsexual outcomes influence present and future sexual motivation. ANS, autonomic nervous system. (B, Adapted from Basson R. The female sexual response: the role of drugs in the management of sexual. dysfunction. Obstet Gynecol. 2001;98:350-352.) CHAPTER 20 Sexual Dysfunction in Men and Women further refined the classification and definition of sexual disorders in men and women.14,15 The growing recognition that ED is commonly a manifestation of systemic disease and the availability of easy-touse therapeutic options, including oral and intraurethral drugs, have duly placed sexual disorders in men within the purview of the endocrinologist and the primary care provider. In middle-aged and older men, but less so for women, sexual dysfunction is often related to comorbid medical conditions.7,9,16-18 Sexual dysfunction can be a manifestation of serious underlying medical disease, such as a pituitary neoplasm, diabetes, or coronary artery disease.10,19 ED may signal asymptomatic coronary artery disease.19,20 In women, sexual dysfunction is more strongly linked to mental health.20-22 The clinical definitions of sexual dysfunction, especially in women, remain shrouded in debate. In women, there is poor correlation between a clinician’s diagnosis of sexual dysfunction and a woman’s perception of the problem.23 For instance, in one study,23 about 20% of middle-aged women were given a diagnosis of sexual dysfunction even though they reported no problem, whereas a similar number did not receive a diagnosis of sexual dysfunction but reported problematic sex. This chapter describes the current conceptualization of sexual response in men and women, the underlying pathophysiologic mechanisms, the sexual sequelae of various endocrine disorders, and clinical assessment of sexual dysfunction and its management. Management strategies for sexual dysfunction stemming from hormonal and nonhormonal factors are also outlined. HUMAN SEXUAL RESPONSE CYCLE The traditional model of human sexual response stemming from the research of Masters, Johnson, and Kaplan envisioned a linear progression from desire to arousal to a plateau of high arousal followed by orgasm/ejaculation, followed by a phase of resolution (see Fig. 20-1A).8 In marked contrast to this earlier model depicting a linear invariable progression of discrete phases, recent research conceptualizes sexual response as a motivation/incentivebased cycle comprising phases of physiologic response and subjective experience.24-28 The phases of the cycle overlap and their order is variable (see Fig. 20-1B). The motivations and incentives for sex are multiple and varied. A wish to both demonstrate and enhance emotional intimacy between the partners is important for both men and women. Depression is a major cause of reduced sexual motivation in otherwise healthy persons and in those with endocrine disease: repeatedly, comorbid depression has been identified as a factor underlying increased sexual dysfunction in women with diabetes.26,29,30 Even in the absence of clinical depression, low sexual interest is associated with having more depressed and more anxious thoughts and lower sexual self-image than that in control subjects. Endocrine disorders can markedly lessen sexual self-image especially when associated with altered appearances, infertility, or ability to be gainfully employed.1,26,29,31 Sexual desire, as in lust or drive, is only one of many reasons people engage in sex and may or may not be sensed initially: desire can be triggered by the sexual excitement (i.e., the subjective sexual arousal in response to sexual stimuli).24,26,32,33 Some researchers posit that arousal and desire occur exclusively in response to sexually relevant stimuli and that any internal thoughts or fantasies may also stem from something external. In both men and women, the relationship between desire and arousal is vari- 787 able and complex, and both are often unable to separate the two.34-36 This overlap of phases is in keeping with neuroimaging data of sexual arousal, which have led to the concept that motivation is one facet of sexual arousal and desire is one component of motivation.37 Many factors, psychological and biologic, influence the brain’s appraisal and processing of the sexual stimuli to allow or disallow subsequent arousal.22,26,30,32-34,36-45 The sexual and nonsexual outcomes influence future sexual motivation. The circle depicted in Figure 20-1B may be partially or completely repeated a number of times during any given sexual encounter (i.e., there is true cyclicity).24 Variability is marked between individuals and within a person’s own sexual life, influenced by multiple factors, including stage of life cycle, age, and relationship duration, and robustly linked to mental health and relationship happiness.36 Even with sufficient sexual motivation and the presence of adequate stimuli, the arousal and pleasure may not occur if attention is not focused.41 Review of the literature on sexual arousal in 2009 confirmed a central role for attentional processes in facilitating the subjective and also the physiologic components of sexual arousal.41 Sexual information is processed in the mind both automatically and consciously.42 The sexual nature of the stimuli is processed by the limbic system, allowing genital congestion (observed to be quick and automatic in women and slower but still involuntary in men).42 Conscious appraisal of the sexual stimuli and the contextual cues can lead to subjective arousal.42-45 The latter may be further increased by awareness of the genital congestion of arousal, which is more accurately registered and more relevant to men’s experience than to women’s.24 The subjective arousal will also be cognitively appraised—for instance, is this pleasurable and safe or is this shameful or likely to have a negative consequence?42-45 Cognitions such as these continually modify both the physiologic and subjective responses.42,43 Focusing on nonerotic thoughts during sexual stimulation, generated possibly by anxiety as first suggested by Barlow, is linked to having sexual problems.43 A recent study of men and women in long-term relationships found that women tended to report nonerotic thoughts about their body image and the external consequences of sexual activity, whereas men were more likely to report nonerotic thoughts about problematic sexual performance.44 Both the men and the women in that study had some nonerotic thoughts about the emotional consequences of the sexual activity.44 Regardless of content, the more frequent the nonerotic thoughts, the more sexual dysfunction. Importantly, the more difficult it was to refocus back on an erotic thought, the more this predicted sexual difficulty. This research is clearly relevant to patients with endocrine disease, which frequently has negative impact upon sexual self-image and sexual functioning.26,29 Thus, the current conceptualization of men’s and women’s sexual responses is in marked contrast to an earlier model depicting a linear invariable progression of discrete phases—from desire, to arousal, to a plateau of high arousal, followed by orgasm/ejaculation, and finally a phase of resolution.24,25,46 Women’s sexual dysfunction typically involves lessened arousal and desire and lessened frequency of orgasm, now reflected in the recently coined sexual interest/arousal disorder appearing in the American Psychiatric Association’s Diagnostic and Statistical Manual, 5th edition (DSM-5) (Table 20-1).14,15 Although the focus in men has typically been on ED or premature ejaculation, they too may experience a more generalized sexual distress disorder affecting desire, erectile function, and ease of orgasm.18,45 788 SECTION V Reproduction TABLE 20-1 Current Definitions of Female Sexual Disorders Female Sexual Interest/Arousal Disorder Lack of sexual interest/arousal for a minimum duration of 6 months as manifested by at least three of the following indicators: 1. Absent/reduced frequency or intensity of interest in sexual activity 2. Absent/reduced frequency or intensity of sexual/erotic thoughts or fantasies 3. Absence or reduced frequency of initiation of sexual activity and typically unreceptive to a partner’s attempts to initiate 4. Absent/reduced frequency or intensity of sexual excitement/ pleasure during sexual activity on all or almost all (approximately 75%) sexual encounters 5. Sexual interest/arousal is absent or infrequently elicited by any internal or external sexual/erotic cues (e.g., written, verbal, visual) 6. Absent/reduced frequency or intensity of genital or nongenital sensations during sexual activity on all or almost all (approximately 75%) sexual encounters Female Orgasmic Disorder At least one of the two following symptoms, which must have been present for a minimum duration of approximately 6 months and be experienced on all or almost all (approximately 75%) occasions of sexual activity: 1. Marked delay in, marked infrequency of, or absence of orgasm 2. Markedly reduced intensity of orgasmic sensation Genitopelvic Pain/Penetration Disorder Persistent or recurrent difficulties for a minimum duration of approximately 6 months with one or more of the following: 1. Marked difficulty having vaginal intercourse/penetration 2. Marked vulvovaginal or pelvic pain during vaginal intercourse/ penetration attempts 3. Marked fear or anxiety either about vulvovaginal or pelvic pain on vaginal penetration 4. Marked tensing or tightening of the pelvic floor muscles during attempted vaginal penetration Bancroft and colleagues proposed dual control theories for sexual appraisal both in men and women.47 Their control model envisions a balance between sexual activation and sexual inhibition in an individual’s brain, with this balance determining whether sexual stimulation leads to arousal. A questionnaire was used to characterize the specific factors associated with an individual’s sexual excitation and sexual inhibition. The latter items were identified as the threat of performance failure and the threat of performance consequences (or both) in men, but in women, relationship importance (reflecting the need for sex to be within a specific type of relationship), concerns about sexual function (worries and distractions about sexual function), and arousal contingency (the potential for arousal to be inhibited by contextual/situational factors) were inhibiting factors.47 PHYSIOLOGIC MECHANISMS OF HUMAN SEXUAL RESPONSE Physiology of Desire and Arousal Functional Brain Imaging of Sexual Arousal in Men and Women Although mainly focused on male sexual arousal in response to visual sexual stimuli, functional neuroimaging techniques have clarified some of the neural correlates of sexual response.48-54 Review of some 73 published studies, the majority focused on healthy male heterosexual volunteers, has led to a model that includes multiple facets of sexual arousal.37 Brain imaging during sexual stimulation engages complex circuitry with activation of brain regions related to the different aspects of arousal while other brain regions inhibitory to sexual arousal are deactivated.48-54 In keeping with the current circular model of sexual response (depicting sexual incentives/motivations, information processing, overlap of arousal and desire, emphasis on subjective as well as physiologic arousal, plus importance of reward), the model of sexual arousal emanating from the neuroimaging data comprises cognitive, motivational, emotional, and autonomic components37 (see Fig. 20-1B). The cognitive component includes appraisal of potentially sexual stimuli, focused attention on those stimuli appraised as erotic, and imagery of actual sexual activity. The activations of the right lateral orbitofrontal cortex (OFC), of the right and the left inferior temporal cortices, of the superior parietal lobules, and of areas belonging to the neural network mediating motor imagery (inferior parietal lobules, left ventral premotor area, right and left supplementary motor areas, cerebellum) are considered to be the neural correlates of this cognitive component. The motivational component comprises the processes that direct behavior to a sexual goal, including the perceived urge to express overt sexual behavior. Thus, the motivational component is conceptualized as including the experience of sexual desire. Neural correlates are thought to involve the anterior cingulate cortex (ACC), claustrum, posterior parietal cortex, hypothalamus, substantia nigra, and ventral striatum. The emotional component is the brain activity underlying the pleasure from the mental excitement and the perception of genital and other physical responses. This pleasure comprises liking and wanting.55 The left primary and secondary somatosensory cortices, the amygdalae, and the right posterior insula are conceived as neural correlates of this emotional component. The autonomic and neuroendocrine component includes the various responses (e.g., genital, cardiovascular, respiratory, changes in hormonal plasma levels) that allow preparedness for sexual activity: activations in the anterior cingulate cortex, anterior insulae, putamens, and hypothalamus may contribute to this component. From studying the brain’s deactivations with sexual arousal, three components of inhibition are suggested37: 1. Inhibition mediated by regions in the temporal lobes and the gyrus rectus of the OFC in the resting state. Patients with lesions in the gyrus rectus are noted to have excessive appetite for sexual and other pleasurable activities.56 This together with temporal lobe deacti­ vation is exemplified by the marked hypersexuality of Klüver-Bucy syndrome.57 The deactivated temporal regions are distinct from those activated in response to visual sexual stimuli. 2. Inhibition of arousal once it has begun, to limit its expression because the circumstances are inappropriate, is mediated in the healthy caudate nucleus and putamen. This is consistent with reports of hypersexuality associated with lesions in the head of the caudate nuclei.58 3. Activation of the left OFC is thought to undermine sexual stimuli so as to limit their potential to arouse. It is of interest that these regions thought to mediate inhibition of sexual arousal have been found to be activated during tasks that require moral judgments and those that involve guilt and embarrassment. Future studies focusing more on women and on nonheterosexual persons are awaited. Of note, men generally show greater responsiveness to visual sexually arousing stimuli than do women.46 Moreover, the complexity and CHAPTER 20 Sexual Dysfunction in Men and Women variability of these systems was reflected in a study of surgically menopausal women who were sexually active but were receiving no hormonal therapy.49 When these women viewed erotica during functional magnetic resonance imaging (MRI), they failed to display the brain activation observed in premenopausal women or in themselves when they were treated with testosterone and estrogen; yet, they reported sexual arousal from the erotic videos, both without and with hormonal supplementation.49 Functional imaging during penile or clitoral stimulation to orgasm indicates that women show more activation in left frontoparietal regions, notably in the posterior parietal cortex and the supplementary motor area—regions associated with making a mental representation of another person’s actions.50 It is suggested that these findings may reflect gender differences in perspective and empathy, and that men and women use different cerebral strategies to reach orgasm—the brain responses during the orgasm(s) themselves being similar in men and women.50 Preliminary research has been published into functional and structural neural correlates of persons with low sexual desire. Reduced activation bilaterally in the entorhinal cortices and increased activation in the right medial frontal gyrus and right inferior frontal gyrus and bilaterally in the putamen was observed in women with DSM-IV hypoactive sexual desire disorder (HSDD) as compared to control subjects in response to erotic videos.51 In keeping with the motivation-based sex response cycle in which processing of sexual information is crucial to subjective and physiologic response, the authors suggest that encoding of erotic stimuli and retrieval of past erotic experiences (entorhinal cortices) differed between the two groups. Additionally, the increased activation in medial and inferior frontal gyri may reflect increased monitoring of sexual responses, which is well documented in women with HSDD. Studying gray matter volume and white matter fractional anisotropy, researchers recently identified changes in women with HSDD as compared to control subjects.52 Whether this is cause or effect of the sexual dysfunction remains unclear, but the observed changes suggested HSDD to be linked to attribution of reduced importance to sexual stimuli (amygdala and occipitotemporal cortex), reduced awareness of sexual response (insula, anterior temporal cortex), and altered attention to, and inhibition of, sexual responses (anterior cingulate cortex, dorsolateral prefrontal cortex).52 Evidence of reversal of these changes with effective treatment is awaited. That structural changes associated with chronic pain can reverse with therapy is encouraging and suggests that anatomic as well as functional changes may reflect rather than control experience.53 Brain imaging in hypogonadal men before and after treatment suggests that the left OFC might exert a testosterone-dependent inhibitory tonic control on sexual arousal and that this control decreases upon visual sexual stimulation.54 Also the response of the right anterior insula to visual sexual stimulation was found to depend on the level of plasma testosterone.54 Neurotransmitters and Hormones Involved in Sexual Desire and Subjective Arousal A variety of hormones and peptides are involved in the sexual response. The interplay among androgens and neurotransmitters is complex59-69: androgens influence neurotransmitter release, and neurotransmitters may modulate androgen receptor signaling.46,61,63 The role of testosterone in desire and arousal is better documented in men than in women.62,63 Serum levels of testosterone do not correlate with women’s sexual function according to large 789 epidemiologic studies.63-66 The radioimmunoassays used to measure testosterone concentrations in many epidemiologic studies were designed to measure the substantially higher levels of testosterone in men and lacked the sensitivity, precision, and accuracy in the low range prevalent in women. When a more sensitive mass spectrometrybased assay was used in a study of women with low desire and low subjective arousal and women in a control group, researchers found no difference in serum testosterone levels between the groups.66 Additionally, it has been difficult to measure intratissue testosterone levels and activity. Labrie and associates have proposed the measurements of androgen metabolites—most notably androsterone glucuronide (ADT-G)—as markers of ovarian plus intracrine androgen activity. Circulating ADT-G levels decrease with age.67 Serum ADT-G levels did not differ significantly between 121 women with low desire and 124 women without low desire.66 Thus, a link between low desire and low androgen activity as reflected by serum testosterone levels or androgen metabolites has not been identified to date. Animal Models. In animal models, steroid hormones modulate sexual arousal by directing synthesis of the enzymes and the receptors for a number of neurotransmitters, including dopamine, noradrenalin, melanocortin, and oxytocin.59,60,68-71 Systems that act within the hypothalamus and limbic regions of the brain are involved in the process of arousal, attention, and sexual behavior. It is thought that dopamine transmission in the medial preoptic area (MPOA) and the nucleus accumbens focuses the person’s attention on sexual stimuli (the incentives or motivations for sexual activity). It is postulated that the behavioral pattern stimulated by those systems and the subjective feelings that accompany them constitute the phenomenon commonly referred to as sexual desire or arousal when genital sensations triggered by these systems are subjectively felt. The main part of this neural pathway includes the MPOA and its outputs to the ventral tegmental area. The latter contains dopamine cell bodies that project to various limbic and cortical regions, including the prefrontal cortex, the nucleus accumbens, the anterior cingulate cortex, and the amygdala. Brain pathways for sexual inhibition include opioid, endocannabinoid, and serotonin neural transmissions feeding back to various levels of the excitatory pathways.60,61 It is thought that the behavioral pattern stimulated by the inhibitory pathways includes both sexual reward and satiety refractoriness. Exogenous opiates are sexually inhibiting independent of their inhibitory effect on luteinizing hormone (LH), LH-releasing hormone, and testosterone.70 Endogenous opioids modulate the feedback effects of sex steroids on the hypothalamus and pituitary.70 β-Endorphin is synthesized in the anterior pituitary, the hypothalamus, and the nucleus of the tractus solitarius in the brainstem. The sexual inhibiting effects of opioids occur mainly through their action in the MPOA and the amygdala.70 Low doses of opiates can have facilitatory effects, possibly through actions in the ventral tegmental area to activate the mesolimbic dopamine system. Exogenous opiates can induce an intense feeling of pleasure, which has been likened to orgasm, followed by a state of relaxation and calm.71 Melanocortins are derived from pro-opiomelanocortin and modulate sexual response through a specific receptor subtype, the melanocortin-4 receptor. Administration of melanocortin receptor agonists has been associated with an increase in spontaneous erections in healthy men and in men with ED, and with increased desire, but not genital responses, in women.72,73 790 SECTION V Reproduction Oxytocin levels increase close to orgasm. This hormone is known to be involved in pair bonding in some animal species, but its relevance in humans is unclear. The physiologic role of prolactin in the human sexual response remains uncertain.74-76 Because a generalized reduction of dopamine activity in the hypothalamus results in increased prolactin secretion, it has been difficult to distinguish between the effects of raised prolactin itself and the possible effects of the reduced dopamine transmission. High levels of prolactin are associated with impaired sexual function in men and women.70,76 The effects of the biologic factors are intertwined with those of the environmental and social factors. For instance, dopamine and progesterone, acting on their cognate receptors in the hypothalamus, can increase sexual behavior in oophorectomized, estrogenized female rats, and the presence of a male animal alongside the cage can cause an identical stimulation of the sexual behavior without the administration of either progesterone or dopamine.77 In rodents, birds, and fish, complex neural networks enable the animal to assess the context of potential sexual activity and relate it to past experience and to expectation of reward.78 Men and women differ substantially with respect to the correlation between genital congestion and subjective sexual arousal (excitement). Whereas subjective arousal is typically concordant with genital congestion in men, there is a poor correlation between subjective arousal and measures of genital congestion in women.79 There are some exceptions in men: sleep-related erections are mostly dissociated from erotic dreams or from subjective sexual arousal.80 Also psychophysiologic studies have found that men can get erections in response to films of assault or rape while experiencing no subjective arousal.81 In contrast, a psychophysiologic study identified some 25% of men in a community sample with minimal penile response to an erotic video while their subjective arousal was similar to the remaining 75% of men with recorded penile congestion. Devaluing stimuli Emotional Pleasure from subjective arousal and from sensations including genital congestion Physiologic Mechanisms of Penile Erection Penile Anatomy and Blood Flow Genital Sexual Congestion and Arousal Focused attention Given the consistent finding of low sexual concordance in women, a correlation with reduced interoception (awareness of nonsexual physiologic states, e.g., awareness of heart rate) was suspected but not identified.82 In contrast to men’s typically accurate assessment of their erections, women’s assessment of their degree of genital congestion is less accurate. It is thought that genital congestion in women is a prompt, automatic reflex that occurs within seconds of an erotic stimulus; it may not be deemed at all sexually arousing by the woman, or it may even be deemed emotionally negative.83 Viewing primates engaging in sexual activity subjectively arouses neither young men nor young women.79 However, the young women viewing primate sex display marked genital congestion, as measured by vaginal photoplethysmography (VPP), whereas no genital response occurs in the men. Similarly, heterosexual women viewing lesbian women engaged in sexual activity report mostly low subjective arousal but show a prompt vasocongestive response; in contrast, heterosexual men viewing male same-sex activity show minimal genital or subjective response.79 The erectile tissue of the penis consists of two dorsally positioned corpora cavernosa and a ventrally placed corpus spongiosum.10,11,84,85 The erectile tissue of both the corpora cavernosa and corpus spongiosum is composed of numerous cavernous spaces separated by trabeculae.10,11,84,85 These trabeculae are composed mainly of smooth muscle cells that are arranged in a syncytium. Endothelial cells cover the surfaces of the trabeculae. The penile arterial blood supply is derived from pudendal arteries, which are branches of the internal iliac arteries (Fig. 20-2). The pudendal artery divides into cavernosal, dorsal penile, and bulbourethral arteries. The cavernosal arteries and their branches, the helicine arteries, provide blood flow to corpora cavernosa.10,11 Dilatation of the helicine arteries increases blood flow and pressure in the cavernosal sinuses.10,11,84,85 Censoring arousal to prevent sexual behavior Cognitive Appraisal of sexual stimuli Motivational Expectation of sexual and nonsexual rewards Desire triggered Imagery of sexual acts Autonomic Unconscious reflex becomes a conscious reinforcing stimulus especially in men Figure 20-2 Brain areas activated during sexual arousal allow (1) continued focus on sexual stimuli, imaging of sexual behavior, evaluation/censorship, and limitation or prevention of actual behavior despite arousal (all constituting a cognitive component of arousal), (2) sexual feelings (an emotional component), (3) anticipation of reward (a motivational component), and (4) an autonomic/neuroendocrine response of physical sexual arousal. (Adapted from Basson R, Weijmar Schultz W. Sexual sequelae of common medical conditions. Lancet. 2007;369:409-424.) CHAPTER 20 Sexual Dysfunction in Men and Women 791 TABLE 20-2 Innervation of the Penis Types of Fibers Location of Neurons in the Spinal Cord Sympathetic T10-L2 Parasympathetic Somatic S2-S4 S2-S4 Nerves Carrying the Fibers General Function Prevertebral outflow through the hypogastric and cavernous nerves; additionally, paravertebral outflow through the parasympathetic ganglia, and pudendal or pelvic and cavernous nerves Cavernosal and pelvic nerves Pudendal nerve Generally antierectile; sympathetic innervation plays an important role in regulating seminal emission Proerectile Penile sensation, contraction of the striated muscles during ejaculation Penile Innveration The neural input to the penis consists of sympathetic (T11L2), parasympathetic (S2-S4), and somatic nerves (Table 20-2).85 Sympathetic and parasympathetic fibers converge in the inferior hypogastric plexus where the autonomic input to the penis is integrated and communicated to the penis through cavernosal nerves. In man, the inferior hypogastric ganglionic plexus is located retroperitoneally near the rectum.11,85 Several brain regions, including amygdala, MPOA, paraventricular nucleus of the hypothalamus, and periaqueductal gray matter act coordinately to affect penile erections.85 The MPOA of the hypothalamus serves as the integration site for the central nervous system control of erections; it receives sensory input from the amygdala and sends impulses to the paraventricular nuclei of the hypothalamus and the periaqueductal gray matter. Neurons in paraventricular nuclei project onto the thoracolumbar and sacral nuclei associated with erections. The parasympathetic input to the penis is proerectile, and sympathetic input is mainly inhibitory.85 The stimuli from the perineum and lower urinary tract are carried to the penis through the sacral reflex arc.85 Hemodynamic Changes During Penile Erection Penile erection results from a series of biochemical and hemodynamic events that are associated with activation of central nervous system sites involved in regulation of erections, relaxation of cavernosal smooth muscle, increased blood flow into cavernosal sinuses, and venous occlusion resulting in penile engorgement and rigidity.10,84 Normal penile erection requires coordinated involvement of intact central and peripheral nervous systems, corpora cavernosa and spongiosa, and normal arterial blood supply and venous drainage.10,84 As cavernosal smooth muscle relaxes and the blood flow to the penis increases, the increased pooling of blood in the cavernosal spaces results in penile engorgement10,84 (Fig. 20-3). The expanding corpora cavernosa compress the venules against the rigid tunica albuginea, restricting the venous outflow from the cavernosal spaces.10,84 This facilitates entrapment of blood in the cavernosal sinuses, imparting rigidity to the erect penis. Biochemical Regulation of Cavernosal Smooth Muscle Tone The tone of the corporal smooth muscle cells determines the erectile state of the penis.10,11,84 When the cavernosal smooth muscle cells are relaxed, the penis is engorged with blood and erect. When the cavernosal smooth muscle cells are contracted, there is predominance of sympathetic neural activity, and the penis is flaccid.85 The smooth muscle tone in the corpora cavernosa is maintained by the release of stored intracellular calcium into the cytoplasm and influx of calcium through membrane channels.86-89 The transmembrane influx of calcium in the cavernosal smooth muscle cells is mediated mostly by L-type voltage-dependent calcium channels, although T-type calcium channels are also expressed in cavernosal smooth muscle cells.86-89 An increase in intracellular calcium activates myosin light chain kinase resulting in phosphorylation of myosin light chain, actin-myosin interactions, and smooth muscle contraction.89 The transmembrane and intracellular calcium flux in the cavernosal smooth muscle cells is regulated by a number of cellular processes that involve K+ flux through potassium channels, connexin43-derived gap junctions, and a number of cholinergic, adrenergic, and noradrenergic noncholinergic mediators (Figs. 20-4 to 20-6).86-94 The nonadrenergic noncholinegic mediators include vasoactive intestinal peptide (VIP), calcitonin gene–related peptide (CGRP), and nitric oxide.94 Prostaglandin E1 (PGE1) binding to its cognate receptor results in generation of cyclic adenosine monophosphate (cAMP), which activates protein kinase A. Activated protein kinase A stimulates K+ channels, resulting in K+ efflux from the cell (see Fig. 20-4). The protein kinase A–mediated processes also result in a net decrease in intracellular calcium, favoring smooth muscle cell relaxation. Adrenergic pathways, acting through norepinephrine and α1-adrenergic receptors, activate phospholipase C, which generates diacyl glycerol and inositol triphosphate (IP3).89 Diacyl glycerol activates protein kinase C, which inhibits K+ channels and activates transmembrane calcium influx by activating L-type calcium channels (see Fig. 20-5).90,91 Inositol triphosphate increases intracellular calcium by promoting the release of calcium from intracellular calcium stores.90,91 The net increase in intracellular calcium promotes actin-myosin interactions, resulting in smooth muscle contraction and a flaccid penis. Potassium Channels. At least three types of potassium channels—ATP-sensitive (KATP), voltage-gated (Kv), and calcium-sensitive K+ channels (referred to as BKCa or maxi-K channels)—are expressed in the cavernosal smooth muscle cells.92,93 Of these, the BKCa channels are the most important, as they account for 90% of K+ efflux from the cavernosal smooth muscle cells. BKCa channel openers have been shown to relax cavernosal smooth muscle cells in vitro.93 Thus, the strategies that increase BKCa channel expression in vivo improve erectile capacity in diabetic and older rodents93-95 and are being explored as therapy for ED. A phase I human gene therapy trial using this approach has shown the feasibility of this approach.95 Connexin43 Gap Junctions. The smooth muscle cells in the corpora cavernosa are connected by connexin43 gap junctions that allow the ions and some signaling molecules 792 SECTION V Reproduction Prostate Cavernous nerve (autonomic) Deep dorsal vein Dorsal artery Dorsal nerve (somatic) Circumflex artery Dorsal artery Circumflex vein Tunica albuginea Dorsal nerve (somatic) Deep dorsal vein Sinusoidal spaces Circumflex vein Sinusoidal spaces Helicine arteries Helicine arteries Corpora cavernosa Trabecular smooth muscle Cavernous artery Flaccid Erect Subtunical venular plexus Figure 20-3 Anatomy and mechanism of penile erection. Corpora cavernosa are made up of trabecular spaces that are surrounded by cavernosal smooth muscle. Helicine arteries provide the arterial supply to the cavernosal spaces. The dorsal nerve provides the sensory innervation to the penis. During erection, the relaxation of the trabecular smooth muscle and increased blood flow result in engorgement of the sinusoidal spaces in the corpora cavernosa. The expansion of the sinusoids compresses the venous return against the tunica albuginea, resulting in entrapment of blood, which imparts rigidity to the tumescent penis. (Adapted from Lue TF. Erectile dysfunction. N Engl J Med. 2000;342(24):1802-1813.) such as inositol triphosphate to diffuse freely across smooth muscle cells96 (Fig. 20-7). The ionic changes induced by a stimulus in one smooth muscle cell are communicated rapidly across other smooth muscle cells, resulting in coordinate regulation of the entire corpora cavernosa.96 Thus, corpora cavernosa can be viewed functionally as a syncytium of interconnected smooth muscle cells (see Fig. 20-7).96 Nitric Oxide. Nitric oxide, derived from the nerve terminals innervating the corpora cavernosa, endothelial lining of penile arteries, and the cavernosal sinuses, is an important biochemical regulator of cavernosal smooth muscle relaxation. Nitric oxide also induces arterial dilatation.97 The actions of nitric oxide on the cavernosal smooth muscle and the arterial blood flow are mediated through the activation of guanylyl cyclase, the production of cyclic guanosine monophosphate (cGMP), and the activation of cGMP-dependent protein kinase (also called protein kinase G, or PKG) (see Fig. 20-6). cGMP causes smooth muscle relaxation by lowering intracellular calcium. There is some evidence that nitric oxide inhibits Rho kinase–induced cavernosal smooth muscle sensitivity to calcium.98 Cyclic Nucleotide Phosphodiesterases. Cyclic nucleotide phosphodiesterases hydrolyze cAMP and cGMP, thus reducing their concentrations within the cavernosal smooth muscle. Of the 13 or more isoforms of cyclic nucleotide phosphodiesterases that have been identified, isoforms 2, 3, 4, and 5 are expressed in the penis.99-106 Only phosphodiesterase 5 (PDE5) is specific to the nitric oxide/cGMP pathway in the corpora cavernosa.99-106 Hydrolysis of cGMP by this enzyme results in reversal of the smooth muscle relaxation and reversal of penile erection (see Fig. 20-6). Sildenafil, vardenafil, and tadalafil are potent and selective inhibitors of the activity of PDE5 that prevent breakdown of cGMP and thereby enhance penile erection9,10 (see Fig. 20-6). Regulation of Sensitivity to Intracellular Calcium by Rho A/Rho Kinase Signaling. Recently, considerable attention has focused on the role of Rho kinase in modulating the sensitivity of cavernosal smooth muscle to intracellular calcium.107 A growing body of evidence suggests that sensitization to intracellular calcium is regulated by the balance between phosphorylation of the regulatory light chain of myosin II by a myosin light chain kinase and its dephosphorylation by a myosin light chain phosphatase (Fig. 20-8).107-112 Phosphorylation of regulatory light chain of myosin II is necessary for activation of myosin II adeno­ sine triphosphatases (ATPases) by actin, and its dephosphorylation prevents activation of myosin II ATPases.107-112 The ratio of the kinase to phosphatase activities is an CHAPTER 20 Sexual Dysfunction in Men and Women PGE1 793 NE G + cAMP + PKA + – K+ K+ [Ca2+]i – + DAG + PKC IP3 + [Ca2+]i K+ Ca2+ K+ Ca2+ + Ca2+ Figure 20-4 Regulation of cavernosal smooth muscle contractility by prostaglandin E1 (PGE1). Relaxation of the cavernosal smooth muscle is regulated by intracellular 3′,5′-cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP). These intracellular second messengers, by activating specific protein kinases, cause sequestration of intracellular calcium (Ca2+) and closure of Ca2+ channels and opening of potassium K+ channels. This results in a net decrease in intracellular Ca2+, leading to smooth muscle relaxation. PGE1, by binding to PGE1 receptors, increases the intracellular concentrations of cAMP, which activates protein kinase A (PKA). PKA promotes the sequestration of intracellular Ca2+, inhibits Ca2+ influx, and stimulates K+ channels. The net result is a decrease in intracytoplasmic Ca2+ and smooth muscle relaxation. PGE1 stimulates cAMP generation. (Adapted from Bhasin S, Benson GS. Male sexual function. In: De Kretser D, ed. Knobil and Neill’s Physiology of Reproduction, 3rd ed. Boston, MA: Academic Press; 2006:1173-1194; and Lue TF. Erectile dysfunction. N Engl J Med. 2000;342:1802-1813.) Ca2+ Figure 20-5 Regulation of cavernosal smooth muscle contractility by norepinephrine (NE), which mediates adrenergic signals, binds to adrenergic receptors, and stimulates diacyl glycerol (DAG) and inositol 1,4,5-triphosphate (IP3). DAG stimulates protein kinase C (PKC), which, along with IP3, causes an increase in intracytoplasmic calcium (Ca2+) and inhibition of potassium (K+) channels. Increased intracellular Ca2+ causes cavernosal smooth muscle contraction and loss of penile erection. (Adapted from Bhasin S, Benson GS. Male sexual function. In: De Kretser D, ed. Knobil and Neill’s Physiology of Reproduction, 3rd ed. Boston, MA: Academic Press; 2006:11731194; and Lue TF. Erectile dysfunction. N Engl J Med. 2000;342:1802-1813.) Ca2+ Ca2+ Ca2+ Ca2+ Ca2+ Ca2+ Sildenafil PDE5 Tadalafil Inhibitors Vardenafil NO K+ – GTP 5'-GMP Guanylyl cyclase PDE5 cGMP cGMP-dependent kinases Proteins Phosphoproteins Sequestration of intracellular calcium Smooth muscle relaxation Figure 20-6 Regulation of cavernosal smooth muscle relaxation by nitric oxide (NO). Cyclic guanosine monophosphate (cGMP) regulates cavernosal smooth muscle relaxation by promoting sequestration of cytoplasmic calcium. NO is released from noradrenergic norcholinergic nerve endings and possibly from the endothelium. NO activates guanylyl cyclase, which generates cGMP from guanosine triphosphate (GTP), which in turn activates cGMP-dependent kinases, resulting in sequestration of intracellular calcium and smooth muscle relaxation. cGMP is degraded by cyclic nucleotide phosphodiesterases. Sildenafil, vardenafil, and tadalafil are selective inhibitors of phosphodiesterase isoform 5 (PDE5), which is present in cavernosal smooth muscles. (Adapted from Bhasin S, Benson GS. Male sexual function. In: De Kretser D, ed. Knobil and Neill’s Physiology of Reproduction, 3rd ed. Boston, MA: Academic Press; 2006:1173-1194; and Lue TF. Erectile dysfunction. N Engl J Med. 2000;342:1802-1813.) Figure 20-7 The interconnection of cavernosal smooth muscle cells in the penis. Connexin43-derived gap junctions connect adjacent corporal smooth muscle cells and allow flow of ions among interconnected smooth muscle cells. Therefore, alterations in action potential and potassium-channel activity in any myocyte affect the adjacent myocytes. Ca2+, calcium ions; K+, potassium ions. (Adapted from Melman A, Christ GJ. Integrative erectile biology: the effects of age and disease on gap junctions and ion channels and their potential value to the treatment of erectile dysfunction. Urol Clin North Am. 2001;28:217-230.) 794 SECTION V Reproduction Myosin II RLC20 MLCK Ca.CaM Rho kinase MLC phosphatase Inactive MLC phosphatase Myosin II RLC20-P Cavernosal smooth muscle contraction and sensitivity to intracellular Ca2+ Figure 20-8 The role of Rho A/Rho kinase in regulation of cavernosal smooth muscle sensitivity to intracellular calcium (Ca2+). Sensitivity to calcium and smooth muscle contractility is regulated by the Rho A/Rho kinase system. The balance between phosphorylation (P) of myosin regulatory light-chain (myosin II RLC20) kinase and its dephosphorylation by a myosin light-chain (MLC) phosphatase is a major determinant of the smooth muscle sensitization to Ca2+. By inhibiting the activity of MLC phosphatase, Rho kinase, the downstream effector of Rho A, can regulate smooth muscle responsiveness to calcium. Ca.CaM, calcium calmodulin. (Adapted from Somlyo AP, Somlyo AV. Ca2+ sensitivity of smooth muscle and nonmuscle myosin II: modulated by G proteins, kinases, and myosin phosphatase. Physiol Rev. 2003;83: 1325-1358.) important determinant of the contractile sensitivity of the cavernosal smooth muscle cell to intracellular calcium.109 Rho A is a guanosine triphosphatase (GTPase) of approximately 20 kDa that modulates Rho kinase activity, myosin light chain phosphorylation, and calcium sensitivity in smooth muscle cells.107 Rho A–GDP (guanosine diphosphate) complex is associated with a GDP dissociation inhibitor (RhoGDI) in its inactive state. A number of intracellular signals can promote an exchange of GDP for GTP on Rho A through the mediation of guanine nucleotide exchange factors.107-112 The Rho A–GTP interacts with its downstream effector Rho kinase,107-112 increasing the sensitivity of vascular smooth muscle to intracellular calcium by inhibiting the myosin light chain phosphatases. Although the Rho A/Rho kinase expression is not significantly different between young and older rats, the activity of Rho kinase is higher in older rats than in young rats111; the age-related increase in Rho kinase activity has been proposed as one possible mechanism to explain the agerelated decrease in erectile capacity.111 Inhibition of Rho kinase activity in experimental animals increases cavernosal smooth muscle relaxation and improves intracavernosal pressures and penile erections. Therefore, inhibitors of Rho A/Rho kinase signaling promise to provide attractive targets for the development of therapies for ED.111,112 Mechanisms of Ejaculation The ejaculatory mechanisms consist of three processes: emission, ejection, and orgasm.113-116 Although orgasm and seminal fluid ejection often occur contemporaneously, these two processes are regulated by separate mechanisms. Emission, the deposition of seminal fluid into the posterior urethra, is dependent upon the integrity of the vasa deferentia, seminal vesicles, prostate gland, and the bladder neck.115,116 Ejaculation refers to the ejection of seminal fluid containing sperm, and the secretions of seminal vesicles, prostate, and bulbourethral glands from the posterior urethra out through the urethral meatus, and is regulated primarily by the central nervous system activation of the sympathetic nervous system.115 This emission is ejaculated out of the urethra by the contractions of the bulbospongiosus and levator ani muscles, the closure of the bladder sphincter due to sympathetic activation, and synchronized opening of the external urinary sphincter.111 The sensation associated with the rhythmic contractions of these pelvic floor muscles is referred to as the orgasm. The stria terminalis, the posteromedial amygdala, the subparafascicular thalamus, the MPOA of the hypothalamus, the periaqueductal gray matter in the midbrain region, and the paragigantocellular nucleus in the pons integrate seminal fluid emission and ejection during copulatory behavior117,118 (see Table 20-2). The paragigantocellular nucleus in the pons through serotonergic pathways inhibits the lumbosacral motor nuclei that are involved in ejaculation118,119; the input from the MPOA to paragigantocellular nucleus causes loss of this inhibition, resulting in ejaculation.118,119 An ejaculation generator in the spinal cord integrates the central and peripheral sympathetic and parasympathetic signals to control ejaculation.113,118 The parasympatheric fibers from the spinal ejaculation generator feed into the sacral parasympathetic nucleus and are carried from there through the pelvic nerve and the major parasympathetic ganglion into the seminal tract.118 Sympathetic fibers are carried from the spinal ejaculation generator into the dorsal gray commissure and intermediolateral cell column and then through the lumbar sympathetic chain, pelvic nerve, superior hypogastric plexus, and major pelvic ganglion onto the seminal tract.118 Neural pathways that utilize serotonin (5-hydroxytryptamine, 5-HT) and dopamine as neurotransmitters play an important role in regulating ejaculation.115 Thus, administration of selective serotonin reuptake inhibitors (SSRIs) is being explored for the treatment of premature ejaculation.117-120 At least 14 different serotonin receptor subtypes have been identified in different brain regions; 5-HT1A somatodendritic receptors in the mesencephalic and medullary raphe nuclei reduce ejacu­latory latency.113 A better understanding of the neurochemical mechanisms that regulate ejaculation may provide mechanism-specific targets for treatment of ejaculatory disorders. THE ROLE OF TESTOSTERONE IN REGULATING SEXUAL FUNCTION IN MEN Testosterone regulates many domains of sexual function in men and women.1 Although androgen-deficient men can achieve penile erections in response to visual erotic stimuli, their overall sexual activity is decreased.121 Spontaneous but not stimulus-bound erections are testosteroneresponsive (Table 20-3).121 Testosterone promotes sexual thoughts and desire54,121-127 and increases sexual arousal and attentiveness to erotic auditory and other stimuli.122,123 Nocturnal erections, temporally related to peaks of nighttime testosterone secretion, are of lower amplitude and duration in androgen-deficient men, and testosterone therapy increases the frequency, fullness, and duration of nocturnal penile tumescence.127,128 Maximum rigidity may require a threshold level of androgen activity.129-133 Testosterone regulates nitric oxide synthase (NOS) in the cavernosal smooth muscle,130,131 exerts trophic effects on cavernosal smooth muscle132 and ischiocavernosus and bulbospongiosus muscles, and is necessary for the venoocclusive response.129-132 Androgen-deficient men show delayed orgasm and low ejaculatory volume.1 Testosterone therapy in androgen-deficient men improves overall sexual activity, sexual desire, spontaneous CHAPTER 20 Sexual Dysfunction in Men and Women TABLE 20-3 Domains of Sexual Function Regulated by Testosterone* Domains of Sexual Function That Have Been Shown to Improve in Response to Testosterone Therapy of Androgen-Deficient Men 1. 2. 3. 4. 5. 6. 7. Sexual desire Spontaneous sexual thoughts Attentiveness to erotic auditory stimuli Frequency of nighttime and daytime erections Duration, magnitude, and frequency of nocturnal penile erections Overall sexual activity scores Volume of ejaculate Domains of Sexual Function That Have Not Been Shown to Improve in Response to Testosterone Therapy or for Which There Is Insufficient or Inconclusive Evidence 1. Erectile response to visual erotic stimulus 2. Erectile function in men who have normal or low-normal testosterone levels 3. Therapeutic response to selective phosphodiesterase inhibitors 4. Ejaculatory dysfunction 5. Orgasms *Testosterone administration in androgen-deficient men improves overall sexual activity scores through its effects on specific domains of sexuality. From Bhasin S, Enzlin P, Coviello A, et al. Sexual dysfunction in men and women with endocrine disorders. Lancet. 2007;369:597-611, used with permission. sexual thoughts, and attentiveness to erotic auditory stimuli; frequency of nighttime and daytime erections; duration, magnitude, and frequency of nocturnal penile erections; overall sexual activity scores; and the volume of ejaculate.1,54,121-124,127-129,133-136 However, testosterone does not improve erectile response to visual erotic stimulus121 or erectile function in men with ED who have normal testosterone levels.133-136 Brain imaging studies suggest that processing of sexual stimuli may be altered in androgen-deficient men with decreased activation in those brain areas that typically are activated in eugonadal men and in androgen-deficient men after testosterone replacement in response to erotic stimuli.54 Acting on dopaminergic receptors in the MPOA of the hypothalamus, testosterone elicits reward-seeking behavior in male mammals.60 This may be the basis for testosterone’s motivational effects on mammalian sexual behavior.60 The roles of cytochrome P450 (CYP19) aromatase and steroid 5α-reductase systems in mediating androgen effects on sexual function remain incompletely understood.62 Recent studies suggest that 5α-reduction of testosterone to 5α-dihydrotestosterone is not essential for mediating testosterone’s effects on desire or erectile function in eugonadal men.137 Recent investigations, including those in men with mutations of the CYP19A gene suggest that aromatization to estradiol may be important in mediating testosterone’s effects on sexual desire.138-140 Androgen deficiency and ED are two independently distributed disorders that may coexist in middle-aged and older men.141-143 Selective phosphodiesterase inhibitors (PDE5Is) are highly effective first-line therapies for ED. However, one third of men with ED do not respond to PDE5 inhibitors; some of the men with ED who are PDE5 inhibitor nonresponders have low testosterone levels. Observations that testosterone stimulates penile NOS, increases penile blood flow, and has trophic effects on cavernosal smooth muscle and bulbo­ spongiosus and ischiocavernosus muscles have led to speculation that testosterone therapy might improve erectile response to PDE5 inhibitors.144-147 Spitzer and associates148 795 evaluated whether the addition of testosterone to sildenafil improves erectile response in men with ED and low testosterone. In this randomized controlled trial, after optimization of sildenafil dose during an initial run-in period, subjects were assigned randomly to 14 weeks of daily testosterone or placebo gel. Sildenafil plus testosterone was not superior to sildenafil plus placebo in improving erectile function in men with ED and low testosterone.148 In another placebo-controlled trial (TADTEST) of men with ED who were deemed tadalafil (Cialis) failures,149 the primary analysis of all randomized subjects also did not show a significantly greater improvement in erectile function in the testosterone arm than in the placebo arm. However, in post hoc analysis, erectile function improved with the addition of testosterone in a subset of men with baseline testosterone of 10 nmol/L or less (300 ng/dL).149 Thus, randomized trials have failed to support the hypothesis that addition of testosterone to PDE5 inhibitor improves erectile function in men with ED. Sildenafil alone raises testosterone levels presumably because of its direct effects on Leydig cell steroidogenesis.150 PHYSIOLOGY OF PHYSICAL SEXUAL AROUSAL IN WOMEN: GENITAL CONGESTION A number of physical changes accompany women’s sexual excitement (i.e., their subjective sexual arousal), including genital swelling, increased vaginal lubrication, breast engorgement, and nipple erection; increased skin sensitivity to sexual stimulation; changes in heart rate, blood pressure, muscle tone, breathing, and temperature; and mottling of the skin with a sexual flush of vasodilatation over the chest and face.151 These changes are reflexive, mediated by the autonomic nervous system. Within seconds there is increased blood flow to the vagina: vasodilatation of the arterioles in the submucosal plexus that increases transudation of interstitial fluid from the capillaries across the epithelium and into the vaginal lumen.151 Simultaneously, there is relaxation of smooth muscle cells around the clitoral sinusoids, which promotes congestion. MRI studies have confirmed the presence of extensive clitoral tissue far beyond the visible portion of the clitoris.152 The clitoris comprises the head, the shaft, the rami that extend along the pubic arch and the periurethral tissue in front of the anterior vaginal wall, as well as the bulbar tissue that surrounds the anterior distal vagina and is contiguous with the periurethral tissue.152 As the clitoris becomes more swollen, it elevates to lie nearer the symphysis pubis. The vagina lengthens and dilates during arousal, elevating the uterus. The labia become swollen and darker red, and the lower third of the vagina swells.152 The autonomic nerves subserving the widespread genital congestion are at risk from gynecologic surgeries that sever the cardinal ligaments and the uterosacral ligaments to potentially injure Frankenhauser’s nerve plexus and the uterovaginal nerve plexus.153,154 Whereas intrafascial abdominal hysterectomy involves an incision and clamping of the pubocervical fascia to sever the dense attachment of cardinal and uterosacral ligaments, thereby interrupting a major support system and nerve plexuses, intrastromal hysterectomy does not involve cutting or clamping the cardinal ligament, uterosacral ligament, or fascia. A 2013 study confirmed ongoing sexual satisfaction after this procedure.153 Transvaginal tapes for urinary incontinence may also compromise the autonomic nerves between anterior vaginal wall and bladder.154 796 SECTION V Reproduction When increases in genital congestion in response to visual erotic stimuli were recorded using vaginal photoplethysmography, the correlation between genital congestion and subjective arousal are found to be highly variable.50,79 This is true in sexually healthy women and in women reporting a lack of desire or arousal or sexual pain. Women reporting chronic lack of arousal show prompt increases in vaginal congestion, comparable to those in control women, but report no subjective sexual excitement in response to the erotic stimulation. Functional MRI studies show that, unlike in men, activation of the areas organizing genital vasocongestion in women does not correlate with subjective excitement.50,155 The neurobiology of the genital vasocongestive response in women is complex and incompletely understood. Involved is release of nitric oxide and VIP from the parasympathetic nerves.156 Acetylcholine, which blocks noradrenergic vasoconstricting mechanisms and promotes nitric oxide release from the endothelium, is also released. There is communication between the nitric oxide–containing cavernous nerve to the clitoris and the distal portion of the somatic dorsal nerve of the clitoris from the pudendal nerve. Pelvic sympathetic nerves release primarily vasoconstrictive noradrenalin, adrenalin, and adenosine triphosphate (ATP), but some release acetylcholine, nitric oxide, and VIP. The provoked anxiety in the laboratory situation can increase the vasocongestive response of the genitalia to erotic stimulation in sexually healthy women.83 The localization of NOS, cAMP, and cGMP-degrading PDE isoenzymes in human vaginal tissue is established, along with recent identification of cAMP and cGMP-binding proteins. The latter are co-localized with endothelial NOS (eNOS). Close proximity to VIP-positive nerves suggests that cAMP and cGMP work synergistically to control vaginal blood flow.156 Neuropeptide Y (a vasoconstrictor), CGRP (possibly influencing capillary permeability and sensation), and substance P (a sensory transmitter) also innervate the vaginal microcirculation. The melanocortin-4 receptors and oxytocin also may be involved in clitoral and vaginal efferent pathways.156 Intermittency of the vaginal microcirculation due to contraction and relaxation of precapillary sphincters in response to hypoxia and the release of metabolites (PCO2, lactic acid, ATP), has been termed vasomotion. Vasomotion is present in the nonaroused state but decreases within seconds of a sexual stimulus, which increases arterial supply to thereby recruit more capillaries and diminish vasomotion: vaginal vasocongestion follows. Slow oscillations in vaginal blood flow, independent of vaginal vasocongestion, have recently been shown to correlate with subjective arousal in healthy women and to be less marked in women with arousal disorder.155 Increased blood flow to the submucosal vaginal capillaries results in increased interstitial fluid production, which diffuses more quickly across the vaginal epithelial cells and onto the lumen: the lubrication fluid in the aroused state thereby contains less potassium and more sodium than in the nonaroused state. How important the contribution of permeability of the epithelial cells is to the process of lubrication is currently unclear. Relaxation of the vaginal wall smooth muscle that enables the vagina to move up into the pelvis is likely mediated by VIP.155 The clitoris is the most sexually sensitive area of the body. Immunohistologic studies have identified neurotransmitters thought to be associated with sensation (substance P and CGRP) that are concentrated immediately under the epithelium of the glans clitoris. Nerve terminals in the glans clitoris known as corpuscular receptors are thought to be involved. They are mechanoreceptors, and their density is variable but can be up to 14 times greater than the density of similar receptors on the glans penis.157 The physiology of nongenital physical changes and their correlation with subjective excitement remain poorly understood. PHYSIOLOGY OF ORGASM Orgasm is a brain event, triggered typically by genital stimulation but also by sleep, stimulation of other parts of the body (including breast and nipple), fantasy, certain medications, and in women with spinal cord injury, vibrostimulation of the cervix. Qualitative differences in orgasm, depending on type of stimulation, are reported by some women. Pilot echographic study suggests that vaginal stimulation involves all of the clitoral-urethral complex including the clitoral rami, whereas with clitoral stimulation (i.e., to the shaft and glans), anatomic/circulatory involvement of the clitoral rami is not involved.151 Men report diminished orgasm intensity subsequent to loss of ejaculation from radical prostatectomy. Orgasm is a subjective experience in both men and women, and it has been difficult to determine an objective marker. In healthy men, there is the associated ejaculation and, in both genders, involuntary (reflexive) muscular contractions of the striated perineal muscles.158 One objective and quantitative measure has been established that shows strong correspondence with the subjective experience of orgasm. The researchers performed spectral analysis of rectal pressure data while volunteers imitated orgasm, or tried to achieve orgasm and failed, or experienced orgasm.158 The most significant and important difference in spectral power between orgasm in both control tasks was found in the alpha band. Outbursts of alpha fluctuations in rectal pressure occurred only during orgasm.158 Positron emission tomography (PET) studies during orgasm have shown largely similar brain activations and deactivations in both men and women: activations mainly in the anterior lobe of the cerebellar vermis and deep cerebellar nuclei and deactivations in the left ventromedial and OFC. The only major difference between the genders during orgasm itself was the activation in the periaqueductal gray matter in men.159,160 The lateral OFC is thought to be involved in urge suppression and behavioral release, whereas the medial parts encode hedonic experiences, becoming activated with increasing satiation and subjective pleasantness and deactivated with feelings of satiety. The medial OFC is part of the neuronal network that includes the amygdala, whose deactivation during orgasm is associated with a more carefree state of mind.159 More recent PET scanning of the brain during orgasm with comparisons to failed attempts to reach orgasm, and also comparisons to faking an orgasm, has been reported.160 Insertion of a rectal probe measured involuntary pelvic muscle contractions to identify the occurrence and duration of orgasm. The variations in rectal pressure indicative of orgasm correlated to widespread blood flow changes in the prefrontal cortex.160,161 The researchers noted specific orgasm-related changes in the mid/anterior OFC and suggest that this fits with the proposed role of the midanterior OFC in the experience of pleasure. Failed orgasm significantly enhanced left lateral OFC activity: orgasm was not reached possibly due to excessive behavioral suppression. The researchers suggest that the orgasm-related OFC dynamics may reflect one of the main features of orgasm (i.e., the typical sense of loss of control). Prefrontal but not temporal perfusion was inversely coupled to rectal pressure fluctuations associated with orgasm. These changes in the CHAPTER 20 Sexual Dysfunction in Men and Women OFC (the dorsal and ventral prefrontal divisions) did not show any clear association with arousal but only with these indicators of orgasm. The researchers therefore concluded that the decreased prefrontal cortex activity may be specific to orgasm. Overall the findings of reduced prefrontal metabolism during orgasm are in keeping with the critical role of the prefrontal cortex in behavioral and emotional control. It may be that successful prefrontal regulation is key to reaching orgasm in keeping with experimental data of exaggerated prefrontal activity with associated sexual dysfunction. Pontine control of female orgasm appears to center on a localized region on the left side of the dorsolateral pontine tegmentum recently termed the pelvic organ–stimulating center.161 Another pontine area, the ventrolateral pontine area, recently termed the pelvic floor–stimulating center, is involved in organizing the pelvic floor–contractions during orgasm and has direct projections to pelvic floor motor neurons. The role of oxytocin and prolactin in orgasm is unclear. Both hormone levels increase at the time of orgasm: PET scanning has confirmed increased pituitary blood flow in women, but not in men, at the moment of orgasm.162 Both hormones can cause uterine and vaginal smooth muscle contraction, which may contribute to the sensations of orgasm. THE REVISED DEFINITIONS OF SEXUAL DYSFUNCTION IN MEN In May 2013, the DSM-5 provided an updated classification and definitions of male sexual disorders.14 The salient differences of the new DSM-5 classification and definitions from the DSM-IV are the following15: 1. DSM-5 includes only four male sexual disorders, as opposed to six in the DSM-IV.15 The four sexual disorders are the following: a. Male hypoactive sexual desire disorder b. ED c. Premature ejaculation d. Delayed ejaculation 2. DSM-5 lists male HSDD as a separate entry.14,15 Male orgasmic disorder has been renamed delayed ejaculation, male ED has been changed to ED, and male orgasmic disorder has been changed to delayed ejaculation. Premature ejaculation remains unchanged. 3. Male dyspareunia, male sexual pain, sexual aversion disorder, and sexual dysfunction have been removed in the DSM-5.14,15 4. Unlike DSM-IV, the DSM-5 includes the requirement of experiencing the disorder 75% to 100% of the time to make a diagnosis of sexual disorder. DSM-5 also requires a minimum duration of approximately 6 months.14,15 5. DSM-5 requires that the sexual disorder must have caused significant distress. The DSM-IV requirement of “interpersonal difficulty” has been removed.14,15 6. DSM-5 added one new exclusion criterion: the disorder should not be better explained by a “nonsexual mental disorder or a consequence of severe relationship distress or other significant stressors.”14,15 Male Hypoactive Sexual Desire Disorder HSDD is the persistent or recurrent deficiency (or absence) of sexual fantasies and desire for sexual activity that causes marked distress and that is not better explained by another 797 disorder, direct physiologic effects of a substance (medication), or general medical condition.163-166 A diagnosis of HSDD is appropriate only if the person reports distress due to low sexual desire.163-166 Low sexual desire is not necessarily pathologic, as low sexual desire may be an appropriate adaptation to relationship and health-related issues.163-166 HSDD is a multifactorial disorder that can result from androgen deficiency, use of medications (SSRIs, antiandrogens, gonadotropin-releasing hormone [GnRH] analogues, antihypertensives, cancer chemotherapeutic agents, anticonvulsants), systemic illness, depression and other psychological problems, other causes of sexual dysfunction, or relationship and differentiation problems. Androgen deficiency is an important, treatable cause of HSDD and should be excluded by measuring serum total testosterone levels.163-166 The incidence and prevalence of HSDD in the general population are unknown. In studies of referred patient populations, the prevalence has been estimated at 5% in men and 22% in women.5-7,165-167 Prevalence increases with age.165-167 HSDD often coexists with other sexual disorders, such as ED, and may develop as a consequence of other preexisting sexual disorders.165-167 Appropriate evaluation and treatment of HSDD are important because evaluation may lead to detection of treatable androgen deficiency. Also, hypoactive sexual desire in one partner can strain the relationship between sexual partners168 and lead to ED. Low sexual desire may impede or reduce effectiveness of treatments for other sexual dysfunctions. Erectile Disorder ED, previously referred to as impotence or male ED, is the inability to attain or maintain an erection or to achieve penile rigidity sufficient for satisfactory sexual intercourse.10,11,14,15 DSM-5 requires that the inability to attain or maintain an erection should occur in 75% to 100% of encounters over a period of at least 6 months.14,15 Sexual dysfunction is a more general term that also includes libidinal, orgasmic, and ejaculatory dysfunction, in addition to the inability to attain or maintain penile erection. The epidemiologic surveys,4-6,167-175 including the MMAS4 and the NHSLS,5,6 revealed a surprisingly high prevalence of ED in men (see later). ED significantly affects quality of life of both the affected individual and his partner. In one study, ED had a negative impact on the sexual life of female partners, specifically on their sexual satisfaction and sexual drive.168 Prevalence and Incidence The best data on the prevalence of ED in men have emerged from two cross-sectional studies that have used population-based sampling techniques, namely the MMAS4,169,172,173 and the NHSLS.6,7 The MMAS is a crosssectional as well as longitudinal, community-based epidemiologic survey in which 1709 men, 40 to 70 years of age, residing in the greater Boston area, were surveyed between 1987 and 1989.4 This survey revealed that 52% of men between the ages of 40 and 70 were affected by ED of some degree; 17.2% of surveyed men reported minimal ED, 25.2% moderate ED, and 9.6% complete ED.4,172,173 The NHSLS was a national probability survey of Englishspeaking Americans, 18 to 59 years of age, living in the United States.6,7 This survey also revealed a high prevalence of ED in men; the prevalence of ED increased with increasing age.6,7 798 SECTION V Reproduction These two landmark studies and data from several other studies are in agreement that ED is a common problem worldwide.4,6,7,167-174 In the U.S. civilian population, the prevalence of ED in men aged 20 to 39 years has been estimated to be 5.1%, whereas prevalence in men aged 40 to 59 years was almost three times as high (14.8%). In the MMAS, crude incidence of ED was reported at 25.9 cases per 1000 person-years, although that study included only men over the age of 40. ED has been estimated to affect 20 million to 30 million men in the United States alone and 150 million to 200 million men worldwide.172,173 The prevalence of ED increases with age; it affects fewer than 10% of men younger than 45 years of age but 75% of men over 80 years of age.4 Men suffering from other medical problems, such as hypertension, diabetes, cardiovascular disease (CVD), and end-stage renal disease, have a significantly higher prevalence of ED than healthy men.4 There is a paucity of longitudinal data on the incidence rates of ED in men. In the MMAS, the crude incidence rate of ED in white men in the Boston area was found to be 25.9 cases per 1000 person-years.169 The incidence rates increased from 12.4 cases per 1000 person-years for men 40 to 49 years of age to 29.8 cases per 1000 person-years for men 50 to 59 years of age and 46.4 per 1000 person-years for men 60 to 69 years of age.169 In another study, incidence rates were derived from a survey of men seen at a preventive medicine clinic.7 This study found the incidence rates of ED to be less than 3 cases per 1000 person-years among men less than 45 years of age and 52 cases per 1000 person-years among men 65 years of age or older. These studies suggest that there were 152 million cases of ED in the world in 1995 and that 600,000 to 700,000 men in the United States develop ED each year.172,173 Risk Factors for Erectile Disorder The risk factors for ED include age, diabetes mellitus, hypertension, smoking, medication use, depression, dyslipidemia, and CVD.4,9-11,175-185 Advancing age is an important risk factor for ED in men4,6,9-11: less than 10% of men below the age of 40 and over 50% of men over the age of 70 have ED. In both the MMAS and the NHSLS, the prevalence of ED increased with each decade of life.4,6 Among the chronic diseases associated with ED, diabetes mellitus is the most important risk factor. In the MMAS, the age-adjusted risk of complete ED was three times higher in men with history of treated diabetes mellitus than in those without a history of diabetes mellitus.4,175 Fifty percent of men with diabetes mellitus will experience ED sometime during the course of their illness. In the MMAS, treated heart disease, treated hypertension, and hyperlipidemia were associated with a significantly increased risk of ED. Among men with treated heart disease and hypertension, the probability of ED was more than two times greater for smokers than for nonsmokers.4-6,9-11 Smoking also increases the risk of ED in men taking medications for CVDs. Cardiovascular disorders, including hypertension, stroke, coronary artery disease, and peripheral vascular disease, are all associated with increased risk of ED. Physical activity is associated with reduced risk of ED.184 Several reviews have emphasized the relationship of prescription medications and the occurrence of ED. In the MMAS, the use of antihypertensives, cardiac medication, and oral hypoglycemic drugs was associated with an increased risk of ED.4 Thiazide diuretics and psychotropic drugs used in the treatment of depression may be the most common drugs associated with ED, simply because of the high prevalence of their use. However, a variety of drugs, including almost all antihypertensives, digoxin, histamine-2 receptor antagonists, anticholinergics, cytotoxic agents, and androgen antagonists, have been implicated in the pathophysiology of ED.4 Erectile Disorder as a Marker of Cardiovascular Disease CVD and ED share common risk factors, such as diabetes mellitus, obesity, hypertension, smoking, and dyslipidemia.176-184 ED precedes the symptoms of coronary artery disease by 2 to 3 years and cardiovascular events such as myocardial infarction or stroke by 3 to 5 years.176-184 ED in men is associated with increased risk of death, particularly fatality due to CVD.178 The presence of ED is a good predictor of subsequent coronary artery disease, especially in younger men, independent of traditional coronary risk factors, although it does not enhance the predictive ability of models that include traditional risk factors, likely reflecting the common pathophysiologic mechanisms of ED and coronary artery disease.179 Men reporting ED are 1.3 to 1.6 times more likely to experience a cardiovascular event within 10 years than men without ED.176-184 Lower Urinary Tract Symptoms and Erectile Disorder Recent surveys have revealed an association of lower urinary tract symptoms (LUTS) with ED185-191 even after adjusting for age and other risk factors. The Cologne Male Study and the Multinational Study of Aging Male revealed that the presence and severity of LUTS is an independent predictor of ED independent of age.186 LUTS and age are stronger predictors of ED than all other risk factors, including diabetes, dyslipidemia, and hypertension. As LUTS and ED are two common conditions in middle-aged and older men, it is possible that this association reflects the coexistence of two highly prevalent conditions. However, there is growing evidence that the two conditions may be mechanistically linked, as the biochemical mechanisms that regulate bladder detrusor and cavernosal smooth muscle function share many similarities.191,192 K+ channels, especially calcium-sensitive K+ channels (BKCa channels), Rho A/Rho kinase signaling, L-type calcium channels, and gap junctions are important mediators of both detrusor and cavernosal smooth muscle contractility and relaxation.191,192 Increased myocyte contractility that characterizes both bladder detrusor dysfunction and ED may be mechanistically related to increased Rho kinase activity, impairments of K+ channel function,192 α-adrenergic receptor imbalance, and endothelial dysfunction. Additional proposed hypotheses include increased sympathetic activity and autonomic dysfunction, and alterations in nitric oxide generation or protein kinase G activity in the detrusor and cavernosal smooth muscles.191-193 Some therapies for LUTS such as some types of surgeries and 5α-reductase inhibitors may worsen sexual dysfunction. PDE5 inhibitors are being investigated for the treatment of LUTS.192-195 Ejaculatory Disorders Ejaculatory disorders include premature ejaculation, delayed ejaculation, retrograde ejaculation, anejaculation, and painful ejaculation.113-116 Recent surveys have highlighted the high prevalence and clinical importance of ejaculatory disorders.18,113-116,196,197 Although the availability of oral PDE5 inhibitors has increased awareness of ED, ejaculatory disorders are at least as prevalent and may be even more prevalent than ED.18,197 Premature ejaculation, defined as ejaculation associated with lack of or poor ejaculatory control that causes distress in one or both partners, CHAPTER 20 Sexual Dysfunction in Men and Women is the most prevalent sexual disorder in men 18 to 59 years of age.6,18,197,198 The new DSM-5 definition has now added a time requirement that the ejaculation must occur within approximately 1 minute following vaginal penetration to be deemed premature.14,15 Delayed ejaculation refers to a man’s inability to ejaculate in a reasonable period that interferes with sexual or emotional satisfaction and is associated with distress. Retrograde ejaculation is the failure of the semen to be ejected out through the urethral meatus; instead the semen is propelled backward into the urinary bladder.113-116 Retrograde ejaculation can be the result of autonomic neuropathy associated with diabetes mellitus; sympathectomy; therapy with adrenergic antagonists, some types of antihypertensives, antipsychotics, or antidepressants; bladder neck incompetence; or urethral obstruction. Retrograde ejaculation due to diabetes-associated autonomic neuropathy is the second most prevalent ejaculatory disorder.113-116 Following transurethral resection of the prostate, the bladder neck closure mechanism may be damaged. Patients remain continent because of a second, more distal, continence mechanism that is present in the region of the membranous urethra; however, many patients who have undergone transurethral resection of the prostate experience retrograde ejaculation. Ejaculatory disorders can lead to infertility among men.113-116 CURRENT DEFINITIONS OF SEXUAL DISORDERS IN WOMEN The currently recommended definitions for female sexual disorders in the DSM-5 are shown in Table 20-1.14,15 A disorder is diagnosed only if there is clinically significant distress or impairment. Disorders are identified as early onset (lifelong) versus late onset (acquired). The sexual dysfunction should not be more attributable to a nonsexual psychiatric disorder, to the effects of a substance (e.g., a drug of abuse, a medication), to a medical condition, or to relationship distress, partner violence, or other significant stressors.14,15 Sexual Interest/Arousal Disorder The definition addressing problematic desire merges sexual interest (motivation) with arousal and focuses away from initial/anticipatory desire.199,200 Increasing evidence suggests that desire ahead of and at the outset of sexual engagement, although welcomed probably by both partners, is not mandatory for a woman’s sexual enjoyment and satisfaction.25,27,28,201 It is the inability to trigger desire and arousal during sexual engagement (as well as an absence of desire initially) that constitutes disorder. Empirical support for the concept that arousal may precede desire and the two then coexist is now strong and includes data from older and younger women.26-28 Therefore, merging of sexual and desire difficulties into one disorder appears logical. However, validated questionnaires used to assess sexual function are based on models of sexual response in which desire is assumed necessary at the outset of engagement. This is now acknowledged as a serious limitation to research,202 and the prevalence of what is currently understood to be disorder is quite unclear.40,201-209 Studies that simply report “low desire and distress” indicate prevalence rates of about 10%, not increasing with age.40,207 Risk factors include negative feelings for the partner and mood disorders.204 Depression, either currently or in the past, and, in the absence of any diagnosed 799 depression, more depressive and anxious thoughts and low self-esteem are found significantly more commonly than in control women.40,207 Female Orgasmic Disorder The prevalence of women’s orgasmic disorder is also unclear, because many studies include women with low arousal who rarely reach orgasm.20,40,207 Risk factors include anxiety about the partner’s presence, fear of being vulnerable, fear of not being in control, and fear of intimacy.20 These factors often stem from childhood (nonsexual) experiences. Genitopelvic Pain/Penetration Disorder The merging of former terms vaginismus and dyspareunia has some merit. Some women report typical phobic avoidance of penetration such that a penile introital contact has never been possible, and physical examination has to be deferred until therapy enables a careful inspection and ultimately a complete pelvic examination to be done. When abnormalities other than the reflex muscle tightening are absent, then vaginismus was diagnosed. However, often the condition is complicated. For example, the woman gives a history of phobic avoidance and fear, and subsequent examination confirms vaginistic reaction, but once therapy allows a careful detailed introital examination, allodynia of the vestibule is confirmed. The diagnosis then, prior to DSM-5, was vaginismus by history but provoked vestibulodynia (PVD) on examination. Reported prevalence of sexual pain varies between 20% and 35%.210-214 The most common form of pain with penetration, PVD, affects some 16% of mostly premenopausal women, many of whom have had pain consistently from first attempts at penetration.205 Risk factors for PVD include some personality traits—perfectionism, reward dependency, fear of negative evaluation—as well as harm avoidance, hypervigilance for pain, higher levels of trait anxiety, and shyness.205 For a small subset, vaginal candidiasis appears to precipitate and maintain the condition. Vaginismus is now included within genitopelvic pain/ penetration disorder.14 The term had described (phobic) avoidance, involuntary pelvic muscle contraction, and anticipation of, fear of, or the experience of pain—there being no structural or other abnormalities on examination, this having to be deferred until some therapy has begun. Risk factors include depression, anxiety, social phobia, somatization, and hostility. Some studies identify increased catastrophic thinking in women with vaginismus compared with women without pain or women with other forms of pain: moreover, women with vaginismus show greater disgust propensity.205 Despite the theories, there is no scientific evidence that vaginismus is secondary to religious orthodoxy, negative sexual upbringing, or concerns about sexual orientation. Typically there is extreme fear of vaginal entry, fear that harm will come from something the size of a penis entering the vagina, and fear of damage by vaginal delivery. Persistent Genital Arousal Disorder Not included in the DSM-5, but clinically an increasingly common and poorly understood entity, is persistent genital arousal disorder: spontaneous, intrusive, and unwanted genital arousal (e.g., tingling, throbbing, pulsating) in the absence of sexual interest and desire. Any awareness of subjective arousal is typically, but not invariably, unpleasant. The arousal is unrelieved by one or more orgasms, and 800 SECTION V Reproduction the feelings of arousal persist for hours or days.206 Prevalence is unknown and a broad range of symptoms is recognized, from mild (and perhaps pleasant) to intrusive, highly distressing, and markedly interfering with life. SEXUAL DYSFUNCTION IN THE CONTEXT OF ENDOCRINE DISEASE We will focus on sexual sequelae of endocrine disease and its treatment, but in any given person nonendocrine factors may be more important. These factors include psychological, relational, contextual, cultural, and nonendocrine medical influences—especially depression, hypertension, neurologic disease, and LUTS.20 For patients with chronic disease, the disease itself, its treatment, its psychological effects, plus interpersonal, personal, and contextual issues affect sexual response.20 In healthy women, factors such as attitudes toward sex, feelings for the partner, past sexual experiences, duration of relationship, and mental and emotional health have been shown to more strongly modulate desire and arousability than do biologic factors.20 Contrary to gender stereotypes, recent analysis of the 1035 sexually active adults who participated in the NHSLS in 1992 showed that men’s physical sexual pleasure was more closely linked to relational factors than was the case for women.6,40,168 Similarly, in a recent international study of midlife and older couples, men rated the importance of sex for closeness and intimacy to their partner more highly than did their female partners.40 Qualitative research also suggests that men as well as women note that positive self-esteem and feeling attractive enhance desire and arousal.40,168 Sexual context is also important for both men and women.168 Endocrine Disorders and Sexual Dysfunction in Men Androgen Deficiency Syndromes Androgen deficiency in men is a syndrome characterized by a constellation of signs and symptoms associated with consistently low testosterone levels due to disorders of the testes, pituitary, or the hypothalamus.1,62 Androgen deficiency can occur either because of primary testicular dysfunction or as a result of disorders affecting the hypothalamus or the pituitary.62 Common causes of primary testicular dysfunction include Klinefelter syndrome, uncorrected cryptorchidism, human immunodeficiency virus (HIV) infection, orchitis, trauma, torsion, and radiation and cancer chemotherapy.62 Secondary testicular dysfunction can result from systemic illness; excessive exercise; recreational drugs, especially opiates, marijuana, cocaine, and alcohol; pituitary and suprasellar tumors; hemochromatosis; hyperprolactinemia; and infiltrative disorders. Exclusion of these secondary causes of hypogonadism may then justify a diagnosis of idiopathic hypogonadotropic hypogonadism, which is a heterogeneous group of disorders characterized by disordered GnRH secretion.62 The testosterone levels required to maintain sexual function are close to the lower limit of the normal male range.64,135,140,215-217 Therefore, some men with pituitary tumors may remain asymptomatic until their tumor has grown substantially and testosterone levels have declined to a level below this threshold. Androgen deficiency is an important treatable cause of male HSDD. Therefore, the men diagnosed with HSDD should be evaluated for androgen deficiency by measurement of testosterone levels using a reliable assay, preferably in an early morning fasting blood sample.62 Although ED and androgen deficiency in men are distinct disorders with separate pathophysiologic mechanisms, the two can coexist in the same patient. Testosterone levels should be measured in men presenting with any form of sexual dysfunction because androgen deficiency is treatable, and furthermore, androgen deficiency may be a manifestation of another underlying disease, such as a pituitary tumor, which may require additional evaluation and diseasespecific intervention. Diabetes and Sexual Dysfunction in Men Men with diabetes mellitus are at increased risk of ED, retrograde ejaculation, and low testosterone levels. Peyronie disease is an important comorbid condition in older diabetic men with ED.218-225 The men with diabetes have significantly lower scores for sexual desire, activity, arousal, and satisfaction,219-225 in part due to the medical and psychological factors associated with diabetes, such as the variations in glycemic control, reduced energy, altered selfimage, and interpersonal difficulties regarding dietary compliance, glucose monitoring, and medications. Diabetes also is associated with increased risk of low testosterone levels.62,226-231 In population studies, sex hormone–binding globulin (SHBG) and total testosterone are more strongly associated with diabetes risk than free testosterone levels; these data suggest that the observed association of testosterone with diabetes risk may be related to factors, such as insulin sensitivity and inflammation, that regulate SHBG.230,231 The prevalence of ED in men with diabetes increases with age and has been as high as 75% in some studies. ED in men with type 2 diabetes even without other risk factors for coronary artery disease may signal silent cardiac ischemia.231-235 Among men with diabetes, those with ED are more likely to be older smokers with longer duration of diabetes, poor metabolic control, untreated hypertension, and presence of neuropathy, microalbuminuria and macroalbuminuria, retinopathy, CVD, diuretic treatment, low testosterone levels, and psychological vulnerability.221-224 Increased physical activity and consumption of small amounts of alcohol have been found to be protective. The risk of ED generally increases with chronic elevation of hemoglobin A1c.221 Endothelial and smooth muscle dysfunction, autonomic neuropathy, and psychological and interpersonal issues contribute to sexual dysfunction in men with diabetes.234,235 Endothelial dysfunction is evident in penile blood vessels as well as in nongenital vascular beds.189 eNOS is reduced, possibly due to overexpression of arginase or lack of nicotinamide adenine dinucleotide phosphate (NADPH), an essential cofactor for NOS.235-240 Additionally, accumulation of oxygen free radicals, including those from advanced glycosylation end products (AGEs), quench nitric oxide and attenuate the action of K+ channels.239,240 The reduction in NADPH is also associated with increased diacylglycerol and protein kinase C, and consequently, increased smooth muscle contractility.237 An increased activation of the Rho A/Rho kinase pathway may increase the sensitivity of cavernosal smooth muscle to calcium.237 Autonomic neuropathy affecting the pelvic nerves may lead to ED as well as ejaculatory dysfunction.238 Retrograde ejaculation and partial ejaculatory incompetence affect up to one third of men with diabetes.241 Autonomic nerve damage in diabetes may be associated with dysfunction of the internal sphincter so that all or a part of the seminal fluid is propelled into the bladder.238 Partial ejaculatory incompetence refers to the condition in which CHAPTER 20 Sexual Dysfunction in Men and Women ejaculatory emission remains intact but the expulsion phase is inhibited; consequently, the semen trickles out of the penis and the experience of orgasm is altered in quality. Both ejaculatory problems may be a cause of infertility. Sexual Dysfunction Associated With Therapies for Benign Prostatic Hypertrophy Benign prostatic hypertrophy is frequently associated with LUTS and sexual dysfunction.185-191 Although treatment with some α1-adrenergic receptor blockers can improve erectile function, others, such as tamsulosin, are associated with ejaculatory dysfunction.242,243 Treatment of men with LUTS with 5α-reductase inhibitors has been associated with increased risk of ejaculatory disorder, ED, and decreased libido.244,245 Several surveys have reported the development of sexual symptoms, including loss of libido, ED, and difficulty with ejaculation in a subset of young men who have taken finasteride for alopecia246-249; these symptoms have been reported to persist even after discontinuation of finasteride. Although the causative role of finasteride and the pathophysiology of these symptoms remain to be established, it has been speculated that polymorphisms in androgen receptor or other genes may render these individuals susceptible to off-target actions of finasteride.250 Hyperprolactinemia and Sexual Dysfunction Hyperprolactinemic men often present with decreased libido or ED; 75% of men with macroprolactinomas and 50% of men with microprolactinomas report reduced desire or ED and almost all have subnormal nocturnal penile erections.251-255 Hyperprolactinemia affects 1% to 5% of men presenting with ED252; a fraction of these men have prolactin-secreting pituitary adenomas. Prolactin lowers testosterone levels through its inhibitory effects on GnRH secretion and on the pituitary response to GnRH. Most, but not all, men with sexual dysfunction and hyperprolactinemia have low testosterone levels.251,252 Whether and how hyperprolactinemia directly affects erectile function through target organ effects is not well understood. Erectile function generally improves in hyperprolactinemic men following treatment with dopamine agonists.254,255 Sexual Dysfunction in Patients With Thyroid Disease Hypothyroidism has been associated with increased risk of hypoactive sexual desire and ED.256-260 The exact prevalence of sexual dysfunction in men with hypothyroidism is unknown. Free testosterone levels are lower in hypothyroid men than in control subjects and become normal after thyroxine replacement.256-260 Serum LH and folliclestimulating hormone levels are typically not elevated in men with primary hypothyroidism.259 Hyperprolactinemia is noted in a small fraction of hypothyroid men.259 Free testosterone levels are typically normal in men with hyperthyrodism, but SHBG and estradiol levels are elevated, resulting in a high estradiol-to-testosterone ratio and gynecomastia in some hyperthyroid men.258 Hyperthyroidism has been observed in a small fraction of men with ED.260 Sexual Dysfunction in Men With Metabolic Syndrome The men with metabolic syndrome have a higher prevalence of ED than men without the metabolic syndrome.261-264 The risk of ED is correlated with the number of identified components of metabolic syndrome.260-264 801 Endocrine Disorders and Sexual Dysfunction in Women Thyroid Disease in Women Both hyper- and hypothyroid states have been found to be risk factors for sexual dysfunction, which mostly remits with return to an euthyroid state.265-267 Studies are few and small, and when mood is also assessed, comorbid depression is found to be associated with sexual dysfunction in the context of thyroid disease.1,265 There is some evidence that thyroid autoimmunity lessens sexual desire independent of altered thyroid status: euthyroid women with Hashimoto thyroiditis may report persistent loss of desire.265-267 One research group found women with nodular goiter to have significantly more sexual dysfunction than control subjects. This group also had the highest body mass index.267 Hyperprolactinemia in Women Hyperprolactinemia is associated with increased risk of sexual dysfunction.76,268 Women with hyperprolactinemia report greater overall dissatisfaction with sexual function and lower scores for sexual desire, arousal, lubrication, and orgasm domains than women with normal prolactin levels. Prolactin inhibits GnRH pulses, attenuates gonadotropin response to GnRH, and is associated with reduced ovarian secretion of estrogen and androgen. Although menstrual disturbance or infertility is more commonly the presenting symptom of hyperprolactinemia, lower scores for sexual function and desire have also been found in women with hyperprolactinemia who have regular menses.268 However, normal menstruation, younger age, and smaller prolactinoma size are more likely to be associated with normal sexual function than the actual level of prolactin or testosterone.20 Sexual outcomes of treatment of hyperprolactinemic women with dopamine agonists have not been well studied. Diabetes in Women Women’s sexual response and satisfaction may be compromised by diabetes-associated changes in their well-being, mood, and self-image, especially if there is unwanted weight gain, recurrent vaginitis from candidiasis, or imposed infertility.269-282 In addition, there may be a com­ promised neurovascular genital sexual response from autonomic neuropathy or endothelial dysfunction and microvascular disease. In women with type 1 diabetes, sexual dysfunction is mostly correlated to psychological factors including depression, anxiety, and marital status.270,271,273,281 The results from a large prospective study of 625 women with type 1 diabetes confirmed depression as the major predictor of dysfunction.277 Most studies on women with type 2 diabetes are small, but one larger study of 600 women with type 2 diabetes confirmed only depression and marital status to be independent risk factors for sexual dysfunction.269 Although sexual dysfunction has been associated with both type 120,270,274,277 and type 220,271-273,276,278 diabetes, not all studies confirm an association.273,275,279 A recent meta-analysis280 that included 26 studies, 3168 women with diabetes, and 2823 control subjects confirmed sexual dysfunction to be more frequent in women with diabetes. Compared to women without diabetes, the risk of sexual dysfunction was 2.27 and 2.49 times higher in women with type 1 and type 2 diabetes, respectively.280 The risk for sexual dysfunction was nearly two times higher for women with any form of diabetes. However, 802 SECTION V Reproduction postmenopausal women with any form of diabetes did not demonstrate an increased risk of sexual dysfunction. The increased prevalence of sexual dysfunction and lower female sexual function index (FSFI) score in women with diabetes may be related to body weight. This association would be in keeping with other studies showing an increased prevalence of sexual dysfunction in obese women281-283 and in women with metabolic syndrome.284,285 Unlike the situation in men with diabetes, sexual dysfunction has not been consistently associated with the presence of diabetic complications in the majority of studies. Type 1 diabetes may be associated with loss of genital sexual sensitivity.286 Sexual dysfunction in women with diabetes is complex, and the roles of body mass index, fat distribution, diabetic complications, insulin resistance, inflammation, CVD, relationship satisfaction, and depression remain poorly understood.20,282,283 Pathogenesis of Sexual Dysfunction in Diabetes. Whereas depression and obesity are the identified major etiologic factors, in the individual woman, neurovascular complications of diabetes may be relevant.20,287,288 Autonomic and somatic neuropathy may contribute to loss of genital sexual sensitivity. When there is less engorgement of the vascular sinusoidal tissue comprising the shaft, head, rami, and bulbs of the clitoris, massaging the structures during sexual stimulation will fail to elicit typical sexual sensations to compromise arousal and limit the experience of orgasm.287,288 In animal studies, diabetes has been shown to impair vaginal smooth muscle relaxation responses to the neurotransmitters, particularly VIP and nitric oxide.287 These studies also report decreased clitoral and vaginal blood flow to nerve stimulation, diffuse fibrosis of the clitoral and vaginal tissues, as well as reduced muscular layer and epithelial thickness in vaginal tissue. Endothelial dysfunction and reduced clitoral blood flow have been documented in women with diabetes.288 Most studies have not found increased prevalence of dyspareunia in women with diabetes. Diabetic women are at higher risk of recurrent candidiasis, which may contribute to dyspareunia.289 Metabolic Syndrome in Women Metabolic syndrome has been shown to have a deleterious effect on women’s sexuality, independent of diabetes and obesity.1,20,289,290 This negative effect seems to be more prevalent in premenopausal than postmenopausal women.1,20,289,290 Polycystic Ovary Syndrome Limited research has shown that women with polycystic ovary syndrome may be less sexually satisfied and may regard themselves as less attractive than control subjects.291-294 The presumption is that obesity and androgenrelated symptoms may contribute to poor body image, which may increase the risk of sexual dysfunction.1,282 Recent studies show little evidence that polycystic ovary syndrome (as opposed to obesity) is a risk factor for sexual dysfunction.294,295 Congenital Adrenal Hyperplasia Nonclassic forms of congenital adrenal hyperplasia may present with signs of hyperandrogenism in childhood or adulthood, depending on the severity of the 21-hydroxylase enzyme deficiency.296 The presenting features of 21hydroxylase enzyme deficiency may include menstrual disorders such as amenorrhea, anovulation, hirsutism, or oligomenorrhea with infertility.297 Limited research suggests that sexual functioning of women with nonclassic 21-hydroxylase deficiency is not different from that of control subjects. However, women with classic congenital adrenal hyperplasia may show gender-atypical behavior298; in one study, male-typical role-playing in childhood correlated with reduced satisfaction with the female gender role and reduced heterosexual interest in adulthood.299 Disturbed body image, repeated genital examinations, and genital surgery may also affect sexual function in women with congenital adrenal hyperplasia.298 Caring for these women requires careful individualized treatment with appropriate therapy for signs and symptoms of androgen excess as well as psychosexual counseling.20 Pituitary Disease in Women There is limited research on sexual function in women who have deficiencies of various pituitary hormones. It is known that most women with pituitary disease often report menstrual irregularity or problems with sexual function, including decreased sexual desire and problems with lubrication or orgasm.76 Although women with hypopituitarism have lower testosterone levels than healthy menstruating women, the short- and long-term effects of testosterone in women with hypopituitarism have not been well studied.300,301 In one randomized trial of 51 women, testosterone therapy in women who were receiving estrogen therapy was associated with some benefit in sexual function and mood, compared with placebo, but with a higher frequency of androgenic side effects than placebo.302 The effects of dehydroepiandrosterone (DHEA) on sexual function and mood in women with hypopituitarism are also poorly understood.301 Adrenal Insufficiency in Women In addition to the deficiency of cortisol and aldosterone, women with adrenal insufficiency also have low levels of testosterone and DHEA.1,303-312 Adrenal insufficiency in women has been associated with low health-related quality of life.308 However, a 2010 larger study comparing 174 women with Addison disease to 740 age-matched healthy control subjects and to 234 women who had received a risk-reducing bilateral salpingo-oophorectomy (BSO) demonstrated that despite subnormal levels of androgens and androgen metabolites, the women with Addison disease reported higher sexual pleasure and less discomfort with intercourse than the normative control women.309 Clinical trials of DHEA replacement in women with adrenal insufficiency have been small and mostly negative.1,303-307,310,312 An earlier small trial in women with primary or secondary adrenal insufficiency reported greater improvements in sexual interest and satisfaction and in mood for women receiving DHEA compared with placebo303; however, four subsequent studies did not find significant improvements in sexual function.304-307 In 2009, a meta-analysis of 10 studies concluded that DHEA therapy in adrenal insufficiency may result in small improvements in health-related quality of life and depression, but it had no effects on anxiety or sexual well-being.312 Thus, there are insufficient data to support the routine use of DHEA in women with adrenal insufficiency. Natural Menopause A majority of women who discontinue postmenopausal estrogen supplementation develop signs of vulvovaginal CHAPTER 20 Sexual Dysfunction in Men and Women atrophy, which is a risk factor for sexual dysfunction.210-214,313,314 However, symptoms from vulvovaginal atrophy may remit spontaneously within 1 year; risk factors for more severe symptoms are diabetes, younger age, and low body mass index.214,313,314 The traditional notion that maintaining sexual activity will prevent symptomatic vulvovaginal atrophy has been refuted.314 Subjective symptoms and objective signs of vulvovaginal atrophy correlate poorly.315 Epidemiologic studies have not shown an increase in the prevalence of dyspareunia with age.210-212 Clearly not all postmenopausal women develop sexual symptoms of estrogen deficiency: of 1525 women followed from age 47 to 54 years, the vast majority were not affected by the major hormonal shifts.213 It is likely that multiple factors contribute to sexual symptoms, including variations in the intracrine production of estrogen from adrenal precursors, the number and sensitivity of estrogen receptors, and the degree of sexual arousal or excitement at the time of vulval stimulation and vaginal entry.316-318 Psychological factors rather than estrogen levels were shown to moderate symptoms when vulvovaginal atrophy is present.318 Most studies report a decrease in sexual desire with advancing age319 that is not easily explained by hormonal deficiency alone. Adaptive changes occur in the brain in response to the reductions in circulating levels of sex hormones associated with age and menopause.320,321 Sex hormones are produced locally within the brain: in women, steroidogenic enzymes and sex-steroid receptors in the brain are upregulated in response to decreased circulating levels of sex hormones.320,321 We do not know whether there is biologic adaptation to reduced amounts of sex hormones. In studies of age, menopausal status, and sexual function, the postmenopausal state has generally been negatively associated with desire mainly among women who experienced low emotional intimacy with their partners. Similarly, the negative association between age and sexual desire was particularly pronounced in women experiencing little intimacy.322 Surgical Menopause Surgical menopause is a state of both androgen and estrogen depletion of sudden onset and has often been viewed as a risk factor for sexual dysfunction. However, most women undergoing bilateral BSO for benign clinical indications do not develop sexual dysfunction. Three pro­ spective studies found that women choosing BSO plus hysterectomy for benign indications did not develop sexual dysfunction over the next 1 to 3 years.323-325 A national survey of 2207 American women confirmed an increased prevalence of distress about low sexual desire in women with a recent BSO.319 Thus, in women undergoing nonelective surgery, the thematic context of bilateral oophorectomy may impair sexual desire and function. For example, women who are treated for malignant disease or those who desire to preserve their fertility may experience greater distress about low sexual desire after BSO than those who undergo BSO for benign conditions. In the same survey, both older and younger women with a relatively recent BSO reported low sexual desire per se, as often as age-matched subjects with intact ovaries.319 Despite their continued hormonal deficit, women older than 45 years who underwent oophorectomy before menopause had fewer complaints of low desire than women of similar age with intact ovaries.319 A recent study of 1352 women showed no difference in the report of sexual ideation, sexual function, or sexual problems between women who have had and women who have not had bilateral oophorectomy.326 Having thoughts 803 about sex is less likely to be affected by contextual details including the sexual relationship than is sexual function or motivation for partnered sex. The women who carry a BRCA mutation and undergo BSO to lessen the risk of breast, ovarian, or fallopian tube cancer mostly remain satisfied with their decision for surgery.327 However, studies on sexual response are conflicting. Less sexual pleasure despite the use of local estrogen to alleviate dyspareunia has been noted,328 whereas another study comparing 234 women who had received a riskreducing BSO to 740 age-matched control subjects from the general population demonstrated that the women with risk-reducing surgery had greater sexual pleasure and less dyspareunia than the normative control women.326,329 Aging-Associated Decline in Sex Hormone Precursors in Women From the middle 30s to the early 60s, a woman’s adrenal production of precursor hormones—DHEA, androstenedione, and DHEA sulfate (DHEAS)—declines by 70%.65,67 However, the trajectories of decline in these precursor steroids vary among women.65-67 The relationship of the age-related decline in these circulating precursors to sexual function remains poorly understood. On the population level, variation in circulating levels of sex steroids and their precursors is related to variation in the activities of ster­ oidogenic enzymes such as 3β-hydroxysteroid dehydrogenase (3β-HSD), 17β-HSD, 17,20-lyase, and aromatase and to the variation in the plasma clearance of these hormones and precursors. Labrie and associates have proposed that the androgen metabolites, most notably ADT-G, may serve as useful markers of ovarian as well as tissue production and activity of androgens in women.67,316,330 A study of 250 women carefully evaluated for sexual dysfunction found that ADT-G levels in the 124 control women were comparable to those in the 121 women with sexual dysfunction.66 Selective Estrogen Receptor Modulators Selective estrogen receptor modulators (SERMs) are a class of ligands that bind estrogen receptor subtypes and induce a unique profile of tissue-specific gene expression. Accordingly, each SERM may also be associated with a unique set of clinical responses. Ospemifene has estrogen antagonist action on breast and endometrium. Ospemifene, but not raloxifene or tamoxifen, can ameliorate the genital sexual symptoms of lack of estrogen.331 Limited research suggests raloxifene and tamoxifen are not associated with sexual adverse effects. Hormonal Contraceptives The estrogen in combined systemic contraceptives increases SHBG and thus decreases available free testosterone. The decrease in sexual desire and subjective arousability in some women receiving oral contraceptives has been attributed to the decrease in free testosterone levels. However, to date low desire has not been associated with testosterone levels, even when mass spectrometry methods are used.65,66 Hormonal contraceptives exert multiple psychological and biologic actions, some of which may positively affect sexuality, for example, by reducing anxiety about unwanted pregnancy and diminishing dysmenorrhea.332 Androgen Insensitivity Syndrome Research is very limited on sexual function in 46,XY women with androgen insensitivity syndrome due to 804 SECTION V Reproduction mutations in the androgen receptor. Women with complete androgen insensitivity syndrome have a female phenotype with full breast development but variable shallow vaginal development, which may require surgical intervention or progressive dilatation. Small cross-sectional studies indicate healthy sexual response with orgasms and experience of self-stimulation and of intercourse.328,333-336 However, these women are often confronted with complex psychosocial issues related to the mismatch between their genetic sex and their gender role, the timing of diagnosis and timing of disclosure to the woman, and infertility. Reduced sexual confidence, self-esteem, and depression are noted in these studies. ASSESSMENT OF SEXUAL DYSFUNCTION Assessment of sexual function is an important part of the general assessment of patients with endocrine diseases. Open-ended, nonjudgmental questions such as, “Many men with diabetes notice changes in their erections or ejaculation—are you having any difficulties?” can facilitate further discussion of sexual problems. When sexual problems are identified, sensitive and respectful inquiry into their nature and the current and past sexual context is necessary. Evaluating both partners together as well as individually can often uncover problems that may not be apparent in individual interviews (Table 20-4). Evaluation of Men With Sexual Dysfunction There are four important considerations in the evaluation of men with HSDDs. First, an important initial step in the evaluation is an interview of the couple to determine whether the patient primarily has ED or a sexual desire problem. Second, ascertain whether the couple has a relationship problem. Establish whether self-stimulation continues despite lack of desire for partnered sex. With the availability of Internet sites, sex alone, possibly on a frequent basis, may allow sexual expression in spite of relationship difficulties. Third, general health evaluation is necessary to exclude systemic illness, depression, and medication use. Last, testosterone levels should be measured to exclude androgen deficiency because androgen deficiency is an important treatable cause of HSDD. The diagnostic workup of men with ED should start with an evaluation of general health (Tables 20-4 and 20-5).10,11,337-342 The presence of diabetes mellitus, coronary TABLE 20-4 Assessment of a Patient With Sexual Dysfunction Assessment Questions Questions Asked of One or Both Partners Comments 1. Sexual problems and reason for presenting at this time Ask patients to describe sexual problems in their own words; clarify further with direct questions, giving options rather than leading questions, support and encouragement, acknowledgment of embarrassment, and reassurance that sexual problems are common Are problems present in all situations? Which problem is most troubling? 2. Duration, consistency, and priority if more than one problem is present 3. Context of sexual problems 4. Each partner’s sexual response in areas other than the given problem area 5. Reaction of each partner 6. Previous help Emotional intimacy between partners, activity or behavior just before sexual activity, privacy, sexual communication, time of day and fatigue level, birth control (adequacy, type), risk of STIs, usefulness of sexual stimulation, sexual knowledge Both currently and before the onset of the sexual problems How has each reacted emotionally, sexually, and behaviorally? Compliance with recommendations and effectiveness Questions Asked of Each Partner When Seen Alone* 1. Partner’s own assessment of the situation 2. Sexual response with self-stimulation 3. Past sexual experiences 4. Developmental history 5. Past or current sexual, emotional, and physical abuse 6. Physical health, especially conditions leading to debility and fatigue, difficulty with mobility (e.g., in caressing a partner, performing self-stimulation), and difficulties with self-image (e.g., from obesity, Cushing syndrome. hypogonadism) 7. Evaluation of mood Sometimes it is easier to disclose symptom severity (e.g., total lack of desire) in the partner’s absence Also inquire about sexual thoughts and fantasies Positive and negative aspects Relationships to others in the home while growing up; losses, traumas, to whom (if anyone) was the patient close; was he or she shown physical affection, love, respect? Explain that abuse questions are routine and do not necessarily imply causation of the problems; it is helpful to ask whether the patient ever felt hurt or threatened in the relationship and, if so, whether he or she wishes to give more information Specifically, ask about medications with known sexual side effects, including SSRIs, SNRIs, β-blockers, narcotics, antiandrogens, GnRH agonists A significant correlation of sexual function and mood (including anxiety and depression) warrants routine screening for mood disorder using either a questionnaire (e.g., Beck Inventory) or semistructured series of questions *Items 3 through 5 of the single-patient interview may sometimes be omitted (e.g., for a recent problem after decades of healthy sexual function). GnRH, gonadotropin-releasing hormone; SSNIs, selective serotonin norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors; STIs, sexually transmitted infections. Adapted from Basson R. Sexual dysfunction in women. N Engl J Med. 2006;354:1497-1506. Copyright ©2006 Massachusetts Medical Society. All rights reserved. CHAPTER 20 Sexual Dysfunction in Men and Women TABLE 20-5 Directed Diagnostic Evaluation of Erectile Dysfunction History Ascertain Psychosexual History The nature of sexual dysfunction: whether the primary problem is decreased desire, erectile dysfunction, premature or delayed ejaculation, or difficulty in achieving orgasms The strength of marital relationship and marital discord Depression Stress Sexual performance anxiety Knowledge and beliefs about sexuality Ascertain Risk Factors The presence of diabetes mellitus, hypertension, hyperlipidemia, coronary artery disease, end-stage renal disease, and peripheral vascular disease History of spinal cord injury, stroke, or Alzheimer disease Prostate or pelvic surgery Pelvic injury Medications such as antihypertensives, antidepressants, antipsychotics, antiandrogens, and inhibitors of androgen production The use of recreational drugs such as alcohol, cocaine, opiates, and tobacco Ascertain Factors That Might Affect Choice of Therapy and the Patient’s Response to It Coexisting coronary artery disease and its symptoms and severity Exercise tolerance The use of nitrates or nitrate donors The use of α-adrenergic blockers The use of vasodilators for hypertension or congestive heart failure The use of foods (such as cranberry juice) or drugs (such as erythromycin, protease inhibitors, ketoconazole, and itraconazole) that might affect metabolism of PDE5 inhibitors Physical Examination Ascertain signs of androgen deficiency, such as loss of secondary sex characteristics, eunuchoidal proportions, small testicular volume, or breast enlargement Genital and perineal sensation to evaluate neurologic deficit from spinal cord lesion, previous stroke, or peripheral neuropathy Blood pressure and postural change in blood pressure Evaluate femoral and pedal pulses and evidence of lower extremity ischemia Penile examination to exclude Peyronie disease or other penile deformities Basic Laboratory Evaluation That Should Be Performed in All Men With ED Fasting blood glucose Plasma lipids Serum testosterone level ED, Erectile dysfunction; PDE5, phosphodiesterase 5. artery disease, peripheral vascular disease, hypertension, stroke, spinal cord or back injury, multiple sclerosis, depression, or dementia should be verified. Information about use of recreational drugs such as alcohol, marijuana, cocaine, and tobacco; prescription medications, particularly antihypertensives, antiandrogens, antidepressants, and antipsychotic drugs; and nonprescription over-thecounter supplements is important because almost a quarter of all cases of impotence can be attributed to medications. A detailed sexual history including the nature of relationships, partner expectations, situational erectile failure, performance anxiety, and marital discord needs to be elicited. It is important to distinguish between inability to achieve erection, changes in sexual desire, failure to achieve orgasm and ejaculation, and dissatisfaction with the sexual rela- 805 tionship, as the etiologic factors vary with the type of sexual disorder. A directed physical examination should focus on secondary sex characteristics, the presence or absence of breast enlargement and testicular volume; evaluation of femoral and pedal pulses; neurologic examination to determine the presence of motor weakness, perineal sensation, anal sphincter tone, and bulbocavernosus reflex; and examination of the penis to evaluate any unusual curvature, palpable plaques, or superficial lesions.337-342 The laboratory tests in the evaluation of a man with ED usually include measurements of hemoglobin, blood glucose, blood urea nitrogen and creatinine, plasma lipid, and testosterone levels. Thus, the initial diagnostic workup in most men presenting with ED consists of general health evaluation; evaluation of cardiovascular risk by the measurements of blood glucose, plasma lipids, and blood chemistries; and measurement of serum testosterone levels. Further evaluation using more invasive diagnostic testing is limited to those men who do not respond to an empiric trial of oral PDE5 inhibitors; these patients should be referred to a specialist for detailed urologic evaluation. Self-reporting questionnaires are useful because many men with ED do not voluntarily come forward to their physicians and state their sexual complaints for a variety of reasons.337-340 The International Index of Erectile Function (IIEF), for example, is a multidimensional scale consisting of 15 questions that address relevant domains of male sexual function, including sexual desire, intercourse satisfaction, orgasmic function, and overall satisfaction337; a short form is also available.340 The diagnosis of androgen deficiency should be made only in men with consistent symptoms and signs and unequivocally low early morning serum testosterone levels that are below the lower limit of the normal range for healthy young men (e.g., testosterone <300 ng/dL in some laboratories) on at least two occasions.1,11,64 Initial eval­ uation is directed at excluding systemic illness, eating disorders, excessive exercise, and use of medicines and recreational drugs that can suppress testosterone levels. The measurement of morning total testosterone level by a reliable assay, such as liquid chromatography tandem mass spectrometry (LC-MS/MS), using rigorously derived reference ranges, remains the best initial test.343-346 The advent of LC-MS/MS, the availability of a testosterone calibrator from the National Institute of Standards and Technologies (NIST), and the institution of Hormone Standardization Program for Testosterone (HoST) has greatly improved the accuracy of testosterone assays and reduced interlaboratory variability among Centers for Disease Control and Prevention (CDC)-certified laboratories.343-346 The measurement of free testosterone levels is useful in men with suspected SHBG alteration due to genetic factors, aging, obesity, diabetes, chronic illness, thyroid and liver disease, and HIV or hepatitis B or C infection.347 Free testosterone levels should be measured using a reliable assay, such as the equilibrium dialysis assay, in a laboratory that has experience in performing this assay.64 Free testosterone concentrations can also be calculated from total testosterone and SHBG concentrations.347 However, Zakharov and colleagues348 have shown that the published linear law of mass action equations based on a linear model of testosterone’s binding to SHBG in which one molecule of SHBG binds one molecule of testosterone with a single binding affinity constant are erroneous.348 These studies have shown that testosterone’s binding to SHBG is a dynamic multistep process that includes heterogeneity in circulating isoforms of SHBG dimer, an allosteric interaction between 806 SECTION V Reproduction the two binding sites on SHBG such that the binding affinities of the two binding sites on SHBG are not equivalent, and convergence to an energetically favored bound state in which both sites are occupied.348 The free testosterone levels computed using this dynamic multistep binding with allosteric match closely the values measured directly by equilibrium dialysis.348 In men found to be androgen-deficient, measurement of LH levels helps distinguish between testicular (LH elevated) and hypothalamic-pituitary (LH low or inappro­ priately normal) defects.64 Men with hypogonadotropic hypogonadism may require measurement of serum prolactin, serum iron, and total iron binding capacity; evaluation of other pituitary hormones; and a pituitary MRI. The diagnostic yield of pituitary imaging to exclude pituitary tumor can be improved by selecting men whose total testosterone level is less than 150 ng/dL or who have panhypopituitarism, persistent hyperprolactinemia, or symptoms of tumor mass.251,252 There is considerable debate about the usefulness and cost-effectiveness of hormonal evaluation and the extent to which androgen deficiency should be investigated in men presenting with ED. Between 8% and 10% of men with ED have low testosterone levels; the prevalence of androgen deficiency increases with advancing age.216,349-351 The prevalence of low testosterone levels is not significantly different among men who present with ED and in an age-matched population.141 These data are consistent with the proposal that ED and androgen deficiency are two common but independently distributed disorders.141 However, it is important to exclude androgen deficiency in this patient population. Androgen deficiency is a correctable cause of sexual dysfunction, and some men with ED and low testosterone levels will respond to testosterone replacement. Androgen deficiency may be a manifestation of serious systemic disease and may have additional deleterious effects on the individual’s health; for instance, androgen deficiency might contribute to osteoporosis and loss of muscle mass and function. In large studies,64 only a small fraction of men with ED and low testosterone levels have been found to have space-occupying lesions of the hypothalamic-pituitary region.251,252 In one large survey, all of the hypothalamic-pituitary lesions were found in men with serum testosterone levels lower than 150 ng/dL.252 Therefore, the cost-effectiveness of the diagnostic workup to rule out an underlying lesion of the hypothalamic-pituitary region can be increased by limiting the workup to men with serum testosterone levels less than 150 ng/dL.64 If the history, physical examination, and laboratory tests do not identify medical problems needing further workup, then a cost-effective approach is to prescribe a trial of oral PDE5 inhibitor provided there are no contraindications (e.g., nitrate use). Tests that evaluate the integrity of penile vasculature and blood flow352,353 are not needed in most patients with ED, are reserved for patients in whom the results of these tests would alter the management or prognosis, and should be performed only by those with considerable experience with their use. The penile brachial blood pressure index is a simple and specific, but not a sensitive, index of vascular insufficiency. It is rarely used today in the evaluation of ED. Intracavernosal injection of a vasoactive agent such as PGE1 can be useful as a diagnostic as well as a potential therapeutic modality. This procedure can reveal whether the patient will respond to this therapeutic modality and can facilitate patient education about the procedure and its potential side effects. Failure to respond to intracaver- nosal injection can raise the suspicion of vascular insufficiency or a venous leak that might need further evaluation and treatment. Most men with ED do not need duplex color sonography, cavernosography, or pelvic angiography.10,11,341,342,352 For instance, angiography could be useful in a young man with arterial insufficiency associated with pelvic trauma. Similarly, suspicion of congenital or traumatic venous leak in a young men presenting with ED would justify a cavernosography. In each instance, confirmation of the vascular lesion might lead to consideration of surgery. Duplex ultrasonography can provide a noninvasive evaluation of vascular function.352 Nocturnal penile tumescence testing is not needed for most patients being evaluated for ED and is recommended only for a limited number of patients with a high clinical suspicion of psychogenic ED or situational problems, or to document preoperatively poor penile rigidity, or for medical-legal reasons. Although recording of nocturnal penile tumescence in a sleep laboratory for successive nights can help differentiate organic from psychogenic impotence, this test is expensive and labor intensive. The introduction of portable RigiScan devices in 1985 has provided clinicians with a reliable means of continuously monitoring penile tumescence and rigidity at home.353 It is a multicomponent device that the patient wears at bedtime for 2 to 3 nights. It has two wire gauge loops that are placed around the base and tip of the penis that record changes in penile circumference and rigidity. Data are stored and downloaded via a software program that allows for interpretation. For most cases, a careful history of nighttime or early morning erections provides a reasonable correlation with nocturnal penile tumescence and RigiScan studies.353 Evaluation of Women With Sexual Dysfunction Sexual dysfunction is diagnosed by clinical interview and, when necessary, physical examination. Sexual function questionnaires can be used to monitor treatment.354-356 One such instrument is the FSFI.354,355 Despite the original intention of such questionnaires to monitor treatment progress, they are frequently (mis)used to diagnose sexual dysfunction in women who have not been clinically assessed. Moreover, the FSFI is based on the DSM-IV criteria of sexual disorders, which are grounded in the conceptualization of female sexual response beginning with conscious desire leading to a phase of arousal, then orgasm, and then resolution, these phases being in set order, discrete, and necessary for normal function. The limitations of the FSFI include the lack of recognition of triggered desire and the normality of beginning an experience initially sexually neutral, the possibility of sexual satisfaction without orgasm, and a focus on partnered sex, which interferes with accurate scoring of women who are currently unpartnered.355 Although the FSFI has been used in most studies of women’s sexual function including those of women with endocrine disease, more contemporary instruments such as the National Survey of Sexual Attitudes and Lifestyles (Natsal-3)356 better reflect the importance of sexual satisfaction in contrast to many previous instruments. This attribute of Natsal-SF instrument is particularly important because patients may report satisfaction despite dysfunction, and dissatisfaction can occur in the context of a functional response357: women’s satisfaction may or may not include orgasms.200 A recent study confirms strong links between sexual satisfaction and sexual motivation.358 CHAPTER 20 Sexual Dysfunction in Men and Women TABLE 20-6 Directed Physical Examination of the Woman With Sexual Dysfunction General Examination Signs of systemic disease leading to low energy, low desire, or low arousability, such as anemia, bradycardia, and slow relaxing reflexes of hypothyroidism Signs of connective tissue disease, such as scleroderma or Sjögren syndrome, that are associated with vaginal dryness Disabilities that might preclude movements involved in caressing a partner, self-stimulation, or intercourse Disfigurements or presence of stomas or catheters that may decrease sexual self-confidence leading to low desire, low arousability External Genitalia Sparsity of pubic hair suggesting low adrenal androgens Vulval skin disorders, including lichen sclerosis, that may cause soreness with sexual stimulation and reduce sexual sensitivity Cracks or fissures in the interlabial folds suggestive of chronic candidiasis Labial abnormalities that may cause embarrassment or sexual hesitancy Past genital mutilation: absent labia minora, minimal or no clitoral tissue Introitus Vulval disease involving introitus, such as pallor, friability, loss of elasticity and moisture of vulval atrophy; lichen sclerosis; recurrent splitting of the posterior fourchette manifested as just visible white lines perpendicular to the fourchette edge; disfigurement, narrowing from genital mutilation; abnormalities of the hymen, adhesions of the labia minora, swellings in the area of the major vestibular glands, allodynia (pain sensation from touch stimulus) of the crease between the outer hymenal edge and the inner edge of the labia minora—typical of provoked vestibulodynia Presence of cystocele, rectocele, prolapse interfering with the woman’s sexual self-image Inability to tighten and relax perivaginal muscles often associated with hypertonicity of pelvic muscles and midvaginal dyspareunia; abnormal vaginal discharge associated with burning dyspareunia Internal Examination Pelvic muscle tone, presence of tenderness, trigger points on palpation of deep levator ani due to underlying hypertonicity Full Bimanual Examination Presence of nodules or tenderness in the cul-de-sac or vaginal fornix and along uterosacral ligaments, retroverted fixed uterus as causes of deep dyspareunia Tenderness on palpation of posterior bladder wall from anterior vaginal wall suggestive of bladder disease Adapted from Basson R. Sexual dysfunction in women. N Engl J Med. 2006;354:1497-1506, used with permission. Physical Examination Physical examination, including pelvic and genital examination, is part of routine care (Table 20-6) and can be reassuring to the patient by confirming normal anatomy and tissue health. Unless dyspareunia is involved, it is not often that physical examination identifies the cause of sexual dysfunction. For some women with a history of coercive or abusive sexual experiences, such examination may cause extreme anxiety. The reason for the examination and an explanation of what will and will not be done should be provided before the examination begins. If the woman would prefer to invite her partner to be present, then the careful examination can be highly educational for both partners. In women with genitopelvic penetration pain disorder with a marked component of vaginismus, the vaginal examination should be delayed until psychological 807 therapy renders it possible and informative for both the patient (and partner if present) and the clinician. Laboratory Testing Laboratory testing plays a small role in women’s sexual evaluation. Estrogen activity is best evaluated by history and examination. The commercially available estradiol radioimmunoassays lack the sensitivity and precision required to measure the low concentrations present in the older woman; also, these assays do not measure estrone, the major estrogen after menopause. As discussed earlier, serum testosterone levels do not correlate with sexual function, even when LC-MS/MS assays are used.65,66 The circulating testosterone levels may not reflect intracrine production, metabolism, or activity of androgens. Measurement of testosterone metabolites has been proposed as a marker of intracrine plus gonadal production of testosterone,67 but the circulating levels of these metabolites have been shown to be similar in women with and without sexual dysfunction.66 The optimal markers of total androgen activity and the clinical usefulness of these metabolites remain to be demonstrated. Prolactin or thyrotropin should be measured if there are other symptoms that suggest abnormality. MANAGEMENT OF SEXUAL DYSFUNCTION IN MEN Treatment of Hypoactive Sexual Desire in Men There is need to focus on the couple when the patient has a sexual partner. Treating the sexual dysfunction in the male partner improves the female partner’s sexual function and satisfaction. Comorbid depression should be treated and relationship difficulties addressed. The efficacy of cognitive and behavioral therapies has not been evaluated systematically in men with HSDD. Testosterone therapy should be considered in men with HSDD who have androgen deficiency, even though there are no randomized trials of testosterone in men with HSDD. Much of the information about the effects of testosterone on sexual desire has emerged from open-label trials of testosterone in hypogonadal men.64,124,359-362 These trials recruited men based on the presence of low testosterone levels alone.124,359-362 Testosterone therapy in these trials has been associated with significant improvements in overall sexual activity, sexual desire, attention to erotic cues, and the duration and frequency of nocturnal penile erections.64,124,359-362 Meta-analyses of randomized testosterone trials mostly in middle-aged and older men reported greater improvements in nocturnal erections, sexual thoughts and motivation, number of successful intercourses, scores of erectile function, and overall sexual satisfaction in men receiving testosterone than in those receiving placebo.64,134,136,142,362 A large placebo-controlled randomized trial of testosterone in older men with decreased sexual desire and unequivocally low testosterone levels, funded by the National Institutes of Health, is currently in progress and should provide novel information about the efficacy of testosterone.363 Treatment of Erectile Disorder The current practice employs a stepwise approach that first utilizes minimally invasive therapies that are easy to use 808 SECTION V Reproduction Psychosexual counseling of the couple Optimize medical management of comorbid conditions Evaluate cardiovascular risk and potential contraindications to PDE5I use No contraindications to PDE5I use PDE5I use contraindicated Initiate PDE5I therapy Satisfactory clinical response Unsatisfactory clinical response Recommend second-line therapies: vacuum constriction device, intraurethral alprostadil, or intracavernosal alprostadil • Evaluate: appropriate use, compliance, couple relationship, AEs, or fear of AEs • Escalate dose to maximal allowed or maximal tolerable dose Satisfactory clinical response Unsatisfactory clinical response Unsatisfactory response Periodic medical follow-up Penile implant Figure 20-9 An algorithmic approach to the treatment of erectile dysfunction in men. AE, adverse effects; PDE5I, phosphodiesterase 5 inhibitor. and have fewer adverse effects and progresses to more invasive therapies that may require injections or surgical intervention after the first-line choices have been exhausted (Fig. 20-9). The physician should discuss the risks, benefits, and alternatives of all therapies with the couple. The selection of the therapeutic modality should be based on the underlying cause, patient preference, the nature and strength of the relationship with his sexual partner, and the absence or presence of underlying CVD and other comorbid conditions.10,11,341,342 All patients with ED can benefit from psychosexual counseling.10,11,341,342,364-368 In the execution of good medical practice, treatment of all associated medical disorders should be optimized. In men with diabetes mellitus, efforts to optimize glycemic control should be instituted, although improving glycemic control may not improve sexual function. In men with hypertension, control of blood pressure should be optimized and, if possible, the therapeutic regimen may be modified to remove antihypertensive drugs that impair sexual function. This strategy is not always feasible because almost all antihypertensive agents have been associated with sexual dysfunction; the frequency of this adverse event is less with converting enzyme inhibitors and angiotensin receptor blockers than with other agents. First-Line Therapies Psychosexual Counseling. The major goals of psychosexual therapy are to reduce performance anxiety, develop the patient’s sexual skills and knowledge, modify negative sexual attitudes, and improve communication between partners.364 Counseling can be of benefit in both psy­ TABLE 20-7 Goals of Psychosexual Therapy in Men With Sexual Dysfunction • • • • Reduce performance anxiety; train the couple to avoid “spectatoring” and be “sensate focused” Identify relationship problems and improve partner communication and intimacy Modify sexual attitudes and beliefs Improve couple’s sexual skills Adapted from Rosen RC. Psychogenic erectile dysfunction: classification and management. Urol Clin North Am. 2001;28:269-278. chogenic and organic causes of sexual dysfunction364-370 (Table 20-7). An individual’s focus on sexual performance rather than erotic stimulation is a major factor in the pathophysiology of psychogenic ED364,365; this behavior is referred to as spectatoring. Many experts recommend a sensate focus treatment approach in which the couple avoids intercourse and engages in nongenital, nondemanding, pleasure-seeking exercises in order to reduce performance anxiety.364 Involving the partner in the counseling process helps dispel misperceptions about the problem, decreases stress, enhances intimacy and the ability to talk about sex, and increases the chances of successful outcome.364 Counseling sessions are also helpful in uncovering conflicts in relationships, psychiatric problems, alcohol and drug abuse, and significant misperceptions about sex. As many men and women may harbor misinformation and unrealistic expectations about sexual performance and age-related changes CHAPTER 20 Sexual Dysfunction in Men and Women 809 TABLE 20-8 Clinical Pharmacology of Selective PDE5 Inhibitors* Feature Sildenafil Vardenafil Tadalafil Avanafil Commercial name Tmax T 12 Viagra 0.5-2.0 h 3-4 h Levitra 0.7-0.9 h 4-5 h Stendra, Spedra 30-45 min 5h Onset of erection (min) Muscle selectivity (ratio of PDE6 IC50/PDE5 IC50) Retinal selectivity (ratio of PDE11/PDE5 IC50), higher number indicates greater selectivity Effect of food and alcohol Protein binding Bioavailability 30-60 11 (most selective) 780 15-45 25 1160 (most selective) Cialis 2h 16.9 h (young) 21.6 (old) 20-30 min 187 (least selective) 5 (least selective) Cmax decreased 96% 41% Minimal change 94% Not available No change 94% 15% Absorption delayed 98-99% Not available O CH3CH2O CH3 N HN O N N CH2CH2CH3 O3S N N H HOOC CH3 Sildenafil OH S N N N H N CO2H H 15 min >100-fold >10,000-fold O N * * X Z * N Y (R0) q N O R3 O N N O N H Cl N H R2 R1 O CO2H Vardenafil OH Tadalafil N N Avanafil *Comparative pharmacokinetic data on the three oral selective PDE5 inhibitors. Selectivity refers to the ratio of the IC50 for a PDE isoform other than PDE5 to the IC50 for PDE5. A higher number implies greater selectivity. Sildenafil is more selective than tadalafil for PDE5 relative to PDE11, but it is less selective than tadalafil for PDE6 relative to PDE5. Cmax, maximum plasma concentration; IC50, 50% inhibitory concentration; PDE, phosphodiesterase; T 12 , half-life; Tmax, time to peak concentration. Adapted from references 99, 101, 373. in sexual function, cognitive restructuring techniques are helpful in correcting sexual myths and beliefs.364 There is a paucity of outcome data on the effectiveness of this psychobehavioral therapy, but meta-analyses have reported benefit from group psychotherapy administered in conjunction with PDE5 inhibitors.367 Selective Phosphodiesterase 5 Inhibitors (Tables 20-8 and 20-9). Selective PDE5 inhibitors are safe and effective and have become widely accepted as first-line therapy for patients with ED, except in men for whom these drugs are contraindicated.9-11,99,101,341,342,370-372 Selective PDE5 inhibitors are contraindicated in men using nitrates on a regular basis, in those with heart disease in whom sexual activity is not recommended, and in those with nonarteritic anterior ischemic optic neuropathy.10,11,99,101,341,342,371,372 Mechanisms of Action. Three classes of enzymes—adenylyl cyclase, guanylyl cyclase, and PDEs—play an important role in regulating the intracavernosal concentrations of cAMP and cGMP. PDEs hydrolyze cAMP and cGMP, thus reducing their concentrations within the cavernosal smooth muscle.100,101,104-106,373-376 Although PDE isoforms 2, 3, 4, and 5 are expressed in the penis, only PDE5 is specific to the nitric oxide/cGMP pathway in the corpora cavernosa.376 PDE inhibitors sildenafil, vardenafil, tadalafil, avanafil, and udenafil are relatively selective inhibitors of PDE5.100,101,104-106,373-399 These drugs block the hydrolysis of cGMP induced by nitric oxide, thus promoting cavernosal smooth muscle relaxation. The action of these drugs requires an intact nitric oxide response, as well as constitutive synthesis of cGMP by the smooth muscle cells of the corpora cavernosa. By selectively inhibiting cGMP catabolism in the cavernosal smooth muscle cells, PDE5 inhibitors restore the natural erectile response to sexual stimulation but do not produce an erection in the absence of sexual stimulation. TABLE 20-9 Common Adverse Effects of Selective Phosphodiesterase Inhibitors 1. 2. 3. 4. 5. 6. 7. 8. 9. Headache Flushing Dyspepsia Nasal and sinus congestion Dizziness Abnormal vision* Back pain* Myalgia* Hearing problems *These adverse effects are related to nonselective inhibition of phosphodiesterase isoforms in other tissues. Headache, flushing, and nasal congestion are related to the drug’s mechanism of vasodilator action. Adapted from Wespes E, Rammal A, Garbar C. Sildenafil no-responders: hemodynamic and morphometric studies. Eur Urol. 2005;48:136-139; Brock GB, McMahon CG, Chen KK, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol. 2002;168:1332-1336; Morales A, Gingell C, Collins M, et al. Clinical safety of oral sildenafil citrate (Viagra) in the treatment of erectile dysfunction. Int J Impot Res. 1998;10:69-73; Katz EG, Tan RB, Rittenberg D, Hellstrom WJ. Avanafil for erectile dysfunction in elderly and younger adults: differential pharmacology and clinical utility. Ther Clin Risk Manag. 2014;10:701-711. Clinical Pharmacology (see Table 20-8). Although the three currently available PDE inhibitors have some structural similarities, they differ in their selectivity and pharmacokinetics (see Table 20-8). The common adverse effects of the available PDE5 inhibitors—headache, visual problems, flush, and myalgias—are related to nonselective inhibition of PDE isoforms 6 and 11 in other organ systems101 (see Table 20-9). The selectivity of PDE5 inhibitor is the ratio of its inhibitory potency for PDE isoforms other than type 810 SECTION V Reproduction 5 relative to its inhibitory potency for PDE isoform.101 For PDE6, tadalafil is the most selective and sildenafil is the least selective; for PDE11, vardenafil is the most selective and tadalafil is the least selective.101 The retinal side effects of sildenafil are related to inhibition of PDE6 in the retina, whereas muscle aches experienced by a small fraction of men using tadalafil are related to inhibition of PDE11 in the skeletal muscle.101 Pharmacokinetics (see Table 20-8). After oral administration of sildenafil, peak plasma concentrations are achieved within 30 to 120 minutes, after which plasma con­ centrations decline, with a half-life of 4 hours (see Table 20-8).100,373-382 Vardenafil achieves peak concentrations within 0.7 to 0.9 hour and has a half-life of 4 to 5 hours. The peak concentrations of tadalafil are achieved at 2 hours, and its half-life of 16.9 hours in young men is significantly longer than the half-lives of sildenafil and vardenafil. The half-life of tadalafil is even longer in older men (21.6 hours) than in young men (16.9 hours).100,373-376 Because of the relatively short half-lives of vardenafil and sildenafil, these drugs should be taken 1 to 4 hours before the planned intercourse; in contrast, tadalafil, because of its longer half-life, does not have to be taken on demand, although it can be.100,373-376 The second-generation PDE5 inhibitors avanafil and udenafil have a more rapid onset of action than the first-generation PDE5 inhibitors sildenafil, vardenafil, and tadalafil.377-380 Food, particularly a high-fat meal and large amounts of alcohol, can delay and decrease the absorption of sildenafil.381,382 However, early pharmacokinetic studies have not reported changes in maximum serum concentrations or absorption rates of vardenafil or tadalafil due to food or moderate alcohol ingestion.376 Efficacy. The orally active, selective PDE5 inhibitors— sildenafil, vardenafil, avanafil, udenafil, and tadalafil— have been shown to be effective and safe in randomized clinical trials of men with ED.9-11,379-405 In men treated with oral, selective PDE5 inhibitors, the rates of successful intercourse vary from 50% to 65%, and rates of improved erections vary from 70% to 75%.379-405 The selective PDE5 inhibitors are effective in men of all ethnic groups and ages379-405 who have ED due to a multitude of causes, although response rates vary in different patient subgroups.379-405 Introduced to the U.S. market in March 1998, sildenafil citrate (Viagra, Pfizer, New York, NY) was the first effective oral agent for the treatment of ED.406 The efficacy of sil­ denafil has been demonstrated in men with organic, psychogenic, or mixed ED in multiple randomized controlled trials (RCTs)383-390,406 and confirmed by meta-analyses of randomized trials.386-388 In these trials, patients receiving sildenafil experienced greater increments in the number of successful attempts per month, penile rigidity, frequency of vaginal penetration, and maintenance of erection than those receiving placebo.386-388 Increasing doses of sildenafil were associated with higher mean scores for the frequency of penetration and maintenance of erections after sexual penetration. The mean scores for orgasms, intercourse satisfaction, and overall satisfaction were also significantly higher in the sildenafil group than in the placebo group.386-388 Sildenafil also is an effective treatment for ED in men with diabetes mellitus.389,390 A meta-analysis of randomized clinical trials of sildenafil confirmed its efficacy in improving erectile function in men with diabetes mellitus.390 In the vardenafil efficacy trials, 5-, 10-, and 20-mg doses of vardenafil were all superior to placebo in improving erectile function domain scores; the improvements in erectile function scores were dose-related.391-397 Vardenafil improved rates of vaginal penetration, penile rigidity, intercourse success, and satisfaction with sexual experience in men with ED from diverse causes.391-397 Similarly, in randomized, clinical trials, 2.5-, 5-, 10-, and 20-mg doses of tadalafil were each superior to placebo in improving erectile function scores.398-402 The beneficial effects of tadalafil were dose-related.398-402 Two new PDE5 inhibitors have been introduced recently in clinical practice. Avanafil has a very rapid onset of action because of its rapid absorption, which allows it to reach maximum circulating concentration in about 30 to 45 minutes.377-379 Therefore, a majority of patients taking avanafil are able to engage in sexual activity within 15 minutes.377-379 Udenafil also has a relatively rapid onset of action, with a time to maximum serum concentrations of 1.0 to 1.5 hours. It has been approved in Korea, Russia, and the Philippines, but not in the United States.380 PDE5 inhibitors are effective in men with ED due to a variety of causes, including spinal cord injury and radical prostatectomy.389,390 In general, baseline sexual function correlates positively with response to PDE5 inhibitors, and patients with diabetes mellitus or previous prostate surgery respond less well than patients with psychogenic or vasculogenic ED.389,390 Because there is no baseline characteristic that predicts the likelihood of failure to respond to silden­ afil therapy, a therapeutic trial of PDE5 inhibitors should be tried in all patients except in those in whom it is contraindicated.372 Adverse Effects (see Table 20-9). In clinical trials, the adverse effects that have been reported with greater frequency in men treated with PDE5 inhibitors than in those treated with placebo include headaches, flushing, rhinitis, dyspepsia, muscle aches, and visual disturbances.101,372,403-405 The occurrence of headache, flushing, and rhinitis, a direct consequence of nonselective PDE5 inhibition in other organ systems, is related to the administered dose. These drugs do not affect semen characteristics.407,408 No cases of priapism were noted in the pivotal clinical trials. Several cases of nonarteritic anterior ischemic optic neuropathy have been reported after ingestion of oral PDE5 inhibitor use.409,410 This condition is characterized by the sudden onset of monocular visual loss due to acute ische­ mia of the anterior portion of the optic nerve in the absence of demonstrable arteritis. This may progress to partial or complete infarction of the optic nerve head resulting in permanent visual loss or visual field cuts.409,410 Although a cause-and-effect relationship with PDE5 inhibitor use has not been established, patients with history of sudden visual loss should not be treated with PDE5 inhibitors without ophthalmologic evaluation. Recently the U.S. Food and Drug Administration (FDA) noted several reports of sudden hearing loss with and without vestibular symptoms, such as tinnitus, vertigo, or dizziness, in temporal relationship to administration of sildenafil, vardenafil, and tadalafil in postmarketing surveillance. Hearing loss was also reported in a few patients in clinical trials of these drugs.411,412 Hearing loss has been noted in patients using sildenafil for the treatment of pulmonary arterial hypertension. Although a causal relationship has not been established, the temporal relationship between the use of PDE5 inhibitors and the onset of sudden hearing loss prompted the FDA to recommend change in the product labeling for the drug class. One observational study has reported an association of PDE5 inhibitor use with an increased risk of melanoma.413 Cardiovascular and Hemodynamic Effects. In postmarketing surveillance of adverse events associated with sildenafil use, several instances of myocardial infarction and sudden death were reported in men using sildenafil in temporal CHAPTER 20 Sexual Dysfunction in Men and Women relation to the ingestion of the drug414; many of these deaths occurred in individuals who also were taking nitrates. Because most men presenting with ED also have high prevalence of cardiovascular risk factors, it is unclear whether these events were causally related to the ingestion of sildenafil, underlying heart disease, or both.414 In controlled studies,415-418 oral administration of 100 mg of sil­ denafil to men with severe coronary artery disease produced only a small decrease in systemic blood pressure and no significant changes in cardiac output, heart rate, coronary blood flow, and coronary artery diameter. In a separate pooled analysis of five randomized, placebo-controlled trials of vardenafil,417 the overall frequency of cardiovas­ cular events was similar in vardenafil-treated men and placebo-treated men. However, vardenafil treatment was associated with a mild reduction in blood pressure (4.6-mm Hg decrease in systolic blood pressure) and a small increase in heart rate (2 beats per minute).418 This led the American Heart Association and other experts to conclude that preexistent coronary artery disease by itself does not constitute a contraindication for the use of PDE5 inhibitors (Table 20-10).418-424 Drug-Drug Interactions. Sildenafil is metabolized mostly by the CYP2C9 and the CYP3A4 pathways. Cimetidine and erythromycin, inhibitors of CYP3A4, increase the plasma concentrations of sildenafil. HIV protease inhibitors may also alter the activity of the CYP3A4 pathway and affect the clearance of sildenafil.425 Conversely, sildenafil is an inhibitor of the CYP2C9 metabolic pathway, and its administration could potentially affect the metabolism of drugs metabolized by this system, such as warfarin and tolbutamide. Combined administration of sildenafil and ritonavir results in significantly higher plasma levels of sildenafil than sildenafil given alone.425 There are similar TABLE 20-10 Guidelines for the Use of Selective Phosphodiesterase Inhibitors 1. Do not administer selective PDE5 inhibitors to men taking long-acting or short-acting nitrate drugs on a regular basis. 2. If the patient has stable coronary artery disease, is not taking long-acting nitrates, and uses short-acting nitrates only infrequently, the use of selective PDE5 inhibitor should be guided by careful consideration of risks. 3. Do not administer selective PDE5 inhibitors within 24 hours of the ingestion of any form of nitrate. 4. Advise men about the risks of the potential interaction between selective PDE5 inhibitors and nitrates, nitrate donors, and α-adrenergic blockers. Concurrent use of nitrates, nitrate donors, or α-adrenergic blockers could result in hypotension that could be serious. 5. In men with preexisting coronary artery disease, assess the risk of inducing cardiac ischemia during sexual activity before prescribing PDE5 inhibitors. This assessment may include a stress test. 6. In men who are taking vasodilators and diuretics for the treatment of hypertension or congestive heart failure, consider the potential risk of inducing hypotension because of potential interaction between PDE5 inhibitors and vasodilators, especially in patients with low blood volume. 7. In HIV-infected men, consider potential drug-drug interactions between selective PDE5 inhibitors and antiretroviral drugs and antimicrobial agents. ACC/AHA, American College of Cardiology/American Heart Association; HIV, human immunodeficiency virus; PDE5, phosphodiesterase isoform 5. Adapted from Cheitlin MD, Hutter AM Jr, Brindis RG, et al. Use of sildenafil (Viagra) in patients with cardiovascular disease: Technology and Practice Executive Committee [published erratum appears in Circulation. 1999;100(23):2389]. Circulation. 1999;99(1):168-177; Lue TF, Giuliano F, Montorsi F, et al. Summary of recommendations on sexual dysfunctions in men. J Sex Med. 2004;1:6-23. 811 interactions with other drugs, including saquinavir and itraconazole. Therefore, the doses of PDE5 inhibitors should be reduced appropriately in men taking protease inhibitors or erythromycin. Grapefruit juice can alter oral drug pharmacokinetics by different mechanisms. Grapefruit juice given in normal amounts (e.g., 200-300 mL) or as whole fresh fruit segments can inactivate irreversibly intestinal CYP3A4, thus reducing presystemic metabolism and increasing oral bioavailability of PDE5 inhibitors.426 Although the magnitude of this problem in clinical practice is unknown, it seems prudent to warn men who are contemplating the use of PDE5 inhibitors not to ingest more than a small amount of grapefruit juice. The most serious interactions of PDE5 inhibitors are with the nitrates. The vasodilator effects of nitrates are augmented by PDE5 inhibitors; this also applies to inhaled forms of nitrates such as amyl nitrate or nitrites that are sold under the street name “poppers.” Concomitant administration of the two vasodilator drugs can cause a potentially fatal decrease in blood pressure.193-195 PDE inhibitors should be used carefully in men taking α-adrenergic blockers. In men with congestive heart failure or those receiving vasodilator drugs or those who are using complex regimens of antihypertensive drugs, blood pressure should be monitored after initial administration of PDE5 inhibitors.193-195 Several trials have demonstrated the safety of administering PDE5 inhibitors in combination with α-adrenergic blockers in men with ED and LUTS.193-195 Therapeutic Regimens. Excellent therapeutic guidelines have been published by expert panels from several societies.99,371,372,419 To minimize the risk of hypotension and adverse cardiovascular events in association with the use of PDE5 inhibitors, the American Heart Association/ American College of Cardiology has published a list of recommen­dations (see Table 20-10), which should be followed rigorously.419 In most men with ED, sildenafil is started at an initial dose of 25 or 50 mg. If this dose does not produce any adverse effects, the dose can be titrated up to 100 mg.99,371,372,427 Further dose adjustment should be guided by the therapeutic response to therapy and occurrence of adverse effects. Vardenafil should be started at an initial dose of 10 mg; the dose should be increased to 20 mg or decreased to 5 mg depending on the clinical response and the occurrence of adverse effects. Unit doses higher than 20 mg are not recommended. Tadalafil is started at an initial unit dose of 10 mg, with further adjustment of dose based on effectiveness and side effects. Tadalafil need not be taken more frequently than once every 48 hours. In men taking protease inhibitors (particularly ritonavir and indinavir), erythromycin, ketoconazole, itraconazole, or large amounts of grapefruit, the doses of PDE5 inhibitors should be reduced, and doses greater than 25 mg of sil­ denafil, 5 mg of vardenafil, or 10 mg of tadalafil are not recommended. Sildenafil and vardenafil are taken at least 1 hour before sexual intercourse and not more than once in any 24-hour period; because of its longer half-life, tadalafil need not be taken immediately before intercourse. Based on the results of the randomized clinical trials,408,428,429 the FDA has approved 2.5 mg or 5 mg tadalafil once daily for the treatment of ED. In the pivotal trials, men using 2.5 mg or 5 mg tadalafil once daily experienced greater improvements in erectile function compared with those taking a placebo.408,428,429 Subsequent open-label extension studies indicated that once-daily 5 mg tadalafil for up to 2 years was effective in maintaining improvements 812 SECTION V Reproduction in erectile function.408,428,429 Thus, tadalafil may be taken at 2.5 mg or increased to 5 mg, as tolerated. The adverse events associated with once-daily administration of tadalafil included headaches, indigestion, back pain, muscle aches, nasal congestion, and flushing and were similar to those observed with on-demand tadalafil ingestion.408,428,429 Once-daily regimen of tadalafil had no significant effect on semen or reproductive hormone levels.408 The Use of Phosphodiesterase 5 Inhibitors in Men With Coronary Artery Disease (see Table 20-10).424 Before prescribing PDE5 inhibitors, cardiovascular risk factors should be assessed. If the patient has hypertension or symptomatic coronary artery disease, the treatment of those clinical disorders should be addressed first.424 The use of nitrates must be ascertained because PDE5 inhibitors are contraindicated in individuals taking any form of nitrates regularly. PDE5 inhibitors should not be used within 24 hours of the use of nitrates or nitrate donors.10,11,423,424 Sexual activity can induce coronary ischemia in men with preexisting coronary artery disease420; therefore, men contemplating use of ED therapies should undergo assessment of their exercise tolerance. One practical way to assess exercise tolerance is to have the patient climb one or two flights of stairs. If the individual can safely climb one or two flights of stairs without angina or excessive shortness of breath, he can likely engage in sexual intercourse with a stable partner without inducing similar symptoms. Exercise testing before prescribing PDE5 inhibitors may be indicated in some men with significant heart disease to assess the risk of inducing cardiac ischemia during sexual activity.419-421 Selective PDE inhibitors have been shown not to impair the ability of patients with stable coronary artery disease to engage in exercise at levels equivalent to that attained during sexual intercourse.419-421 Similarly, each of the three PDE5 inhibitors has been shown not to have significant adverse effects on hemodynamics and cardiac events in carefully selected men with ED who did not have any contraindication for the use of PDE5 inhibitors.417-424 None of the PDE5 inhibitors adversely affects total exercise time or time to ischemia during exercise testing in men with stable angina.417-424 Treatment of Patients Who Do Not Respond to Phosphodiesterase 5 Inhibitors. Although oral PDE5 inhibitor therapy has revolutionized the management of ED, not all men will respond to this treatment. The cumulative probability of intercourse success with sildenafil citrate increases with the number of attempts, reaching a maximum after eight attempts.430 Based largely on these data,430 the failure to respond to PDE inhibitor therapy has been defined as the failure to achieve satisfactory response even after eight attempts of either the highest approved dose (e.g., 100 mg sildenafil) or the highest tolerable dose of PDE inhibitor, whichever is lower. Many factors may contribute to apparent treatment failure, including failure to take the medi­ cation as recommended, suboptimal dose, dose-limiting adverse effects, psychological issues, partner and relationship issues, incorrect diagnosis, and patient-specific pathophysiologic factors.430-432 In clinical trials of PDE5 inhibitors, treatment failures were reported predominantly in men who had diabetes mellitus, non-nerve sparing radical prostatectomy, cavernosal nerve damage, venous leak, and high disease severity.430-432 In an evaluation of cavernosal smooth muscle biopsies in sildenafil nonresponders, Wespes and coworkers432 found severe vascular lesions and cavernosal smooth muscle atrophy and fibrosis to be the underlying pathologic processes. Patients may not take the medication appropriately because of inadequate instructions, failure to understand the instructions, adverse effects, or fear of adverse effects.430-432 Oral PDE5 inhibitors are taken optimally 1 to 2 hours before planned intercourse. The medication is unlikely to be effective if it is taken immediately before intercourse; a high-fat meal and large amounts of alcohol may further affect the maximal serum concentrations of sildenafil citrate. Similarly, patients may not take the appropriate dose because of side effects or fear of side effects. The men who have been misdiagnosed as having ED and whose primary sexual disorder is unresponsive to PDE5 inhibitors may be incorrectly deemed treatment failures. For instance, men with HSDD, Peyronie disease, or orgasmic or ejaculatory disorder would not be expected to respond to PDE5 inhibitors. The anxiety associated with resumption of sexual activity and unresolved relationship and partner issues can attenuate response to treatment. The sexual partner may not be willing or able to engage in sexual activity because of relationship issues, sexual disorder, or real or perceived health issues. Patients who report lack of satisfactory response to initial administration of PDE5 inhibitors should be asked about the time of drug administration, the dose taken, and adverse effects experienced. Psychological and partner issues should be evaluated. The dose of PDE5 inhibitor should be increased gradually as tolerated. Should the patient not respond to maximal tolerable doses of PDE5 inhibitors, PDE5 inhibitors can be combined with vacuum devices or intraurethral therapy. Second-line therapies such as intracavernosal injections should be pursued. The men who are unresponsive to oral PDE5 inhibitors and secondline therapies may find penile implant an acceptable alternative.430 Cost-Effectiveness of Phosphodiesterase 5 Inhibitor Use for Erectile Disorder. A number of studies have evaluated the economic cost of treating ED in men in managed care health plans.433-437 One simulation estimated sildenafil citrate cost to be approximately $11,000 per quality-adjusted life year (QALY) that it produces.435 This amount is less than that for many other accepted treatments for medical disorders that cost less than $50,000 to $100,000 per QALY; thus, the cost-effectiveness of PDE5 inhibitor therapy compares favorably with other accepted medical therapies. Other analyses have concluded that PDE5 inhibitors and vacuum constriction devices are the most cost-effective of all the available therapeutic options.433-437 Several recent analyses have shown that the financial burden imposed by patients with ED on managed care plans is surprisingly small.433-437 In one such cost-utility analysis, the monthly cost of providing ED-related treatment services in a health plan with 100,000 members amounted to less than $0.10 per member.435 Thus, the failure of many insurance companies to cover the cost of PDE5 inhibitor therapy is not informed by cost-utility analyses. Second-Line Therapies Vacuum Devices for Inducing Erection. The vacuum devices consist of a plastic cylinder, a vacuum pump, and an elastic constriction band.438-440 The plastic cylinder fits over the penis and is connected to a vacuum pump. The negative pressure created by the vacuum within the cylinder draws blood into the penis, producing an erection. An elastic band slipped around the base of the penis traps the blood in the penis, maintaining an erection as long as the rubber band is retained. The constriction band should not be left in place for more than 30 minutes. Also, only vacuum devices with a pressure-limiting mechanism should be recommended to prevent injury due to high vacuum. Limited data on the efficacy of vacuum devices from open-label trials indicate that these devices are safe, CHAPTER 20 Sexual Dysfunction in Men and Women relatively inexpensive, and moderately effective.438-440 They can impair ejaculation, resulting in entrapment of semen. Some couples dislike the lack of spontaneity engendered by the use of these devices. Partner cooperation is important for successful use of these devices.440 Intraurethral Therapies. An intraurethral system for delivery of alprostadil called MUSE (medicated urethral system for erection; VIVUS, Menlo Park, CA) was released in 1997. Alprostadil is a stable, synthetic form of PGE1, which results in generation of cAMP and activation of protein kinase A. Activated protein kinase A stimulates K+ channels, resulting in K+ efflux from the cell. In addition, protein kinase A– mediated processes also result in a net decrease in intracellular calcium, favoring smooth muscle cell relaxation. Alprostadil, when applied into the urethra, is absorbed through the urethral mucosa into the corpus cavernosum. In comparison to intracavernosal injection of PGE1, intraurethral PGE1 is easier to administer and has a lower frequency of adverse effects, particularly penile fibrosis. Alprostadil is available in 125-, 250-, 500-, and 1000-µg strengths. Typically, the initial alprostadil dose of 250 µg is applied in the clinician’s office to observe changes in blood pressure or urethral bleeding secondary to misapplication of the device into the urethra. Initial randomized, placebo-controlled studies reported 40% to 60% success rates, defined as having at least one successful sexual intercourse during a 3-month study period.441-443 In clinical practice, only about a third of men using intrauretheral alprostadil will respond.444 Common side effects of intraurethral alprostadil are penile pain and urethral burning in up to 30% of patients441-444; its use also may cause dizziness, hypotension, and syncope in a small fraction of users. Intraurethral alprostadil can cause mild burning or itching in the vagina of the sexual partner. Intraurethral alprostadil should not be used by men whose partners are pregnant or planning to get pregnant. Intracavernosal Injection of Vasoactive Agents (Table 20-11). The use of intracavernosal injections of vasoactive agents has been a cornerstone of the medical management of ED since the early 1980s. Patients can be taught to inject a TABLE 20-11 Guidelines for Intracavernosal Therapy 1. Do not prescribe intracavernosal therapy to men who have psychiatric disorders, hypercoagulable states, sickle cell disease; those who are receiving anticoagulant therapy; or those who are unable to comprehend the risks or take appropriate action should complications occur. 2. Designate a physician or a urologist to be available to handle emergencies related to complications of intracavernosal injections such as prolonged erection and priapism. 3. Instruct the patient in the injection technique, the risks of intracavernosal therapy, and the steps to be taken in the event of prolonged erection or priapism. 4. Administer the first injection in the office and observe the blood pressure and heart rate response. This provides an excellent opportunity for educating the patient, observing adverse effects, and determining whether the patient will respond to intracavernosal therapy. 5. Start with a low dose of alprostadil and titrate the dose based on the erectile response and the duration of erection. Adjust the dose of alprostadil to achieve an erection that is sufficient for sexual intercourse but that does not last more than 30 minutes. 6. If the erection does not abate in 30 minutes, the patient should be instructed to take a tablet of pseudoephedrine or brethine or an intracavernosal injection of phenylephrine. If this is not effective, the patient should call the designated physician or the urologist, and come to the emergency room. 813 vasoactive agent into their corpora cavernosa using a 27- or 30-gauge needle prior to the planned intercourse. Erections occur typically 15 minutes after intracorporal injection and last 45 to 90 minutes. Although intracavernosal injection therapy is highly effective,445-452 it is associated with significantly higher complication rates than oral therapy and should be used only by practitioners who are experienced in the use of this therapy and who can provide emergency medical support to their patients in the event of a serious adverse event, such as priapism. Although several different agents—PGE1, papaverine, and phentolamine—have been used alone or in combination,445-453 only intracavernosal PGE1 has been approved for clinical use. The long-term data on the efficacy and safety of intracavernosal therapy are sparse. Several formulations of alprostadil (PGE1) are commercially available (Caverject, Pharmacia; Prostin VR, Pharmacia; Edex, Schwarz Pharma). PGE1 binds to PGE1 receptors on the cavernosal smooth muscle cells, stimulates adenylyl cyclase, increases the concentrations of cAMP, and is a powerful smooth muscle relaxant. The usual dose is 5 to 20 µg, and response to therapy is dose-related and should be titrated.445-451 In one placebo-controlled efficacy trial, the intracavernosal alprostadil injection resulted in satisfactory sexual performance after more than 90% of administrations, and approximately 85% of men and their partners reported satisfactory sexual activity.445 Intracavernosal alprostadil is more effective than intraurethral alprostadil.449 The common adverse effects of intracavernosal therapy include penile pain, occurrence of hematoma, formation of corporal nodules, penile fibrosis, and prolonged erections.445-452 Despite the effectiveness of this approach in producing rigid erections, many patients do not relish injecting a needle into their penis; therefore, it is not surprising that long-term dropout rates are high. Intracavernosal injections of papaverine, phentolamine, forskolin, and VIP have also been used, although these agents are not approved by the FDA.453 Papaverine, derived originally from the poppy seed, is a nonspecific PDE inhibitor, which increases both intracellular cAMP and cGMP. It has a greater propensity to induce priapism and fibrosis with long-term use, and efficacy and long-term safety data from randomized, placebo-controlled trials are lacking. Therefore, there is insufficient information to evaluate its efficacy and safety. Phentolamine is a competitive α1- and α2-adrenergic antagonist that contributes to smooth muscle relaxation. As a single agent it is minimally efficacious, but it has been used to potentiate the effects of papaverine, VIP, and PGE1.453 Randomized clinical trial data on its efficacy and safety are lacking. Therefore, there is insufficient information to evaluate its efficacy and safety. A serious concern with the use of intracavernosal injection therapy is priapism. In patients who develop a prolonged or painful erection with PGE1, either brethane 5 mg or pseudoephedrine 60 mg, administered orally, may be of benefit. If priapism persists longer than 4 hours, patients should be instructed to seek medical care in which aspiration alone or with the injection of an α-adrenergic agent is used to induce detumescence. If this fails, surgical therapy may be indicated to reverse a prolonged erection; otherwise, anoxic damage to the cavernosal smooth muscle cells and fibrosis can occur. Third-Line Therapies Penile Prosthesis. The penile prostheses are invasive and costly, but they can be an effective method for restoring 814 SECTION V Reproduction erectile function for patients with advanced organic disease who are unresponsive to other medical therapies, have significant structural disorders of the penis (e.g., Peyronie disease), or have suffered corporal loss from cancer or traumatic injury.454-456 Penile implants are paired supports that are placed in each of the two erectile bodies. There are two basic types of penile implants: hydraulic (fluid filled), referred to as inflatable prostheses; and malleable, semirigid rods, which are bendable but always remain firm in the penis.454-456 Penile prostheses come in a variety of lengths and girths. Implantation surgery usually takes less than an hour and in most cases can be done as an outpatient procedure under general or regional anesthesia. Infection and mechanical malfunction are the most common problems with penile prostheses. With recent improvements in materials and design, the chance of mechanical malfunction has decreased to 5% to 10% in the first 10 years.454-456 Infection occurs in 1% to 3% of cases, but infection rates can be higher in revision surgery, especially in men with diabetes mellitus. The total cost of penile prosthesis implantation varies from $3,000 to $20,000, depending on the type of device used and the community in which the procedure is performed. There are no randomized efficacy trials, but retrospective analyses have reported that greater than 80% of patients and 70% of partners are pleased with their prosthesis and the togetherness that it brings to their relationship.454-457 Testosterone Replacement in Androgen-Deficient Men Presenting With Erectile Disorder. Testosterone treatment does not improve sexual function in men with ED who have normal testosterone levels.1,64,134,135,142 It is not known whether testosterone replacement improves sexual function in impotent men with borderline serum testosterone levels. Many, but not all, of the impotent men with low testosterone levels experience improvements in their libido and overall sexual activity with androgen replacement therapy.1,64,134,135 The response to testosterone therapy even in this group of men is variable, because of the coexistence of other disorders such as diabetes mellitus, hypertension, CVD, and psychogenic factors.1,134,135,142 ED in middle-aged and older men is a multifactorial disorder, often associated with other comorbid conditions such as diabetes mellitus, hypertension, medications, peripheral vascular disease, psychogenic factors, and endstage renal disease. Therefore, it is not surprising that testosterone treatment alone may not improve sexual function in all men with androgen deficiency. Testosterone induces NOS activity,130,131 has trophic effects on cavernosal smooth muscle and ischiocavernosus and bulbospongiosus muscles,132 increases penile blood flow,145 and is essential for achieving venous occlusion in animal models.129 These observations have led to speculation that testosterone might improve response to PDE5 inhibitors; however, as discussed earlier, data from randomized trials have not shown the superiority of testosterone over placebo in improving erectile function in men with ED who have low testosterone levels and in whom the PDE5 inhibitor dose has been optimized.148 Therapies With Either Unproven Efficacy or Limited Efficacy Data. There are insufficient efficacy data to support the use of trazodone458 or yohimbine459 in men with ED. The literature on the effectiveness of herbal therapies is difficult to interpret because of lack of consistency in product formulations and potencies, contamination of herbal products with PDE5 inhibitors, poor trial design, and paucity of randomized clinical trial data.460-464 One randomized trial of Korean red ginseng reported this product to be effective in the treatment of ED461; these data need further confirmation. Icariin is a flavonoid, derived from several species of plants, whose extracts have been known in herbal medicine to produce aphrodisiac effects and enhance erectile function.464 Dipyridamole also inhibits PDE5 and can augment the effects of nitric oxide. 4-Methylpiperazine and pyrazolopyrimidine, components of the lichen Xanthoparmelia scabrosa, have also been claimed to inhibit PDE5.463 The use of these or other herbal therapies is not recommended.463 Apomorphine also functions as a dopamine agonist and acts centrally to initiate erection; its main adverse effect is nausea. Gene Therapy and Erectile Disorder. The goal of gene therapy for ED is to introduce novel genetic material into the cavernosal smooth muscle cells to restore normal cellular function and produce a therapeutic effect.465-467 Gene therapy has been proposed as a treatment option for diseases that have a vascular origin, such as arteriosclerosis, congestive heart failure, and pulmonary hypertension.465-467 ED may be particularly amenable to gene therapy because of the easily accessible external location of the penis,465-467 which permits direct injection into the corpora cavernosa. A tourniquet placed around the base of the penis limits entry of the injected material into the systemic circulation. This is a distinct advantage of the gene therapy of penile diseases over gene therapy for other systemic diseases because introduction of the genetic material into the systemic circulation can potentially induce adverse systemic effects due to insertion of the material into an incorrect organ or vascular bed. Additionally, in the penis, only a small number of cells need to be transfected because the interconnection of smooth muscle cells in the corpus cavernosum by gap junctions allows second messenger molecules and ions to be transferred to other interconnected smooth muscle cells.465-467 The low turnover rate of the vascular smooth muscle cells of the penis allows the desired gene to be expressed for long periods of time. The current strategies of gene therapy for ED treatment have focused on the molecules that regulate corporal smooth muscle relaxation or neovascularization (Table 20-12).465-467 A number of candidate genes have been explored, including the penile-inducible NOS, eNOS, VIP, calcitonin-related peptide, maxi-K+ channel, vascular endothelial growth factor (VEGF), the brain neurotrophic factor, angiopoietin-1, neurturin (a member of the glial cell line–derived neurotrophic factor family), superoxide dismutase, IGF-1, protein kinase G (PKG-1α), and Rho A/ Rho kinase465-475 (see Table 20-12). A number of vectors have been used to transfer exogenous genes, including adenoviruses, adeno-associated viruses, retroviruses, sinbis viruses, replication-deficient retroviruses, liposomes, naked DNA, and gold nanoparticles.465-481 Garban and associates468 first demonstrated that gene therapy can be performed in the penis by utilizing naked cDNA (complementary DNA) encoding the penile-inducible NOS gene leading to physiologic benefit in the aging rat. Christ and colleagues469 injected hSlo cDNA (which encodes the human smooth muscle maxi-K+ channel) into the rat corpora cavernosa and demonstrated increased gap junction formation and enhanced erectile responses to nerve stimulation in the aged rat. Adenoviral constructs encoding the eNOS and CGRP genes were shown to reverse agerelated ED in rats.470,471 In these studies, both eNOS and CGRP expression were sustained for at least 1 month in the corpora cavernosa of the rat penis. Five days after transfection with the AdCMVeNOS or AdRSVeNOS viruses, aged rats had significant increases in erectile function as determined by cavernosal nerve stimulation and pharmacologic injection with the endothelium-dependent vasodilator CHAPTER 20 Sexual Dysfunction in Men and Women 815 TABLE 20-12 Physiologic Targets for Gene Therapy Gene Target Vector and Mechanism Reference Nitric oxide isoforms Increase eNOS, nNOS, and iNOS activity in the cavernosal smooth muscle Protein inhibitor of NOS (PIN) Maxi-K+ channel Antisense and short hairpin RNA (shRNA) constructs targeting PIN (protein inhibitor of NOS) Transfer of maxi-K+ channels using a plasmid vector that carries the hSlo gene encoding the α-subunit of the maxi K+ channel; first human trial demonstrates the safety and feasibility of gene therapy in humans Replication-deficient recombinant adenoviruses carrying the PKG-1α Transfer of VEGF cDNA into rat corpora cavernosa to promote neovascularization Adenovirus-mediated transfer of human angiopoietin-1 Transfer of brain-derived neurotrophic factor using adeno-associated virus Transfer of neurotrophin 3 gene using HSV vector Neurturin (NTN), a member of glial cell line–derived neurotrophic factor (GDNF) family Transfection of corpora cavernosa of streptozotocin-treated diabetic rats using pcDNA3 carrying VIP cDNA Adenoviral transfer of CGRP in aged rats Adenoviral-mediated gene transfer of extracellular superoxide dismutase injected into the corpora cavernosa Adenoviral-mediated gene transfer of IGF-1 Champion 1999; Bivalacqua 2000, 2003, 2005; Gonzalez-Cadavid 2004; Kendirci 2005; Wessels 2006 Magee et al 2007 PKG-1α VEGF Angiopoietin-1 BDNF Neurotrophin 3 gene Neurturin VIP CGRP Superoxide dismutase Insulin-like growth factor-1 Christ et al 2002, 2004, 2004; Melman 2003, 2005, 2006, 2007, 2008; So et al 2007 Bivalacqua et al 2007 Rogers et al 2003; Buchardt et al 2005; Dall’Era et al 2008 Ryu et al 2006; Jin et al 2010 Rogers et al 2005; Gholani et al 2003 Bennett et al 2005 Kato et al 2009 Shen et al 2005 Bivalacqua et al 2001; Deng 2004 Bivalacqua 2003; Brown 2006; Lund 2007 Pu et al 2007 BDNF, brain-derived neurotrophic factor; cDNA, complementary DNA; CGRP, calcitonin gene–related peptide; HSV, human syncytial virus; IGF-1, insulin-like growth factor 1; NOS, nitric oxide synthase (epithelial [e], inducible [i], or neuronal [n] isoforms); PIN, protein inhibitor of NOS; PKG, protein kinase G; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal protein. Adapted from Melman and Davies481; Condorelli et al, 2010; Harraz et al465; Strong et al466; Deng et al.467 acetylcholine and the type PDE5 inhibitors.470,471 In one study, intracavernous injection of adeno-associated virus construct carrying the brain-derived neurotrophic factor gene improved erectile function after cavernosal nerve injury.475 This neurotrophic factor purportedly restored neuronal NOS in the major pelvic ganglion, thus enhancing the recovery of erectile function after bilateral cavernous nerve injury.475 In other studies, intracavernosal VEGF injection and adeno-associated virus-mediated VEGF gene therapy were each shown to reverse venogenic ED in rats.472,473 These preclinical studies and others using additional targets for gene therapy such as CGRP, superoxide dismutase, and Rho A/Rho kinase provide evidence that in vivo gene transfer can be accomplished technically. The translation of these preclinical data into human trials has been slow and unsuccessful so far. Ion Channel Innovations, Inc. has completed a phase I trial of slow K+ channel in men with ED.95,477,478 In this trial, hmaxi-K, a “naked” DNA plasmid carrying the human cDNA encoding for the gene for the α-subunit of the human smooth muscle maxi-K channel, was injected directly into the penises of 11 men with ED. Patients who received the highest dose of hmaxi-K experienced significant improvements in their erectile function that was sustained for the 24-week duration of the trial. This trial demonstrated the feasibility and safety of injecting naked DNA into the human penis.477,478 A trial of hmaxi-K in patients with overactive bladders is ongoing. Phase I gene therapy trials using VEGF and hepatocyte growth factor have been conducted in patients with peripheral vascular disease and chronic limb ischemia and to prevent the development of stent restenosis; these trials have reported low frequency of serious adverse effects. However, phase II studies have not confirmed efficacy. Thus, the early therapeutic promise of gene therapy has yet to be realized. Successful gene therapy may require introduction of multiple gene products using vectors with higher efficiency of transfection of a larger number of target cells and more prolonged action than can be realized with the current generation of vectors. The Potential of Stem Cell Therapy for Erectile Disorder. The past decade has seen considerable interest in the transplantation of stem cells derived from bone marrow, adipose tissue, or skeletal muscle into the corpora cavernosa.482-490 However, it has become apparent that the stem cells, even when injected within the corpora cavernosa, escape rapidly from the penis and hone into the bone marrow.482-490 The mechanism of the reported improvements in intracavernosal pressure after stem cell injection into the corpora cavernosa remains unclear.485 The safety and efficacy of stem cell therapy in humans has yet to be demonstrated. We do not know whether transplanted human mesenchymal stem cells (hMSCs) can differentiate into functional cavernosal smooth muscle cells and restore erectile capacity in men with ED. Also, the long-term outcomes including the tumorigenic potential of these transplanted progenitor cells are unknown. hMSCs may also be attractive gene delivery vehicles because these cells can replicate in vitro as well as in vivo, thus potentially providing a large pool of cells.486,487 Initial studies have demonstrated that rat mesenchymal stem cells, expanded and transfected ex vivo and implanted into the corpora cavernosa, are capable of expressing the gene product of interest.482-487 Stem cell therapy using stem cells carrying angiogenic or neurotrophic genes or proteins is also being explored. Although several animal studies have reported improved erectile function with hMSC transplantation, few studies have shown evidence of long-term stem cell survival in the cavernosal smooth muscle or evidence of differentiation of the transplanted stem cells into endothelial cells or cavernosal smooth muscle cells.482-490 Management of Retrograde Ejaculation Case reports have shown benefit from methoxamine, imipramine, midodrine, and ephedrine, although randomized 816 SECTION V Reproduction clinical trial data are lacking.491-493 Induction of fertility in men with retrograde ejaculation may require retrieval of sperm from the urinary bladder after sexual stimulation or electrostimulation of the prostatic nerve plexus per rectum plus assisted reproductive techniques, such as intrauterine insemination or in vitro fertilization with or without intracytoplasmic sperm injection using the retrieved sperm.494-497 MANAGEMENT OF SEXUAL DYSFUNCTION IN WOMEN Psychotherapeutic methods are the mainstay of management of the female sexual dysfunction; Frühauf and coworkers498 provided a systematic review and metaanalysis of these interventions in 2013. On an investigational basis a small number of medications have received limited study (see Table 20-13). Management of Low Desire and Arousal in Women Management of sexual interest/arousal disorder (SIAD) begins with explaining the circular model of sexual response (see Fig. 20-1B) as a basis for discussing which areas are problematic with one or preferably both partners. When insufficient emotional intimacy is identified, the normality of low interest to be sexual can be clarified; referral for couple counseling may be indicated. When the lack of sexual context and stimuli are contributing factors, simply emphasizing the requirement of appropriate environment and sufficiently erotic stimuli is usually sufficient, but referral to a sex therapist may be appropriate. Nonsexual distractions, fears about sexual outcome, self-monitoring of sexual response, anxiety, low self-image, and depression all interrupt the mental appraisal of stimuli. These issues can be explained and addressed. The main modalities of treatment are cognitive therapy, sex therapy, and psychoeducation. Psychoeducation Psychoeducation includes giving information while simultaneously soliciting the woman’s input to share thoughts and feelings that emerge in session, which are then addressed and processed. It includes teaching cognitive techniques and can help dispel widespread myths about sexuality in women (e.g., that the absence of desire preceding sexual activity denotes sexual dysfunction). Bibliotherapy with self-help reading material or videos can be helpful. TABLE 20-13 Investigational Pharmacotherapy for Women’s Sexual Dysfunctions Sexual Dysfunction Sexual interest arousal disorder Mechanisms of Dysfunction Loss of brain’s sexual arousability to sexual stimuli Drug Type Drugs with specific serotonin receptor subtype of agonist/ antagonist profile Melanocortin agonists Dopamine agonists Genital arousal disorder: estrogen deplete Genital arousal disorder despite estrogen replete Serotonergic antidepressant– associated orgasmic disorder Off Label/Investigational Drug Comments Flibanserin: 5HT1A agonist and 5HT2A antagonist, weak partial agonist D4 Recent FDA approval despite marginal benefit and potentially serious side effects521a Bremelanotide–synthetic peptide: α-melanocytestimulating hormone analogue-agonist at MCR1, MC3R, and MC4R receptors Bupropion Small RCT showed benefit for women’s arousal disorder with in home use of nasal drug 45 min before sex.73 Sponsor has discontinued trials Loss of genital vasocongestion in response to sexual stimulation Loss of genital vasocongestion in response to sexual stimulation Loss of genital vasocongestion in response to sexual stimulation To provide local substrate for estrogen and testosterone intracrine synthesis Local vaginal DHEA Selective tissue estrogenic activity regulator with androgenic and progestogenic properties To enhance the action of NO-PDEIs Tibolone Former orgasmic response absent or extremely delayed PDEIs Sildenafil Sildenafil, tadalafil, vardenafil One small 4-month study, in nondepressed premenopausal women showed increased arousability and sexual response, no increase in initial desire.110 Recent phase III RCT showing increased maturation of vaginal epithelium, lower pH and sexual benefit in all domains of response from local vaginal DHEA for 12 weeks558 RCT of dysfunctional women showed tibolone marginally superior to 50 µg/140 µg combined transdermal estradiol/norethisterone.112 Major problem is distinguishing the subgroup of women with genital arousal disorder who have reduced genital vasocongestion. Small RCTs in diabetes146 and MS116 showed only modest benefit from sildenafil. Recent 8-week RCT with very strict entry criteria showed benefit from 50-100 mg.510 Superscript numbers indicate references at the end of the chapter. D4, dopamine 4 receptor; DHEA, dehydroepiandrosterone; 5-HT, serotonin; ISSWSH, International Society for the Study of Women’s Sexual Health; MC1R, melanocortin-1 receptor; MS, multiple sclerosis; MSH, melanocyte-stimulating hormone; NO, nitric oxide; PDEIs, phosphodiesterase inhibitors; RCTs, randomized controlled trials. CHAPTER 20 Sexual Dysfunction in Men and Women For some women, information on anatomy and physiology is necessary. Cognitive Behavioral Therapy Cognitive behavioral therapy (CBT) can assist the woman to recognize, challenge, and in time, change her negative and often catastrophic self-view imposed by underlying illness, including endocrine conditions or their imposed infertility. Some of the exaggerated or catastrophic thoughts amenable to cognitive therapy include “sex is only for well women,” “I am no longer fertile, so I am no longer sexually attractive,” and “if intercourse is too painful to include, then no one will want me.” Identifying these biased/ maladaptive thoughts is the first step: changing such thoughts to be more evidenced-based is then practiced. Empiric support for benefit from targeting cognitions and emotions during sex in order to increase physical and subjective arousal is emerging.42,499 Mindfulness-Based Cognitive Therapy New to Western medicine is the addition of mindfulness, which is of benefit for medically well women with sexual dysfunction,500,501 those with pelvic cancer,502 and those with PVD.503 Mindfulness is an Eastern practice of medi­ tation: the learned skill is to be fully present and accepting of all that is sensed in that moment. Attention is enhanced by the gradual ability to identify thoughts arising in that moment, be they future- or past-oriented, but not to engage in them but ultimately to view these negative or positive thoughts more distantly as if they are just sensations not dissimilar to physical sensations. The practice of mindfulness focuses the attention on sexual sensations rather than on self-monitoring. Functional brain imaging performed before and after mindfulness training supports the clinical finding that such training lessens self-referencing of sensations and emotions, including pain and anxiety.504-506 Resources in the community and through the Internet for mindfulness practice can be given. Recently, an adapted form of CBT blended with mindfulness was defined—the treatment is called mindfulnessbased cognitive therapy (MBCT). Regular mindfulness practice is an integral component. As with CBT, the skill of detecting maladaptive thoughts including those critical or evaluative is learned but with simple observation of their presence and an acknowledgment that they are just mental events, not necessarily the truth; there is no focus here to change thoughts. MBCT is used to treat or prevent anxiety disorder and depression and has been adapted to treat arousal and desire disorders and chronic pain of PVD.500,501,503,507 Current clinical research includes the use of detailed treatment manuals for clinicians with separate versions for patients. The aim is to provide sufficiently detailed manuals for non–mental health professionals and non–sexual medicine specialists to provide CBT and MBCT to small groups of women. This small group format is consistently rated as a major benefit.508 Sex Therapy Sex therapy usually focuses on sensate focus exercises whereby each partner takes turns giving and receiving sensual and, later on, sexual touches, caresses, and kisses. Initially, genital areas and breasts are off-limits. The idea of any goal or expectation is put aside. The couple together with the clinician decides as to when breasts and genital 817 areas are on-limits. Ultimately, the act of intercourse (or vaginal penetration with dildo), may be included—but not as the focus. Outcome of Psychological Treatments for Women’s Sexual Dysfunctions Data are limited regarding the long-term effects of psychological treatments for women’s sexual dysfunction. A systematic review and a meta-analysis of controlled clinical trials for female and male sexual dysfunction published before 2009 was recently conducted.498 None of these studies targeted patients with endocrine disease. The overall conclusion was that psychosocial interventions for sexual dysfunction were efficacious. For women with sexual dysfunction associated with the hormonal changes arising from breast cancer treatment, a systematic review suggests that the most effective interventions are couple-based psychoeducational interventions that include an element of sex therapy.509 Management of Women’s Orgasmic Disorder Although in clinical practice CBT methods and mindfulness training have been used in women with orgasmic disorder, outcome research is sparse. The 2013 metaanalysis found clear evidence of benefit in both symptom severity and sexual satisfaction for women with orgasmic dysfunction, but only three trials were identified.498 To date there is no pharmacologic treatment for orgasmic disorder. In one trial with highly selective inclusion criteria, sil­ denafil was reported to improve orgasm dysfunction associated with SSRI use,510 whereas a recent small trial of transdermal testosterone did not improve sexual function beyond placebo as measured by the Sabbatsberg Sexual Self-Rating Scale as the primary outcome.511 However, testosterone therapy was associated with statistically significant increase in the number of sexually satisfying events (SSEs) per month. Confirmation of these findings and their clinical relevance is awaited (Table 20-13). Management of Genitopelvic Pain/Penetration Disorder (Dyspareunia and Vaginismus) The most common type of dyspareunia is PVD, which affects about 12% to 18% of women.512 PVD and the other common type of dyspareunia—that stemming from vul­ vovaginal atrophy—are typically associated with pelvic muscle hypertonicity and reflexive involuntary contractions when penetration is anticipated. DSM-5 therefore merged the previous terms of dyspareunia and vaginismus. The use of pain-free transperineal four-dimensional ultrasound on pelvic floor muscle morphometry in women with PVD confirmed abnormalities both at rest (e.g., small levator hiatus area, small anorectal angle suggesting increased tone) and with maximal contraction. These findings are thought to be consistent with weakness and poor control of pelvic muscle.513 Pelvic floor physiotherapy is frequently part of sexual pain management. Management of Provoked Vestibulodynia There is no definite association between PVD and endocrine status, but recent investigation of the presence of polymorphism in the guanine triphosphate cyclohydrolase gene (GCH1) is of interest. Specific single nucleotide polymorphisms (SNPs) in the GCHI gene are associated with 818 SECTION V Reproduction reduced pain sensitivity. Although no correlation between PVD and the pain-protective GCH1 SNP combination was found, patients with PVD using oral contraceptives and carrying the specified SNP combination had higher pain sensitivity.514 This finding is in keeping with the documented clinical experience that some women with PVD benefit from discontinuing oral contraceptives.515 Randomized trials of oral and topical medications for PVD including tricyclics, anticonvulsants, lidocaine, flu­ conazole, cromolyn, and nifedipine gave similar results in analgesic benefit compared to placebo.516 Investigational botulinum toxin was statistically inferior to placebo in reduction of sexual distress.516 Because medical treatments for PVD have been unsatisfactory, an interdisciplinary biopsychosexual approach is currently encouraged.517,518 Although rarely chosen by women, surgical vestibulectomy can be of benefit; however, exclusion factors are numerous519 and benefit is obtained mostly in women with acquired as opposed to lifelong histories. Other common negative prognostic factors for successful vestibulectomy include comorbid muscle tightening, widespread allodynia of the introital margin, involvement of the Skene duct openings, unwillingness to have sex therapy if offered, and comorbid depression and anxiety. Negative prognostic factors for all treatment modalities include disgust and contamination sensitivity, erotophobia (the tendency to respond with negative effects to sexual cues), and coexistence of depression and anxiety.520 Recent research suggests an expanded stress model of chronic pain,520,521 focusing on allostasis, which is the physiologic stability maintained by various mechanisms within the body that promote adaptation to stress in the longer term. Allostatic load/overload522 depicts the wear and tear of body systems, including the brain, from excessive stress. Given the debility and negative consequences of recurrent pain, the stress produced by the pain disorder maintains a vicious cycle. This cycle may be especially applicable to the sexual pain of PVD: a stress-induced and maintenance model for the pain of PVD was recently described,516 similar to the vicious cycle depicted for migraine.521 Personality traits of women with PVD, including negative self-evaluation and fear of negative evaluation by others, predisposes to self-labeling as sexually substandard or even sexually inadequate. The stress model of pain posits that sexual stress not only contributes to the chronic pelvic muscle hypertonicity but also maintains a heightened reactivity of the pain circuitry from top-down modulation afforded by neuroplasticity. The cause of the sensitization within the nervous system has not been established with certainty, but internal stress appears to be a likely cause. Women with PVD report higher levels of premorbid depression and anxiety, as well as perfectionism, reward dependency, fear of negative evaluation, increased prevalence of type D personality, self-dislike, harm avoidance, hypervigilance for pain, and shyness compared to women without PVD.523-527 Given that mood disorder is so commonly comorbid with PVD, management needs to address both pain and the depression/anxiety. There is evidence of benefit from CBT, which was sustained over the 2 years of follow-up.528 Catastrophic thinking, amenable to CBT approaches, is par­ticularly common in women with PVD.529 The lack of self-acceptance apparent in women with PVD, considered to be a pain-maintaining stress, is potentially amenable to MBCT given that a key component of MBCT is acceptance. Significant beneficial effects beyond waitlist control were confirmed from a brief mindfulness-based group intervention on both cotton swab–induced vestibular pain and psychological measures of pain.503,508 Management of Phobic Reflex Pelvic Muscle Contractions (Vaginismus) Heightened pelvic muscle tone, often along with muscle tension elsewhere, may be the only physical findings in women reporting dyspareunia or painful but unsuccessful attempts at penetration. Often guided by pelvic floor physiotherapists, management involves progressive desensiti­ zation and progressive vaginal accommodation using a variety of relaxation techniques and vaginal inserts.530 The term dilators is preferably avoided, because women fear that their therapy is going to (painfully) stretch the vagina. Psychotherapies including mindfulness and CBT are often used to reduce anxiety.531 A 2013 waitlist controlled study of in-clinic physical therapy suggests better outcomes than traditional guidance for insert therapy at home.532 Testosterone Therapy for Women With Sexual Dysfunction As discussed earlier in this chapter, testosterone deficiency has not been demonstrated in women diagnosed with sexual dysfunction, either by measurement of blood levels or by measurement of androgen metabolites. Several randomized trials of testosterone therapy have been conducted, mostly in postmenopausal women. These testos­ terone trials were conducted largely in women distressed by reduced sexual desire since their menopause. The eligibility criteria for these trials did not meet the diagnostic criteria for DSM-IV, HSDD, or for the newly coined SIAD of DSM-5. The first series of randomized trials showed a statistically significant improvement in the numbers of SSEs in women receiving testosterone: on average SSEs increased from 2 to 3 per month to 5 per month in women on active drug and to 4 per month in women receiving placebo. Testosterone was given transdermally in the form of a patch with a nominal testosterone delivery of 300 µg/day. Doses of either 150 or 450 µg/day were not effective.533 Serum testosterone and dihydrotestosterone concentrations exceeded the target high-normal serum concentrations of these hormones in a significant number of women receiving testosterone.534 Women on active drug reported further improvements in arousal, pleasure, orgasm, self-image, and responsiveness to a statistically significantly greater extent than did women receiving placebo. These testosterone trials focused mostly on surgically menopausal women, but one testosterone patch study included naturally menopausal women535 with comparable results. Two testosterone studies recruited naturally and surgically menopausal women who were not receiving estrogen therapy. One of these studies reported a significant increase in SSEs in the naturally menopausal women from the active drug but not in the smaller subgroup of surgically menopausal women.536 Only 464 of the 814 participants completed treatment, with similar distribution of high discontinuation rates in all three arms. A second study of 272 naturally menopausal women, of whom a total of 73% of the participants were not receiving systemic estrogen therapy, showed a significant increase in SSEs.537 On the basis of these studies, all by the same sponsor, the transdermal testosterone patch was approved in Europe, but not in North America or elsewhere, for the treatment of surgically menopausal women with persistently distressing low sexual desire despite adequate systemic estrogen therapy that did not include conjugated equine estrogens. Although approved, the patch is no longer available in Europe because of low sales. CHAPTER 20 Sexual Dysfunction in Men and Women Negative Trials of Testosterone Therapy In contrast to the previous studies, two large phase III RCTs by a different sponsor of 1172 postmenopausal women, approximately half of whom received systemic estrogen, showed no benefit of transdermal testosterone in the form of a gel over placebo.538 Full study details are not available as these two studies have not been published. The entry criterion of distressingly reduced sexual desire after menopause was similar to the previous randomized trials; end points were numbers of SSEs per month and the level of sexual desire as assessed from a daily diary. There is very little information available on the effects of testosterone in premenopausal women. One study of 261 women who experienced loss of their former sexual satisfaction reported minimal benefit from testosterone.539 Testosterone Plus a Phosphodiesterase Inhibitor One small study evaluated the efficacy of a pharmacologic dose of testosterone (0.5 mg sublingually) to improve attentiveness for erotic cues in women with low desire.540 The testosterone was combined with sildenafil, a PDE inhibitor, to facilitate genital congestion. In those women who at baseline already showed high levels of subconscious attention bias for erotic cues (as measured by a masked version of the emotional Stroop task), this drug combination had no effect, and in fact, testosterone alone reduced attention to erotic cues. However, the women with lower arousability or sensitivity to erotic cues at baseline showed increased physiologic genital congestion and increased awareness of the genital sensations and of sexual desire when they subsequently viewed an erotic video. The safety of intermittent use of markedly supraphysiologic testosterone therapy is unknown. Limitations of Trials of Testosterone Therapy in Women A major limitation of testosterone trials to date is the targeted population. Studies have recruited women with decreased desire since menopause, most of whom retained the ability to be aroused and sexually satisfied on at least some (on average 50%) occasions. Thus, an absence of sexual desire between sexual encounters has been the focus. However, research confirms this to be well within the range of normal female sexual experience. The majority of 3250 multiethnic middle-aged women in the SWAN cohort indicated that although moderately or extremely sexually satisfied, they never or very infrequently felt desire.541 In an online survey of 3687 younger women, 1865 were assessed to be without evidence of sexual dysfunction, specifically confirming their easy sexual arousal— close to one third of this group rarely or never began a sexual experience with a sense of sexual desire.542 As noted earlier in this chapter, an incentives/motivations model of human sexual response is now considered to more accurately reflect sexual experience, desire for sex per se being just one of many reasons or incentives for sex. When absent at the beginning of a sexual encounter, desire can be triggered along with arousal after effective stimulation. Clinical trials have been conducted largely in women who were able to have satisfactory sexual experiences 50% of the time, leading to the criticism that these women probably did not have a biologic cause or consistent sexual dysfunction to merit any hormonal therapy.543-545 The studies of postmenopausal women showed improvements in desire and response domains using validated sexual questionnaires; however, increasing the degree and frequency of pleasure and arousal currently experienced by 819 study subjects does not necessarily imply that improvements would be observed in women with consistent absence of pleasure and arousal.543 There has been criticism of the use of statistical significance alone to evaluate the difference between the powerful placebo effects and active drug treatments in the area of women’s sexual dysfunction—especially that of low desire.546,547 It is suggested that effects might be better reported in terms of percentage of participants no longer meeting criteria for sexual dysfunction.546 As noted, the women in the testosterone trials were not recruited on the basis of a clinical diagnosis of sexual dysfunction but based on confirmation of low desire after menopause that caused distress. Risks of Testosterone Therapy Long-term safety data are lacking; published safety data from trials of up to 12 months’ duration are reassuring.547 There are theoretical reasons to consider exogenous testosterone as either a risk factor or a protective factor for breast cancer; high endogenous testosterone may be associated with an increased risk.545,548 A high endogenous testosteroneto-estrogen ratio can increase the risk of metabolic syndrome and CVD.549 However, some data suggest that low SHBG may be related to the risk of diabetes, metabolic syndrome, and CVD.550 In the Melbourne Women’s Midlife Health Project, weight gain and free androgen index, but not total testosterone, were strong predictors of CVD risk.551 Similar results were observed in 9-year follow-up of the SWAN cohort.552 In this study, free androgen index was positively and SHBG was negatively associated with the development of obesity. Weight gain preceded changes in the free androgen index and SHBG. The expert panel of the American Endocrine Society noted that the association between the free androgen index, CVD risk factors, and the metabolic syndrome phenotype appears to be more driven by obesity and low SHBG rather than testosterone.548 In most randomized trials, testosterone therapy has been administered in the background of concurrent estrogen therapy.548 However, the present advice, especially in North America, is to limit the duration of estrogen therapy. The Endocrine Society Task Force noted the limited safety data (median follow-up 4 months, range 6 weeks to 2 years). Furthermore, the efficacy data are focused on sexually responsive women without the common comorbid conditions including depression or antidepressant treatment. The task force requested a meta-analysis of transdermal testosterone RCTs; the gel studies, however, were excluded as they are only published in abstract form. Across all trials testosterone, used mostly in sexually responsive women, was associated with a statistically significant improvement in satisfaction, pleasure, orgasm, and libido.553 The Endocrine Society’s recommendations include the following548: 1. Most studies of testosterone therapy have targeted women with low desire but with the ability to be aroused and sexually satisfied on at least some (on average 50%) occasions. An incentives/motivations model of human sexual response is now considered to more accurately reflect sexual experience, desire for sex per se being just one of many reasons or incentives for sex. Studies are needed in women with low sexual interest/incentives and low arousal (and typically few orgasms) to reflect the prevalent clinical situation. 2. The expert panel recommended against the generalized use of testosterone by women for infertility or sexual dysfunction (but with the previous caveat in mind, except for a specific diagnosis of DSM-IV HSDD). 820 SECTION V Reproduction 3. The expert panel recommended against the routine treatment of women with low androgen levels due to hypopituitarism, adrenal insufficiency, bilateral oophorectomy, or other conditions associated with low androgen levels because of the lack of adequate data supporting efficacy and long-term safety of therapy. 4. The expert panel suggested consideration of a 3- to 6-month trial of a dose of testosterone resulting in a midnormal premenopausal value of plasma testosterone for postmenopausal women who request therapy for properly diagnosed HSDD and in whom therapy is not contraindicated. Needed Research in the Area of Testosterone Supplementation Further research is needed in women with low sexual interest/incentives and low arousal (and typically few orgasms) to reflect the prevalent clinical situation and to merit a diagnosis of SIAD. It is of note, however, that in the study of 125 women with and 125 women without HSDD when no group differences in androgen activity were found, 55% of the women with HSDD also met criteria for SIAD.554 Women diagnosed with SIAD and in remission from depression but taking antidepressants and women who, despite treatment, still score in the depressive range again reflect the clinical situation. Given that depression typically blunts sexual response, it has been an exclusion factor in clinical trials, as has the use of antidepressant therapy, but the reality is that mood disorder and its treatment commonly accompany complaints of low sexual desire.554-556 Not only is depression the factor most robustly linked to low desire in otherwise healthy women but also depression frequently determines the presence of sexual dysfunction even when other medical conditions including diabetes are comorbid.20 Oral Dehydroepiandrosterone for Sexual Dysfunction in Healthy Women Small trials of DHEA have been conducted in older healthy women. A recent systematic review and meta-analysis to evaluate the benefits and risks of systemic DHEA therapy for postmenopausal women557 included 15 randomized trials that were in general considered at high risk of bias and were of short duration. Statistically, DHEA use was marginally significant for desire, and there were no other significant improvements to outcome. The quality of evidence was considered low to moderate for benefit and very low for long-term harm. The recent Endocrine Society Task Force recommended against using DHEA in this setting.548 Local DHEA Therapy for Sexual Dysfunction in Healthy Women A recent phase III randomized trial of local vaginal DHEA therapy in postmenopausal women with vulvovaginal atrophy reported benefit of such therapy in improving vaginal symptoms of dryness and dyspareunia and all domains of sexual function.558 Moreover, all steroids, measured by mass spectrometry methods, remained in the postmenopausal range. Specifically, ADT-G remained constant. This delivery of precursor hormones to the target tissue may allow strictly local estrogen and androgen actions and may be a preferable choice for women in whom any systemic estrogen therapy is undesirable, such as those receiving aromatase inhibitors for breast cancer who can develop severe vulvovaginal atrophy. Rodent work suggests that local DHEA’s beneficial effect on genital sexual sensitivity might stem from its potent stimulatory effect on vaginal nerve fiber density.559 Estrogen Therapy for Women With Sexual Dysfunction Local vaginal therapy is recommended for dyspareunia associated with vulvovaginal atrophy. Low doses of estrogen can be supplied by a Silastic vaginal ring, vaginal cream, or a mucoadhesive vaginal tablet with similar benefit and low systemic absorption. Use of estradiol, 10 µg twice weekly and the estring (a Silastic ring containing estradiol, placed high in the vaginal vault), results in serum levels of 4.6 and 8.0 pg/mL, respectively. Progesterone is usually considered unnecessary for endometrial protection. Smaller doses of these formulations of estrogen are being investigated (e.g., 10 µg rather than 100 µg estradiol cream, 0.03 mg rather than 0.2 mg estriol vaginal pessaries) or have already been approved (e.g., 10-µg rather than 25µg estradiol vaginal tablets). When local estrogen does not ameliorate postmenopausal vulvovaginal atrophyassociated dyspareunia, comorbid PVD may be present.560 Of concern is that women using aromatase inhibitors and vaginal estrogen may show a small increase in serum estradiol levels561: a prospective trial of aromatase inhibition plus vaginal estrogen is under way. Investigational vaginal DHEA that appears not to increase serum levels of testosterone or estrogen has not been studied in breast cancer patients but appears promising.558 Intravaginal testosterone may alleviate symptoms,562 but any systemic absorption could increase serum estrogen through aromatization. Of particular relevance to women with past breast cancer is a 2013 report of a hyaluronic acid vaginal gel improving dyspareunia in 85% of women, comparable to women receiving vaginal estriol.563 When systemic estrogen is needed for other menopausal symptoms, it is sometimes necessary to give additional local estrogen for dyspareunia. In contrast, for some women, ultra-low-dose (0.014 mg/day) systemic transdermal estradiol may be sufficient for all menopausal symptoms including dyspareunia.564 If systemic supplementation improves insomnia and dyspareunia, sexual motivation would logically be expected to increase, but this has not been vigorously studied. No significant differences were found between estrogen and placebo groups in reported sexual satisfaction in the Women’s Health Initiative Trial.565 However, sexual dysfunction was not a primary focus of that trial; women with marked menopausal symptoms were excluded; and the instruments used to assess sexual function were substandard. REFERENCES 1. Bhasin S, Enzlin P, Coviello A, Basson R. Sexual dysfunction in men and women with endocrine disorders. Lancet. 2007;369(9561): 597-611. 2. Mercer CH, Fenton KA, Johnson AM, et al. Sexual function problems and help seeking behaviour in Britain: national probability sample survey. BMJ. 2003;327:426-427. 3. Kinsey AC, Pomeroy WB, Martin CE. Sexual Behavior in the Human Male. Philadelphia, PA: WB Saunders; 1948. 4. Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151:54-61. 5. Laumann EO, Paik A, Rosen RC. The epidemiology of erectile dysfunction: results from the National Health and Social Life Survey. Int J Impot Res. 1999;11(Suppl 1):S60-S64. 6. Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281:537-544. 7. Lewis RW, Fugl-Meyer KS, Bosch R, et al. Epidemiology/risk factors of sexual dysfunction. J Sex Med. 2004;1(1):35-39. CHAPTER 20 Sexual Dysfunction in Men and Women 8. Masters EH, Johnson V. Human Sexual Response. Boston, MA: Little, Brown; 1966. 9. Lue TF, Tanagho EA. Hemodynamics of erection. In: Tanagho EA, Lue TF, McClure RD, eds. Contemporary Management of Impotence and Infertility. Baltimore, MD: Williams & Wilkins; 1988:28-38. 10. Lue TF. Erectile dysfunction. N Engl J Med. 2000;342:1802-1813. 11. Bhasin S, Benson GS. Male sexual function. In: De Kretser D, ed. Knobil and Neill’s Physiology of Reproduction. 3rd ed. Boston, MA: Academic Press; 2006:1173-1194. 12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994. 13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, Text Revision. Washington, DC: American Psychiatric Association; 2000. 14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013. 15. Sungur MZ, Gündüz A. A comparison of DSM-IV-TR and DSM-5 definitions for sexual dysfunctions: critiques and challenges. J Sex Med. 2014;11(2):364-373. 16. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA. 1993;270:83-90. 17. The Process of Care Consensus Panel. The process of care model for evaluation and treatment of erectile dysfunction. Int J Impot Res. 1999;11:59-70, discussion 70-74. 18. Laumann EO, Nicolosi A, Glasser DB, et al. Sexual problems among women and men aged 40-80y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17:39-57. 19. Blumentals WA, Gome-Camninero A, Joo S, Bannappagari V. Should erectile dysfunction be considered as a marker for acute myocardial infarction? Results from a retrospective cohort study. Int J Impot Res. 2004;16:350-353. 20. Basson R, Schulz WW. Sexual sequelae of general medical disorders. Lancet. 2007;369:409-424. 21. Cyranowski JM, Bromberger J, Youk A, et al. Lifetime depression history and sexual function in women at midlife. Arch Sex Behav. 2004;33:539-548. 22. Hartmann U, Philippsohn S, Heiser K, Ruffer-Hesse C. Low sexual desire in midlife and older women: personality factors, psychosocial development, present sexuality. Menopause. 2004;11:726-740. 23. King M, Holt V, Nazareth I. Women’s view of their sexual difficulties: agreement and disagreement for the clinical diagnoses. Arch Sex Behav. 2007;36:281-288. 24. Basson R. Human sex response cycles. J Sex Marital Ther. 2001; 27(1):33-43. 25. Basson R. The female sexual response: a different model. J Sex Marital Ther. 2000;26:51-65. 26. Goldhammer DL, McCabe MP. A qualitative exploration of the meaning and experience of sexual desire among partnered women. Can J Human Sex. 2011;20(1–2):19-34. 27. Both S, Everaerd W, Laan E. Desire emerges from excitement: a psychophysiological perspective on sexual motivation. In: Janssen E, ed. The Psychophysiology of Sex. Bloomington, IN: Indiana University Press; 2007:327-339. 28. Laan E, Both S. What makes women experience desire? Feminine Psychol. 2008;18(4):505-514. 29. Balercia G, Boscaro M, Lombardo F, et al. Sexual symptoms in endocrine diseases: psychosomatic perspectives. Psychother Psychosom. 2007;76(3):134-140. 30. Enzlin P, Rosen R, Wiegel M, et al. Sexual dysfunction in women with type-1 diabetes: long-term findings from the DCCT/EDIC study cohort. Diabetes Care. 2009;32:780-783. 31. El-Sakka AI. Association of risk factors and medical comorbidities with male sexual dysfunctions. J Sex Med. 2007;4:1691-1700. 32. Vannier SA, O’Sullivan LF. Sex without desire: characteristics of occasions of sexual compliance in young adults’ committed relationships. J Sex Res. 2010;47:429-439. 33. Hayes R. Circular and linear modeling of female sexual desire and arousal. J Sex Res. 2011;48:130-141. 34. Janssen E, McBride KR, Yarber W, et al. Factors that influence sexual arousal in men: a focus group study. Arch Sex Behav. 2008;37: 252-265. 35. Brotto LA, Heiman JR, Tolman D. Narratives of desire in mid-age women with and without arousal difficulties. J Sex Res. 2009;16:1-12. 36. Mitchell KR, Wellings KA, Graham C. How do men and women define sexual desire and sexual arousal? J Sex Marital Ther. 2014;40(1):17-32. 37. Stoléru S, Fonteille V, Cornélis C, et al. Functional neuroimaging studies of sexual arousal and orgasm in healthy men and women: a review and meta-analysis. Neurosci Biobehav Rev. 2012;36:1481-1509. 38. Meston CM, Buss DM. Why humans have sex. Arch Sex Behav. 2007;36:477-507. 39. Carpenter LM, Nathanson CA, Kim JY. Physical women, emotional men: gender and sexual satisfaction in midlife. Arch Sex Behav. 2009;38:87-107. 821 40. Heiman JR, Long JS, Smith SN, et al. Sexual behaviour and relationship satisfaction in midlife and older couples in five countries. J Sex Med. 2009;6(Suppl 2):72. 41. de Jong DC. The role of attention in sexual arousal: implications for treatment of sexual dysfunction. J Sex Res. 2009;46(2–3):237-248. 42. Nobre PJ, Pinto-Gouveia J. Cognitions, emotions, and sexual response: analysis of the relationship among automatic thoughts, emotional responses, and sexual arousal. Arch Sex Behav. 2008;37:652-661. 43. Barlow DH. Causes of sexual dysfunction: the role of anxiety and cognitive interference. J Consult Clin Psychol. 1986;54:140-148. 44. Nelson AL, Purdon C. Non-erotic thoughts, attentional focus, and sexual problems in a community sample. Arch Sex Behav. 2011;40: 395-406. 45. Carvalho J, Vieira AL, Nobre P. Latent structures of male sexual functioning. J Sex Med. 2011;8:2501-2511. 46. Pfaus JG. Pathways of sexual desire. J Sex Med. 2009;6:1506-1533. 47. Bancroft J, Graham C, Janssen E, et al. The dual control model: current status and future directions. J Sex Res. 2009;46:121-142. 48. Takahashi H, Yahata N, Koeda M, et al. Brain activation associated with evaluative processes of guilt and embarrassment: an fMRI study. Neuroimage. 2004;23(3):967-974. 49. Archer JS, Love-Geffen TE, Herbst-Damm KL, et al. Effect of estradiol versus estradiol and testosterone on brain activation patterns in postmenopausal women. Menopause. 2006;13:528-537. 50. Georgiadis JR, Reinders AA, Paans AMJ, et al. Men versus women on sexual brain function: prominent differences during tactile genital stimulation, but not during orgasm. Hum Brain Mapp. 2009;30: 3089-3101. 51. Arnow BA, Millheiser L, Garrett A, et al. Women with hypoactive sexual desire disorder compared to normal females: a functional magnetic resonance imaging study. J Neurosci. 2009;158:484-502. 52. Bloemers J, Scholte S, van Rooij K, et al. Reduced gray matter volume and increased white matter fractional anisotropy in women with hypoactive sexual desire disorder. J Sex Med. 2014;11:753-767. 53. Seminowicz DA, Wideman TH, Naso L, et al. Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function. J Neurosci. 2011;31(20):7540-7550. 54. Redouté J, Stoléru S, Pugeat M, et al. Brain processing of visual sexual stimuli in treated and untreated hypogonadal patients. Psychoneuroendocrinology. 2005;30:461-482. 55. Berridge KC. Food reward: brain substrates of wanting and liking. Neurosci Biobehav Rev. 1996;20:1-25. 56. Miller B, Cummings J, McIntyre H, et al. Hypersexuality or altered sexual preference following brain injury. J Neurol Neurosurg Psychiatry. 1986;49:867-873. 57. Devinsky J, Sacks O, Devinsky O. Kluver-Bucy syndrome, hypersexuality, and the law. Neurocase. 2010;16(2):140-145. 58. Richfield E, Twyman R, Berent S. Neurological syndrome following bilateral damage to the head of the caudate nuclei. Ann Neurol. 1987;22:768-771. 59. Paredes RG, Agmo A. Has dopamine a physiological role in the control of sexual behavior? A critical review of the evidence. Prog Neurobiol. 2004;73:179-226. 60. Hull EM, Muschamp JW, Sato S. Dopamine and serotonin: influences on male sexual behavior. Physiol Behav. 2004;83:291-307. 61. Stahl SM. The psychopharmacology of sex: part 2. Effects of drugs and disease on the 3 phases of human sexual response. J Clin Psychiatry. 2001;62:147-148. 62. Bhasin S, Cunningham GR, Hayes FJ, et al; Task Force Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559. 63. Wierman ME, Basson R, Davis SR, et al. Androgen therapy in women: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2006;1:3697-3710. 64. Santoro N, Torrens J, Crawford S, et al. Correlates of circulating androgens in midlife women: the study of women’s health across the nation. J Clin Endocrinol Metab. 2005;90(8):4836-4845. 65. Davis SR, Davison SL, Donath S, Bell RJ. Circulating androgen levels in self-reported sexual function in women. JAMA. 2005;294:91-96. 66. Basson R, Brotto LA, Petkau J, Labrie F. Role of androgens in women’s sexual dysfunction. Menopause. 2010;17(5):962-971. 67. Labrie F, Bélanger A, Tusan L, et al. Marked decline in serum concentrations of adrenal C19 sex steroid precursors and conjugated androgen metabolites during aging. J Clin Endocrinol Metab. 1997;82: 2396-2402. 68. Stahl SM. The psychopharmacology of sex: part 1. Neurotransmitters and the 3 phases of the human sexual response. J Clin Psychiatry. 2001;62:80-81. 69. Halaris A. Neurochemical aspects of the sexual response cycle. CNS Spectr. 2003;8(3):211-216. 70. van Furth WR, Wolterink G, van Ree JM. Regulation of masculine sexual behavior: involvement of brain opioids and dopamine. Brain Res Brain Res Rev. 1995;21(2):162-184. 71. Chessick RD. The “pharmacogenic orgasm” in the drug addict. Arch Gen Psychiatry. 1960;3:565-566. 822 SECTION V Reproduction 72. Diamond LE, Earle DC, Rosen RC, et al. Double-blind, placebocontrolled evaluation of the safety, pharmacokinetic properties, and pharmacodynamic effects of intranasal PT-141, a melanocortin receptor agonist, in healthy males and patients with mild-to-moderate erectile dysfunction. Int J Impot Res. 2004;16:51-59. 73. Diamond LE, Earle DC, Heiman JR, et al. An effect of the subjective sexual response in premenopausal women with sexual arousal disorder by bremelanotide (PT-141), a melanocortin receptor agonist. J Sex Med. 2006;3:628-638. 74. Krüger TH, Hartmann U, Schedlowski M. Prolactinergic and dopaminergic mechanisms underlying sexual arousal and orgasm in humans. World J Urol. 2005;23:130-138. 75. Corona G, Mannucci E, Fisher AD, et al. Effect of hyperprolactinemia in male patients consulting for sexual dysfunction. J Sex Med. 2007;4: 1485-1493. 76. Kadioglu P, Yalin AS, Tiryakioglu O, et al. Sexual dysfunction in women with hyperprolactinemia: a pilot study report. J Urol. 2005; 174:1921-1925. 77. Blaustein JD. Progestin receptors: neuronal integrators of hormonal and environmental stimulation. Ann N Y Acad Sci. 2003;1007:238-250. 78. Pfaus JG, Kippin TE, Coria-Avila GA. What can animal models tell us about human sexual response? Ann Rev Sex Res. 2003;14:1-63. 79. Chivers ML, Seto MC, Lalumiere ML, et al. Agreement of self-reported and genital measures of sexual arousal in men and women: a metaanalysis. Arch Sex Behav. 2010;39(1):5-56. 80. Janssen E, Vorst H, Finn P, et al. The Sexual Inhibition (SIS) and Sexual Excitation (SES) Scales: II. Predicting psychophysiological response patterns. J Sex Res. 2002;39:127-132. 81. Janssen E, Goodrich D, Petrocelli J, et al. Psychophysiological response patterns and risky sexual behaviour in heterosexual and homosexual men. Arch Sex Behav. 2009;38:538-550. 82. Suschinsky KD, Lalumière ML. The relationship between sexual concordance and interoception in anxious and non-anxious women. J Sex Med. 2014;11:942-955. 83. Palace EM, Gorzalka BB. The enhancing effects of anxiety on arousal in sexually dysfunctional and functional women. J Abnorm Psychol. 1990;99(4):403-411. 84. Christ GJ. The penis as a vascular organ. The importance of corporal smooth muscle tone in the control of erection. Urol Clin North Am. 1995;22:727-745. 85. Benson GS, McConnell J, Lipshultz LI, et al. Neuromorphology and neuropharmacology of the human penis: an in vitro study. J Clin Invest. 1980;65:506-513. 86. Christ GJ. Gap junctions and ion channels: relevance to erectile dysfunction. Int J Impot Res. 2000;12(Suppl 4):S15-S25. 87. Zeng X, Keyser B, Li M, Sikka SC. T-type (alpha1G) low voltageactivated calcium channel interactions with nitric oxide-cyclic guanosine monophosphate pathway and regulation of calcium homeostasis in human cavernosal cells. J Sex Med. 2005;2:620-630, discussion 630-623. 88. Somlyo AP, Somlyo AV. Ca2+ sensitivity of smooth muscle and nonmuscle myosin II: modulated by G proteins, kinases, and myosin phosphatase. Physiol Rev. 2003;83:1325-1358. 89. O-Uchi J, Komukai K, Kusakari Y, et al. Alpha1-adrenoceptor stimulation potentiates L-type Ca2+ current through Ca2+/calmodulindependent PK II (CaMKII) activation in rat ventricular myocytes. Proc Natl Acad Sci U S A. 2005;102:9400-9405. 90. Krall JF, Fittingoff M, Rajfer J. Characterization of cyclic nucleotide and inositol 1,4,5-trisphosphate-sensitive calcium-exchange activity of smooth muscle cells cultured from the human corpora cavernosa. Biol Reprod. 1988;39:913-922. 91. Fittingoff M, Krall JF. Changes in inositol polyphosphate-sensitive calcium exchange in aortic smooth muscle cells in vitro. J Cell Physiol. 1988;134:297-301. 92. Hewawasam P, Fan W, Ding M, et al. 4-Aryl-3-(hydroxyalkyl)quinolin2-ones: novel maxi-K channel opening relaxants of corporal smooth muscle targeted for erectile dysfunction. J Med Chem. 2003;46: 2819-2822. 93. Christ GJ, Day N, Santizo C, et al. Intracorporal injection of hSlo cDNA restores erectile capacity in STZ-diabetic F-344 rats in vivo. Am J Physiol Heart Circ Physiol. 2004;287(4):H1544-H1553. 94. Naylor AM. Endogenous neurotransmitters mediating penile erection. Br J Urol. 1998;81:424-431. 95. Melman A, Bar-Chama N, McCullough A, et al. The first human trial for gene transfer therapy for the treatment of erectile dysfunction: preliminary results. Eur Urol. 2005;48:314-318. 96. Christ GJ, Moreno AP, Melman A, Spray DC. Gap junction-mediated intercellular diffusion of Ca2+ in cultured human corporal smooth muscle cells. Am J Physiol. 1992;263:C373-C383. 97. Ignarro LJ, Bush PA, Buga GM, et al. Nitric oxide and cyclic GMP formation upon electrical field stimulation cause relaxation of corpus cavernosum smooth muscle. Biochem Biophys Res Commun. 1990;170: 843-850. 98. Mills TM, Chitaley K, Lewis RW, Webb RC. Nitric oxide inhibits RhoA/ Rho-kinase signaling to cause penile erection. Eur J Pharmacol. 2002; 439:173-174. 99. Haning H, Niewohner U, Bischoff E. Phosphodiesterase type 5 (PDE5) inhibitors. Prog Med Chem. 2003;41:249-306. 100. Wallis RM, Corbin JD, Francis SH, Ellis P. Tissue distribution of phosphodiesterase families and the effects of sildenafil on tissue cyclic nucleotides, platelet function, and the contractile responses of trabeculae carneae and aortic rings in vitro. Am J Cardiol. 1999;83: 3C-12C. 101. Bischoff E. Potency, selectivity, and consequences of nonselectivity of PDE inhibition. Int J Impot Res. 2004;16(Suppl 1):S11-S14. 102. Boolell M, Allen MJ, Ballard SA, et al. Sildenafil: an orally active type 5 cyclic GMP-specific phosphodiesterase inhibitor for the treatment of penile erectile dysfunction. Int J Impot Res. 1996;8:47-52. 103. Taher A, Meyer M, Stief CG, et al. Cyclic nucleotide phosphodiesterase in human cavernous smooth muscle. World J Urol. 1997;15: 32-35. 104. Jeremy JY, Ballard SA, Naylor AM, et al. Effects of sildenafil, a type-5 cGMP phosphodiesterase inhibitor, and papaverine on cyclic GMP and cyclic AMP levels in the rabbit corpus cavernosum in vitro. Br J Urol. 1997;79:958-963. 105. Stief CG, Uckert S, Becker AJ, et al. The effect of the specific phosphodiesterase (PDE) inhibitors on human and rabbit cavernous tissue in vitro and in vivo. J Urol. 1998;159:1390-1393. 106. Carter AJ, Ballard SA, Naylor AM. Effect of the selective phosphodiesterase type 5 inhibitor sildenafil on erectile dysfunction in the anesthetized dog. J Urol. 1998;160:242-246. 107. Gong MC, Iizuka K, Nixon G, et al. Role of guanine nucleotidebinding proteins—ras-family or trimeric proteins or both—in Ca2+ sensitization of smooth muscle. Proc Natl Acad Sci U S A. 1996;93: 1340-1345. 108. Chikumi H, Fukuhara S, Gutkind JS. Regulation of G protein-linked guanine nucleotide exchange factors for Rho, PDZ-RhoGEF, and LARG by tyrosine phosphorylation: evidence of a role for focal adhesion kinase. J Biol Chem. 2002;277:12463-12473. 109. Gong MC, Fujihara H, Somlyo AV, Somlyo AP. Translocation of rhoA associated with Ca2+ sensitization of smooth muscle. J Biol Chem. 1997;272:10704-10709. 110. Segraves RT. Bupropion sustained-release for the treatment of hypoactive sexual desire disorder in premenopausal women. J Clin Psychopharmacol. 2004;24:339-342. 111. Jin L, Liu T, Lagoda GA, et al. Elevated RhoA/Rho-kinase activity in the aged rat penis: mechanism for age-associated erectile dysfunction. FASEB J. 2006;20:536-538. 112. Davis SR, Nijland FA, Weijmar-Schultz W. Tibolone vs transdermal continuous combined estrogen plus progestin in the treatment of female sexual dysfunction in naturally menopausal women: Results from the NETA trial. Maturitas. 2006;554S:S1-S112. 113. Lipshultz LI, McConnell J, Benson GS. Current concepts of the mechanisms of ejaculation. Normal and abnormal states. J Reprod Med. 1981; 26:499-507. 114. McMahon CG, Abdo C, Incrocci L, et al. Disorders of orgasm and ejaculation in men. J Sex Med. 2004;1:58-65. 115. Gil-Vernet JM Jr, Alvarez-Vijande R, Gil-Vernet A, Gil-Vernet JM. Ejaculation in men: a dynamic endorectal ultrasonographical study. Br J Urol. 1994;73:442-448. 116. Caruso S, Rugolo S, Agmello C, et al. Sildenafil improves sexual functioning in premenopausal women with type 1 diabetes who are affected by sexual arousal disorder: A double-blind, crossover, placebocontrolled pilot study. Fertil Steril. 2006;85:1496-1501. 117. Guiliano P, Clement P. Serotonin and premature ejaculation: from physiology to patient management. Euro Urol. 2006;50:454-466. 118. Waldinger M. The neurobiological approach to early ejaculation. J Urol. 2002;168:2359-2366. 119. Olivier B, Van Oorschot R, Waldinger M. Serotonin, serotonergic receptors, selective serotonin reuptake inhibitors and sexual behavior. Int Clin Psychopharmacol. 1998;13(Suppl 6):9. 120. Waldinger MD, Olivier B. Utility of selective serotonin reuptake inhibitors in premature ejaculation. Curr Opin Investig Drugs. 2004;5: 743-747. 121. Kwan M, Greenleaf WJ, Mann J, et al. The nature of androgen action on male sexuality: a combined laboratory-self-report study on hypogonadal men. J Clin Endocrinol Metab. 1983;57:557-562. 122. Alexander GM, Sherwin BB. The association between testosterone, sexual arousal, and selective attention for erotic stimuli in men. Horm Behav. 1991;25:367-381. 123. Alexander GM, Swerdloff RS, Wang C, et al. Androgen-behavior correlations in hypogonadal men and eugonadal men. I. Mood and response to auditory sexual stimuli. Horm Behav. 1997;31(2):110-119. 124. Arver S, Dobs AS, Meikle AW, et al. Improvement of sexual function in testosterone deficient men treated for 1 year with a permeation enhanced testosterone transdermal system. J Urol. 1996;155:16041608. 125. King BE, Packard MG, Alexander GM. Affective properties of intramedial preoptic area injections of testosterone in male rats. Neurosci Lett. 1999;269:149-152. 126. Bagatell CJ, Heiman JR, Rivier JE, Bremner WJ. Effects of endogenous testosterone and estradiol on sexual behavior in normal young men CHAPTER 20 Sexual Dysfunction in Men and Women 127. 128. 129. 130. 131. 132. 133. 134. 135. 136. 137. 138. 139. 140. 141. 142. 143. 144. 145. 146. 147. 148. 149. 150. 151. 152. [published erratum appears in J Clin Endocrinol Metab. 1994;78(6):1520]. J Clin Endocrinol Metab. 1994;78(3):711-716. Carani C, Bancroft J, Granata A, et al. Testosterone and erectile function, nocturnal penile tumescence and rigidity, and erectile response to visual erotic stimuli in hypogonadal and eugonadal men. Psychoneuroendocrinology. 1992;17:647-654. Cunningham GR, Hirshkowitz M, Korenman SG, Karacan I. Testosterone replacement therapy and sleep-related erections in hypogonadal men. J Clin Endocrinol Metab. 1990;70(3):792-797. Mills TM, Lewis RW, Stopper VS. Androgenic maintenance of inflow and veno-occlusion during erection in the rat. Biol Reprod. 1998;59(6): 1413-1418. Reilly CM, Zamorano P, Stopper VS, Mills TM. Androgenic regulation of NO availability in rat penile erection. J Androl. 1997;18(2):110115. Lugg JA, Rajfer J, Gonzalez-Cadavid NF. Dihydrotestosterone is the active androgen in the maintenance of nitric oxide-mediated penile erection in the rat. Endocrinology. 1995;136:1495-1501. Shabsigh R. The effects of testosterone on the cavernous tissue and erectile function. World J Urol. 1997;15:21-26. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:19952010. Jain P, Rademaker AW, McVary KT. Testosterone supplementation for erectile dysfunction: results of a meta-analysis. J Urol. 2000;164: 371-375. Buena F, Swerdloff RS, Steiner BS, et al. Sexual function does not change when serum testosterone levels are pharmacologically varied within the normal male range. Fertil Steril. 1993;59:1118-1123. Isidori AM, Giannetta E, Gianfrilli D, et al. Effects of testosterone on sexual function in men: results of a meta-analysis. Clin Endocrinol (Oxf). 2005;63(4):381-394. Bhasin S, Travison TG, Storer TW, et al. Effect of testosterone supplementation with and without a dual 5α-reductase inhibitor on fat-free mass in men with suppressed testosterone production: a randomized controlled trial. JAMA. 2012;307(9):931-939. Carani C, Rochira V, Faustini-Fustini M, et al. Role of oestrogen in male sexual behaviour: insights from the natural model of aromatase deficiency. Clin Endocrinol (Oxf). 1999;51(4):517-524. Carani C, Granata AR, Rochira V, et al. Sex steroids and sexual desire in a man with a novel mutation of aromatase gene and hypogonadism. Psychoneuroendocrinology. 2005;30(5):413-417. Finkelstein JS, Lee H, Burnett-Bowie SA, et al. Gonadal steroids and body composition, strength, and sexual function in men. N Engl J Med. 2013;369(11):1011-1022. Korenman SG, Morley JE, Mooradian AD, et al. Secondary hypogonadism in older men: its relation to impotence. J Clin Endocrinol Metab. 1990;71:963-969. Corona G, Isidori AM, Buvat J, et al. Testosterone supplementation and sexual function: a meta-analysis study. J Sex Med. 2014;11(6): 1577-1592. Kohler TS, Kim J, Feia K, et al. Prevalence of androgen deficiency in men with erectile dysfunction. Urology. 2008;71(4):693-697. Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172:658-663. Aversa A, Isidori AM, Spera G, et al. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin Endocrinol (Oxf). 2003;58(5):632-638. Dasgupta R, Wiseman OJ, Kanabar G, et al. Efficacy of sildenafil in the treatment of female sexual dysfunction due to multiple sclerosis. J Urol. 2004;171:1189-1193. Kalinchenko SY, Kozlov GI, Gontcharov NP, Katsiya GV. Oral testosterone undecanoate reverses erectile dysfunction associated with diabetes mellitus in patients failing on sildenafil citrate therapy alone. Aging Male. 2003;6:94-99. Spitzer M, Basaria S, Travison TG, et al. Effect of testosterone replacement on response to sildenafil citrate in men with erectile dysfunction: a parallel, randomized trial. Ann Intern Med. 2012;157(10): 681-691. Buvat J, Montorsi F, Maggi M, et al. Hypogonadal men nonresponders to the PDE5 inhibitor tadalafil benefit from normalization of testosterone levels with a 1% hydroalcoholic testosterone gel in the treatment of erectile dysfunction (TADTEST study). J Sex Med. 2011;8(1): 284-293. Spitzer M, Bhasin S, Travison TG, et al. Sildenafil increases serum testosterone levels by a direct action on the testes. Andrology. 2013; 1(6):913-918. Buisson O, Jannini A. Pilot echographic study of the differences in clitoral involvement following clitoral or vaginal sexual stimulation. J Sex Med. 2013;10:2734-2740. Oakley SH, Vaccaro CM, Crisp CC, et al. Clitoral size and location in relation to sexual function using pelvic MRI. J Sex Med. 2014;11(4): 1013-1022. 823 153. Samimi D, Allam A, Devereaux R, et al. Advantages of nerve-sparing intrastromal total abdominal hysterectomy. Int J Womens Health. 2013;5:37-42. 154. Bekker MD, Hogewoning CR, Wallner C, et al. The somatic and autonomic innervation of the clitoris; preliminary evidence of sexual dysfunction after minimally invasive slings. J Sex Med. 2012;9:1566-1578. 155. Salonia A, Giraldi A, Chivers ML, et al. Physiology of women’s sexual function: basic knowledge and new findings. J Sex Med. 2010;7: 2637-2660. 156. Uckert S, Albrecht K, Kuczyk MA, et al. Phosphodiesterase type 1, calcitonin gene-related peptide and vasoactive intestinal polypeptide are involved in the control of human vaginal arterial vessels. Eur J Obstet Gynecol Reprod Biol. 2013;169(2):283-286. 157. Shih C, Cold CJ, Yang CC. Cutaneous corpuscular receptors of the human glans clitoris: descriptive characteristics and comparison with the glans penis. J Sex Med. 2013;10:1783-1789. 158. van Netten JJ, Georgiadis JR, Nieuwenburg A, et al. 8-13 Hz fluctuations in rectal pressure are an objective marker of clitorally-induced orgasm in women. Arch Sex Behav. 2008;37:279-285. 159. Hamann S, Herman RA, Nolan CL, et al. Men and women differ in amygdala response to visual sexual stimuli. Nat Neurosci. 2004;7(4): 411-416. 160. Georgiadis JR, Kringelbach ML. The human sexual response cycle: brain imaging evidence linking sex to other pleasures. Prog Neurobiol. 2012;98(1):49-81. 161. Huynh HK, Willemsen ATM, Lovick TA, et al. Pontine control of ejaculation and female orgasm. J Sex Med. 2013;10:3038-3048. 162. Huynh HK, Willemsen AT, Holstege G. Female orgasm but not male ejaculation activates the pituitary. A PET-neuro-imaging study. Neuroimage. 2013;76:178-182. 163. Beck JG. Hypoactive sexual desire disorder: an overview. J Consult Clin Psychol. 1995;63:919-927. 164. Rosen RC, Leiblum SR. Hypoactive sexual desire. Psychiatr Clin North Am. 1995;18:107-121. 165. Segraves KB, Segraves RT. Hypoactive sexual desire disorder: prevalence and comorbidity in 906 subjects. J Sex Marital Ther. 1991;17: 55-58. 166. LoPiccolo J. Diagnosis and treatment of male sexual dysfunction. J Sex Marital Ther. 1985;11:215-232. 167. Panser LA, Rhodes T, Girman CJ, et al. Sexual function of men ages 40 to 79 years: the Olmsted County Study of Urinary Symptoms and Health Status Among Men. J Am Geriatr Soc. 1995;43(10):11071111. 168. Chevret M, Jaudinot E, Sullivan K, et al. Impact of erectile dysfunction (ED) on sexual life of female partners: assessment with the Index of Sexual Life (ISL) questionnaire. J Sex Marital Ther. 2004;30:157-172. 169. Johannes CB, Araujo AB, Feldman HA, et al. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol. 2000;163:460-463. 170. Benet AE, Melman A. The epidemiology of erectile dysfunction. Urol Clin North Am. 1995;22:699-709. 171. Braun M, Wassmer G, Klotz T, et al. Epidemiology of erectile dysfunction: results of the “Cologne Male Survey.” Int J Impot Res. 2000;12: 305-311. 172. McKinlay JB, Digruttolo L, Glasser D, et al. International differences in the epidemiology of male erectile dysfunction. Int J Clin Pract Suppl. 1999;102:35. 173. McKinlay JB. The worldwide prevalence and epidemiology of erectile dysfunction. Int J Impot Res. 2000;12(Suppl 4):S6-S11. 174. Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999;84:50-56. 175. Selvin E, Burnett AL, Platz EA. Prevalence and risk factors for erectile dysfunction in the US. Am J Med. 2007;120(2):151-157. 176. Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trial. Eur Heart J. 2006;27(22):2632-2639. 177. Thompson IM, Tangen CM, Goodman PJ, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294(23):29963002. 178. Araujo AB, Travison TG, Ganz P, et al. Erectile dysfunction and mortality. J Sex Med. 2009;6(9):2445-2454. 179. Araujo AB, Hall SA, Ganz P, et al. Does erectile dysfunction contribute to cardiovascular disease risk prediction beyond the Framingham risk score? J Am Coll Cardiol. 2010;55(4):350-356. 180. Schouten BW, Bohnen AM, Bosch JL, et al. Erectile dysfunction prospectively associated with cardiovascular disease in the Dutch general population: results from the Krimpen Study. Int J Impot Res. 2008; 20(1):92-99. 181. Jackson G, Boon N, Eardley I, et al. Erectile dysfunction and coronary artery disease prediction: evidence-based guidance and consensus. Int J Clin Pract. 2007;61(12):2019-2025. 182. Hodges LD, Kirby M, Solanki J, O’Donnell J. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2010;64(7):848-857. 824 SECTION V Reproduction 183. Feldman HA, Johannes CB, Derby CA, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging study. Prev Med. 2000;30:328-338. 184. Derby CA, Mohr BA, Goldstein I, et al. Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology. 2000; 56:302-306. 185. Rosen R, Altwein J, Boyle P, et al. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol. 2003;44:637-649. 186. Braun MH, Sommer F, Haupt G, et al. Lower urinary tract symptoms and erectile dysfunction: co-morbidity or typical “aging male” symptoms? Results of the “Cologne Male Survey.” Eur Urol. 2003;44: 588-594. 187. Barqawi A, O’Donnell C, Kumar R, et al. Correlation between LUTS (AUA-SS) and erectile dysfunction (SHIM) in an age-matched racially diverse male population: data from the Prostate Cancer Awareness Week (PCAW). Int J Impot Res. 2005;17:370-374. 188. Glina S, Santana AW, Azank F, et al. Lower urinary tract symptoms and erectile dysfunction are highly prevalent in ageing men. BJU Int. 2006;97:763-765. 189. McVary K. Lower urinary tract symptoms and sexual dysfunction: epidemiology and pathophysiology. BJU Int. 2006;97(Suppl 2):23-28, discussion 44-45. 190. Paick SH, Meehan A, Lee M, et al. The relationship among lower urinary tract symptoms, prostate specific antigen and erectile dysfunction in men with benign prostatic hyperplasia: results from the PROSCAR long-term efficacy and safety study. J Urol. 2005;173: 903-907. 191. McVary KT. Interrelation of erectile dysfunction and lower urinary tract symptoms. Drugs Today (Barc). 2005;41:527-536. 192. Christ GJ, Hodges S. Molecular mechanisms of detrusor and corporal myocyte contraction: identifying targets for pharmacotherapy of bladder and erectile dysfunction. Br J Pharmacol. 2006;147(Suppl 2): S41-S55. 193. Carson CC. Combination of phosphodiesterase-5 inhibitors and alpha-blockers in patients with benign prostatic hyperplasia: treatments of lower urinary tract symptoms, erectile dysfunction, or both? BJU Int. 2006;97(Suppl 2):39-43, discussion 44-45. 194. Liguori G, Trombetta C, De Giorgi G, et al. Efficacy and safety of combined oral therapy with tadalafil and alfuzosin: an integrated approach to the management of patients with lower urinary tract symptoms and erectile dysfunction. Preliminary report. J Sex Med. 2009;6(2):544-545. 195. Kaplan SA, Gonzalez RR, Te AE. Combination of alfuzosin and sildenafil is superior to monotherapy in treating lower urinary tract symptoms and erectile dysfunction. Eur Urol. 2007;51(6):1717-1723. 196. Buvat J, Glasser D, Neves RC, et al. Global Study of Sexual Attitudes and Behaviours (GSSAB) Investigators’ Group. Sexual problems and associated help-seeking behavior patterns: results of a populationbased survey in France. Int J Urol. 2009;16(7):632-638. 197. Laumann EO, Glasser DB, Neves RC, Moreira ED Jr. Global Study of Sexual Attitudes and Behaviours Investigators’ Group. A populationbased survey of sexual activity, sexual problems and associated helpseeking behavior patterns in mature adults in the United States of America. Int J Impot Res. 2009;21(3):171-178. 198. Porst H, Montorsi F, Rosen R, et al. The premature ejaculation prevalence and attitudes (PEPA) survey: prevalence, comorbidities, and professional help-seeking. Eur Urol. 2007;51:816-824. 199. Brotto L. The DSM diagnostic criteria for hypoactive sexual desire disorder in women. Arch Sex Behav. 2010;39:221-239. 200. Graham C. The DSM diagnostic criteria for female sexual arousal disorder. Arch Sex Behav. 2010;39:240-255. 201. Carvalho J. Sexual desire in women: an integrative approach regarding psychological, medical, and relationship dimensions. J Sex Med. 2010; 7:1807-1815. 202. Althof SE, Dean J, Derogates LR, et al. Current perspectives on the aclinical assessment and diagnosis of female sexual dysfunction and clinical studies of potential therapies: a statement of concern. J Sex Med. 2005;2:146-153. 203. Sidi H, Naing L, Midin M, Nik Jaafar NR. The female sexual response cycle: do Malaysian women conform to the circular model? J Sex Med. 2008;5:2359-2366. 204. Basson R. Women’s sexual desire and arousal disorders. Prim Psychiatry. 2008;15:72-81. 205. van Lankveld JJ, Granot M, Weijmar Schultz WC, et al. Women’s sexual pain disorders. J Sex Med. 2010;7(1 Pt 2):615-631. 206. Basson R, Leiblum S, Brotto L, et al. Definitions of women’s sexual dysfunctions reconsidered: advocating expansion and revision. J Psychosom Obstet Gynaecol. 2003;24:221-229. 207. Bancroft J, Loftus J, Long JS. Distress about sex: a national survey of women in heterosexual relationships. Arch Sex Behav. 2003;32: 193-208. 208. Tiefer L, Hall M, Tavris C. Beyond dysfunction: a new view of women’s sexual problems. J Sex Marital Ther. 2002;28(Suppl 1):225-232. 209. DeLamater JD, Sill M. Sexual desire in later life. J Sex Res. 2005; 42:138-149. 210. Lindau ST, Schumm LP, Laumann EO, et al. The study of sexuality and health among older adults in the United States. N Engl J Med. 2007; 357:762-774. 211. Öberg K, Sjögern Fugl-Myer K. On Swedish women’s distressing sexual dysfunctions: some concomitant conditions and life satisfaction. J Sex Med. 2005;2:169-180. 212. Valadares ALR, Pinto Neto AM, Osis MJD, et al. Dyspareunia: a population based study with Brazilian women between 40 and 65 years old. Menopause. 2006;13:P-98-P-1016. 213. Mishra G, Kuh D. Sexual functioning throughout menopause: the perceptions of women in a British cohort. Menopause. 2006;13: 880-890. 214. Levine KB, Williams RE, Hartmann KE. Vulvovaginal atrophy is strongly associated with female sexual dysfunction among sexually active postmenopausal women. Menopause. 2008;15:661-666. 215. Zitzmann M, Faber S, Nieschlag E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J Clin Endocrinol Metab. 2006;91(11):4335-4343. 216. Wu FC, Tajar A, Beynon JM, et al; EMAS Group. Identification of lateonset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363(2):123-135. 217. Kelleher S, Conway AJ, Handelsman DJ. Blood testosterone threshold for androgen deficiency symptoms. J Clin Endocrinol Metab. 2004; 89(8):3813-3817. 218. El-Sakka AI, Tayeb KA. Peyronie’s disease in diabetic patients being screened for erectile dysfunction. J Urol. 2005;174(3):1026-1030. 219. Corona G, Mannucci E, Mansani R, et al. Organic, relational and psychological factors in erectile dysfunction in men with diabetes mellitus. Eur Urol. 2004;46(2):222-228. 220. De Berardis G, Pellegrini F, Franciosi M, et al. QuED (Quality of Care and Outcomes in Type 2 Diabetes) Study Group. Longitudinal assessment of quality of life in patients with type 2 diabetes and selfreported erectile dysfunction. Diabetes Care. 2005;28(11):2637-2643. 221. Klein R, Klein BE, Moss SE. Ten-year incidence of self-reported erectile dysfunction in people with long-term type 1 diabetes. J Diabetes Complications. 2005;19(1):35-41. 222. Rhoden EL, Ribeiro EP, Riedner CE, et al. Glycosylated haemoglobin levels and the severity of erectile function in diabetic men. BJU Int. 2005;95(4):615-617. 223. Kalter-Leibovici O, Wainstein J, Ziv A, et al. Israel Diabetes Research Group (IDRG) Investigators. Clinical, socioeconomic, and lifestyle parameters associated with erectile dysfunction among diabetic men. Diabetes Care. 2005;28(7):1739-1744. 224. Xin Z, Yuan SY, Wang ZP, et al. Influencing factors of erectile function in male patients with type 2 diabetes mellitus. Zhongguo Linchyuang Kangfu. 2004;8(21):4136-4137. 225. Zheng H, Fan W, Li G, Tam T. Predictors for erectile dysfunction among diabetics. Diabetes Res Clin Pract. 2006;71:313-319. 226. Ding EL, Song Y, Malik VS, Liu S. Sex differences of endogenous sex hormones and risks of type 2 diabetes: a systematic review and metaanalysis. JAMA. 2006;295:1288-1299. 227. Yeap BB, Chubb SA, Hyde Z, et al. Lower serum testosterone is independently associated with insulin resistance in non-diabetic older men: the Health in Men Study. Eur J Endocrinol. 2009;161(4): 591-598. 228. Laaksonen DE, Niskanen L, Punnonen K, et al. Testosterone and sex hormone-binding globulin predict the metabolic syndrome and diabetes in middle-aged men. Diabetes Care. 2004;27(5):1036-1041. 229. Dhindsa S, Prabhakar S, Sethi M, et al. Frequent occurrence of hypogonadotropic hypogonadism in type 2 diabetes. J Clin Endocrinol Metab. 2004;89(11):5462-5468. 230. Lakshman KM, Bhasin S, Araujo AB. Sex hormone-binding globulin as an independent predictor of incident type 2 diabetes mellitus in men. J Gerontol A Biol Sci Med Sci. 2010;65(5):503-509. 231. Bhasin S, Jasjua GK, Pencina M, et al. Sex hormone-binding globulin, but not testosterone, is associated prospectively and independently with incident metabolic syndrome in men: the Framingham Heart Study. Diabetes Care. 2011;34(11):2464-2470. 232. Gazzaruso C, Giordanetti S, De Amici E, et al. Relationship between erectile dysfunction and silent myocardial ischemia in apparently uncomplicated type 2 diabetic patients. Circulation. 2004;110(1): 22-26. 233. Basu A, Ryder RE. New treatment options for erectile dysfunction in patients with diabetes mellitus [review]. Drugs. 2004;64(23):26672688. 234. De Vriese AS, Verbeuren TJ, Van de Voorde J, et al. Endothelial dysfunction in diabetes. Br J Pharmacol. 2000;130:963-974. 235. Saenz de Tejada I, Angulo J, Cellek S, et al. Pathophysiology of erectile dysfunction. J Sex Med. 2005;2:26-39. 236. Seftel AD, Vasin ND, Ni Z, et al. Advanced glycation end products in human penis: elevation in diabetic tissue, site of deposition and possible effect through iNOS or eNOS. Urology. 1997;50:1016-1026. 237. Bivalacqua TJ, Champion HC, Usta MF, et al. RhoA/Rho-kinase suppresses endothelial nitric oxide synthase in the penis: a mechanism for diabetes-associated erectile dysfunction. Proc Natl Acad Sci U S A. 2004;101(24):9121-9126. CHAPTER 20 Sexual Dysfunction in Men and Women 238. Boulton AJM, Vinik AJ, Arezzo JC, et al. Diabetic neuropathies. A statement by the American Diabetes Association. Diabetes Care. 2005; 28(4):956-962. 239. Bivalacqua TJ, Hellstrom WJ, Kadowitz PJ, Champion HC. Increased expression of arginase II in human diabetic corpus cavernosum: in diabetic-associated erectile dysfunction. Biochem Biophys Res Commun. 2001;283(4):923-927. 240. El-Sakka AI, Lin CS, Chui RM, et al. Effects of diabetes on nitric oxide synthase and growth factor genes and protein expression in an animal model. Int J Impot Res. 1999;11(3):123-132. 241. Ellenberg M, Weber H. Retrograde ejaculation in diabetic neuropathy. Ann Intern Med. 1966;65(6):1237-1246. 242. Seftel AD, Rosen RC, Rosenberg MT, Sadovsky R. Benign prostatic hyperplasia evaluation, treatment and association with sexual dysfunction: practice patterns according to physician specialty. Int J Clin Pract. 2008;62(4):614-622. 243. Wilt TJ, Mac Donald R, Rutks I. Tamsulosin for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2003;(1):CD002081. 244. Edwards JE, Moore RA. Finasteride in the treatment of clinical benign prostatic hyperplasia: a systematic review of randomised trials. BMC Urol. 2002;2:14. 245. Giuliano F. Impact of medical treatments for benign prostatic hyperplasia on sexual function. BJU Int. 2006;97(Suppl 2):34-38, discussion 44-45. 246. Ganzer CA, Jacobs AR, Iqbal F. Persistent sexual, emotional, and cognitive impairment post-finasteride: a survey of men reporting symptoms. Am J Mens Health. 2015;9(3):222-228. 247. Irwig MS, Kolukula S. Persistent sexual side effects of finasteride for male pattern hair loss. J Sex Med. 2011;8(6):1747-1753. 248. Di Loreto C, La Marra F, Mazzon G, et al. Immunohistochemical evaluation of androgen receptor and nerve structure density in human prepuce from patients with persistent sexual side effects after finasteride use for androgenetic alopecia. PLoS ONE. 2014;9(6): e100237. 249. Traish AM, Hassani J, Guay AT, et al. Adverse side effects of 5α-reductase inhibitors therapy: persistent diminished libido and erectile dysfunction and depression in a subset of patients. J Sex Med. 2011;8(3): 872-884. 250. Cecchin E, De Mattia E, Mazzon G, et al. A pharmacogenetic survey of androgen receptor (CAG)n and (GGN)n polymorphisms in patients experiencing long term side effects after finasteride discontinuation. Int J Biol Markers. 2014;29(4):e310-e316. 251. Buvat J, Lemaire A. Endocrine screening in 1,022 men with erectile dysfunction: clinical significance and cost-effective strategy [see comments]. J Urol. 1997;158:1764-1767. 252. Citron JT, Ettinger B, Rubinoff H, et al. Prevalence of hypothalamicpituitary imaging abnormalities in impotent men with secondary hypogonadism. J Urol. 1996;155:529-533. 253. Carter JN, Tyson JE, Tolis G, et al. Prolactin-screening tumors and hypogonadism in 22 men. N Engl J Med. 1978;299(16):847-852. 254. Franks S, Jacobs HS, Martin N, Nabarro JD. Hyperprolactinaemia and impotence. Clin Endocrinol (Oxf). 1978;8(4):277-287. 255. Colao A, Vitale G, Cappabianca P, et al. Outcome of cabergoline treatment in men with prolactinoma: effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J Clin Endocrinol Metab. 2004;89:1704-1711. 256. Krassas GE, Tziomalos K, Papadopoulou F, et al. Erectile dysfunction in patients with hyper- and hypothyroidism: how common and should we treat? J Clin Endocrinol Metab. 2008;93(5):1815-1819. 257. Carani C, Isidori AM, Granata A, et al. Multicenter study on the prevalence of sexual symptoms in male hypo- and hyperthyroid patients. J Clin Endocrinol Metab. 2005;90:6472-6479. 258. Dumoulin SC, Perret BP, Bennet AP, Caron PJ. Opposite effects of thyroid hormones on binding proteins for steroid hormones (sex hormone-binding globulin and corticosteroid-binding globulin) in humans. Eur J Endocrinol. 1995;132(5):594-598. 259. Donnelly P, White C. Testicular dysfunction in men with primary hypothyroidism; reversal of hypogonadotrophic hypogonadism with replacement thyroxine. Clin Endocrinol (Oxf). 2000;52(2):197-201. 260. Veronelli A, Masu A, Ranieri R, et al. Prevalence of erectile dysfunction in thyroid disorders: comparison with control subjects and with obese and diabetic patients. Int J Impot Res. 2006;18:111-114. 261. Esposito K, Giugliano D. Obesity, the metabolic syndrome, and sexual dysfunction. Int J Impot Res. 2005;17(5):391-398. 262. Koca O, Calışkan S, Oztürk MI, et al. Vasculogenic erectile dysfunction and metabolic syndrome. J Sex Med. 2010;7(12):3997-4002. 263. Demir O, Akgul K, Akar Z, et al. Association between severity of lower urinary tract symptoms, erectile dysfunction and metabolic syndrome. Aging Male. 2009;12(1):29-34. 264. Demir T, Demir O, Kefi A, et al. Prevalence of erectile dysfunction in patients with metabolic syndrome. Int J Urol. 2006;13(4):385-388. 265. Oppo A, Franceschi E, Atzeni F, et al. Effects of hyperthyroidism, hypothyroidism, and thyroid autoimmunity on female sexual function. J Endocrinol Invest. 2011;34:449-453. 266. Atis G, Dalkilinc A, Altuntas Y, et al. Hyperthyroidism: a risk factor for female sexual dysfunction. J Sex Med. 2011;8(8):2327-2333. 825 267. Pasquali D, Maiorino MI, Renzullo A, et al. Female sexual dysfunction in women with thyroid disorders. J Endocrinol Inv. 2013;36(9):729-733. 268. Wierman M, Nappi R, Avis N, et al. Endocrine aspects of women’s sexual function. J Sex Med. 2010;7(1 Pt 2):561-585. 269. Esposito K, Maiorino MI, Bellastella G, et al. Determinants of female sexual dysfunction in type 2 diabetes. Int J Impot Res. 2010;22:179-184. 270. Maiorino MI, Bellastella G, Esposito K. Diabetes and sexual dysfunction: current perspectives. Diabetes Metab Syndr Obes. 2014;7:95-105. 271. Abu Ali RM, Al Hajeri RM, Khader YS, et al. Sexual dysfunction in Jordanian diabetic women. Diabetes Care. 2008;31:1580-1581. 272. Olarinoye J, Olarinoye A. Determinants of sexual function among women with type 2 diabetes in a Nigerian population. J Sex Med. 2008;5(4):878-886. 273. Wallner LP, Sarma AV, Kim C. Sexual functioning among women with and without diabetes in the Boston Area Community Health Study. J Sex Med. 2010;7:881-887. 274. Tagliabue M, Gottero C, Zuffranieri M, et al. Sexual function in women with type 1 diabetes matched with a control group: depressive and psychosocial aspects. J Sex Med. 2011;8:1694-1700. 275. Leedom L, Feldman M, Procci W, et al. Symptoms of sexual dysfunction and depression in diabetic women. J Diabetes Complications. 1991;5:38-41. 276. Ogbera AO, Chinenye S, Akinlade A, et al. Frequency and correlates of sexual dysfunction in women with diabetes mellitus. J Sex Med. 2009;6:3401-3406. 277. Jensen SB. Sexual dysfunction in younger insulin-treated diabetic females. A comparative study. Diabetes Metab. 1985;11:278-282. 278. Campbell LV, Redelman MJ, Borkman M, et al. Factors in sexual dysfunction in diabetic female volunteer subjects. Med J Aust. 1989; 151:550-552. 279. Salonia A, Lanzi R, Scavini M, et al. Sexual function and endocrine profile in fertile women with type 1 diabetes. Diabetes Care. 2006; 29:312-316. 280. Pontiroli AE, Cortelazzi D, Morabito A. Female sexual dysfunction and diabetes: a systematic review and meta-analysis. J Sex Med. 2013;10: 1044-1051. 281. Veronelli A, Mauri C, Zecchini B, et al. Sexual dysfunction is frequent in premenopausal women with diabetes, obesity, and hypothyroidism, and correlates with markers of increased cardiovascular risk. A preliminary report. J Sex Med. 2009;6:1561-1568. 282. Esposito K, Ciotola M, Giugliano F, et al. Association of body weight with sexual function in women. Int J Impot Res. 2007;19(4):353-357. 283. Castellini G, Mannucci E, Mazzei C, et al. Sexual function in obese women with and without binge eating disorder. J Sex Med. 2010;7(12): 3969-3978. 284. Esposito K, Ciotola M, Marfella R, et al. The metabolic syndrome: a cause of sexual dysfunction in women. Int J Impot Res. 2005;17: 224-226. 285. Martelli V, Valisella S, Moscatiello S, et al. Prevalence of sexual dysfunction among postmenopausal women with and without metabolic syndrome. J Sex Med. 2012;9(2):434-441. 286. Basson RJ, Rucker BM, Laird PG, et al. Sexuality of women with diabetes. J Sex Reprod Med. 2001;1(1):11-20. 287. Giraldi A, Persson K, Werkström V, et al. Effects of diabetes on neurotransmission in rat vaginal smooth muscle. Int J Impot Res. 2001;13: 58-66. 288. Caruso S, Rugolo S, Mirabella D, et al. Changes in clitoral blood flow in premenopausal women affected by type 1 diabetes after single 100-mg administration of sildenafil. Urology. 2006;68:161-165. 289. Ponholzer A, Temml C, Rauchenwald M, et al. Is the metabolic syndrome a risk factor for female sexual dysfunction in sexually active women? Int J Impot Res. 2008;20:100-104. 290. Kim YH, Kim SM, Kim JJ, et al. Does metabolic syndrome impair sxual function in middle to old-aged women? J Sex Med. 2011;8:112-1130. 291. Elsenbruch S, Hahn S, Kowalsky D, et al. Quality of life, psychosocial well-being, and sexual satisfaction in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2003;88:5801-5807. 292. Hahn S, Janssen OE, Tan S, et al. Clinical and psychological correlates of quality-of-life in polycystic ovary syndrome. Eur J Endocrinol. 2005; 153:853-860. 293. Janssen OE, Hahn S, Tan S, et al. Mood and sexual function in polycystic ovary syndrome. Semin Reprod Med. 2008;26:45-52. 294. Ferraresi SR, Lara LA, Reis RM, et al. Changes in sexual function in women with polycystic ovary syndrome: a pilot study. J Sex Med. 2013;10(2):467-473. 295. Ercan CM, Coksuer H, Aydogan U, et al. Sexual dysfunction assessment and hormonal correlations in patients with polycystic ovary syndrome. Int J Impot Res. 2013;25(4):127-132. 296. Dewailly D, Vantyghem-Haudiquet MC, Sainsard C, et al. Clinical and biological phenotypes in late-onset 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1986;63:418-423. 297. Lobo RA, Goebelsmann U. Adult manifestation of congenital adrenal hyperplasia due to incomplete 21-hydroxylase deficiency mimicking polycystic ovarian disease. Am J Obstet Gynecol. 1980;138:720-726. 298. Frisén L, Nordenström A, Falhammar H, et al. Gender role behavior, sexuality, and psychosocial adaptation in women with congenital 826 299. 300. 301. 302. 303. 304. 305. 306. 307. 308. 309. 310. 311. 312. 313. 314. 315. 316. 317. 318. 319. 320. 321. 322. 323. SECTION V Reproduction adrenal hyperplasia due to CYP21A2 deficiency. J Clin Endocrinol Metab. 2009;94:3432-3439. Hines M, Brook C, Conway GS. Androgen and psychosexual development: core gender identity, sexual orientation and recalled childhood gender role behavior in women and men with congenital adrenal hyperplasia (CAH). J Sex Res. 2004;41:75-81. Miller KK, Sesmilo G, Schiller A, et al. Androgen deficiency in women with hypopituitarism. J Clin Endocrinol Metab. 2001;86(2): 561-567. Wierman M, Arlt W, Basson R, et al. Androgen therapy in women: a reappraisal: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2014;99(10):3489-3510. Miller KK, Biller BM, Beauregard C, et al. Effects of testosterone replacement in androgen-deficient women with hypopituitarism: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab. 2006;91:1683-1690. Arlt W, Callies F, van Vlijmen JC, et al. Dehydroepiandrosterone replacement in women with adrenal insufficiency. N Engl J Med. 1999;341:1013-1020. Hunt PJ, Gurnell EM, Huppert FA, et al. Improvement in mood and fatigue after dehydroepiandrosterone replacement in Addison’s disease in a randomized, double blind trial. J Clin Endocrinol Metab. 2000;85: 4650-4656. Gurnell EM, Hunt PJ, Curran SE, et al. Long-term DHEA replacement in primary adrenal insufficiency: a randomized, controlled trial. J Clin Endocrinol Metab. 2008;93:400-409. Libè R, Barbetta L, Dall’Asta C, et al. Effects of dehydroepiandrosterone (DHEA) supplementation on hormonal, metabolic and behavioral status in patients with hypoadrenalism. J Endocrinol Invest. 2004;27: 736-741. Binder G, Weber S, Ehrismann M, et al. South German Working Group for Pediatric Endocrinology. Effects of dehydroepiandrosterone therapy on pubic hair growth and psychological well-being in adolescent girls and young women with central adrenal insufficiency: a double-blind, randomized, placebo-controlled phase III trial. J Clin Endocrinol Metab. 2009;94:1182-1190. Erichsen MM, Løvås K, Skinningsrud B, et al. Clinical, immunological, and genetic features of autoimmune primary adrenal insufficiency: observations from a Norwegian registry. J Clin Endocrinol Metab. 2009;94:4882-4890. Erichsen MM, Huseby ES, Michelsen TM, et al. Sexuality and fertility in women with Addison’s disease. J Clin Endocrinol Metab. 2010;95: 4354-4360. Løvås K, Husebye ES. Replacement therapy in Addison’s disease. Expert Opin Pharmacother. 2003;4:2145-2149. Van Thiel SW, Romijn JA, Pereira AM, et al. Effects of dehydroepiandrostenedione, superimposed on growth hormone substitution, on quality of life and insulin-like growth factor I in patients with secondary adrenal insufficiency: a randomized, placebo-controlled, cross-over trial. J Clin Endocrinol Metab. 2005;91:1683-1690. Alkatib AA, Cosma M, Elamin MB, et al. A systematic review and metaanalysis of randomized placebo-controlled trials of DHEA treatment effects on quality of life in women with adrenal insufficiency. J Clin Endocrinol Metab. 2009;94:3676-3681. Huang AJ, Moore EE, Boyko EJ, et al. Vaginal symptoms in post menopausal women: self-reported severity, natural history, and risk factors. Menopause. 2010;17:121-126. Santoro N, Komi J. Prevalence and impact of vaginal symptoms among postmenopausal women. J Sex Med. 2009;6:2133-2142. Indhavivadhana S, Leerasiri P, Rattanachaiyanont M, et al. Vaginal atrophy and sexual dysfunction in current users of systemic postmenopausal hormone therapy. J Med Assoc Thai. 2010;93(6):667-675. Labrie F, Bélanger A, Bélanger P, et al. Androgen glucuronides, instead of testosterone, as the new markers of androgenic activity in women. J Steroid Biochem. 2006;99:182-188. Woods NF, Mitchell ES, Tao Y, et al. Polymorphisms in the estrogen synthesis and metabolism pathways and symptoms during the menopausal transition: observations from the Seattle Midlife Women’s Health Study. Menopause. 2006;13:902-910. Kao A, Binik Y, Amsel R, et al. Biopsychosocial predictors of postmenopausal dyspareunia: the role of steroid hormones, vulvovaginal atrophy, cognitive-emotional factors and dyadic adjustment. J Sex Med. 2012;9:2057-2076. West SL, D’Aloisio AA, Agans RP, et al. Prevalence of low sexual desire and hypoactive sexual desire disorder in a nationally representative sample of US women. Arch Intern Med. 2008;168:1441-1449. Melcangi RC, Panzica GC. Neuroactive steroids: old players in a new game. Neuroscience. 2006;138:733-739. Ishunina TA, Swaab DF. Alterations in the human brain in menopause. Maturitas. 2007;57:20-22. Birnbaum GE, Cohen O, Wertheimer V. It is all about intimacy? Age, menopausal status, and women’s sexuality. Pers Relation. 2007;14: 167-185. Aziz A, Brannstrom M, Bergquist C, et al. Perimenopausal androgen decline after oophorectomy does not influence sexuality or psychological well-being. Fertil Steril. 2005;83:1021-1028. 324. Farquar CM, Harvey SA, Yu Y, et al. A prospective study of three years of outcomes after hysterectomy with and without oophorectomy. Obstet Gynecol. 2006;194:714-717. 325. Teplin V, Vittinghoff E, Lin F, et al. Oophorectomy in premenopausal women: health-related quality of life and sexual functioning. Obstet Gynecol. 2007;109:347-354. 326. Erekson EA, Martin DK, Zhu K, et al. Sexual function in older women after oophorectomy. Obstet Gynecol. 2012;120(4):833-842. 327. Finch A, Narod SA. Quality of life and health status after prophylactic salpingo-oophorectomy in women who carry a BRCA mutation: a review. Maturitas. 2011;70:261-265. 328. Fliegner M, Krupp K, Brunner F, et al. Sexual life and sexual wellness in individuals with complete androgen insensitivity syndrome (CAIS) and Mayer-Rokitansky-Küster-Hauser Syndrome (MRKHS). J Sex Med. 2014;11:729-742. 329. Erekson EA, Martin DK, Ratner ES. Oophorectomy: the debate between ovarian conservation and elective oophorectomy. Menopause. 2013;20: 110-114. 330. Labrie F. Intracrinology. Mol Cell Endocrinol. 1991;78:C113-C118. 331. Cui Y, Zong H, Yan H, et al. The efficacy and safety of ospemifene in treating dyspareunia associated with postmenopausal vulvar and vaginal atrophy: a systematic review and meta-analysis. J Sex Med. 2014;11:487-497. 332. Pastor Z, Holla K, Chmel R. The influence of combined oral contraceptives on female sexual desire: a systematic review. Eur J Contracept Reprod Health Care. 2013;18:27-43. 333. Wisniewski AB, Migeon CJ, Meyer-Bahlburg HFL, et al. Complete androgen insensitivity syndrome: long-term medical, surgical, and psychosexual outcome. J Clin Endocrinol Metab. 2000;85:2664-2669. 334. Minto CL, Liao KL, Conway GS, et al. Sexual function in women with complete androgen insensitivity syndrome. Fertil Steril. 2003;80: 157-164. 335. Hines M, Ahmed SF, Hughes IA. Psychological outcomes and genderrelated development in complete androgen insensitivity syndrome. Arch Sex Behav. 2003;32:93-101. 336. Köhler B, Kleinemeier E, Lux A, et al. Satisfaction with genital surgery and sexual life of adults with XY disorders of sex development: results from the German Clinical Evaluation Study. J Clin Endocrinol Metab. 2012;97:577-588. 337. Cappelleri JC, Rosen RC, Smith MD, et al. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology. 1999;54:346-351. 338. Lue TF, Giuliano F, Montorsi F, et al. Summary of recommendations on sexual dysfunctions in men. J Sex Med. 2004;1:6-23. 339. O’Leary MP, Fowler FJ, Lenderking WR, et al. A brief male sexual function inventory. Urology. 1995;46:697-706. 340. Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11:319-326. 341. Montague DK, Jarow JP, Broderick GA, et al. Erectile Dysfunction Guideline Update Panel. J Urol. 2005;174(1):230-239. 342. Lobo JR, Nehra A. Clinical evaluation of erectile dysfunction in the era of PDE-5 inhibitors. Urol Clin North Am. 2005;32(4):447-455. 343. Bhasin S, Pencina M, Jasuja GK, et al. Reference ranges for testosterone in men generated using liquid chromatography tandem mass spectrometry in a community-based sample of healthy nonobese young men in the Framingham Heart Study and applied to three geographically distinct cohorts. J Clin Endocrinol Metab. 2011;96(8): 2430-2439. 344. Rosner W, Vesper H. Endocrine Society; American Association for Clinical Chemistry; American Association of Clinical Endocrinologists; Androgen Excess/PCOS Society; American Society for Bone and Mineral Research; American Society for Reproductive Medicine; American Urological Association; Association of Public Health Laboratories; Endocrine Society; Laboratory Corporation of America; North American Menopause Society; Pediatric Endocrine Society. Toward excellence in testosterone testing: a consensus statement. J Clin Endocrinol Metab. 2010;95(10):4542-4548. 345. Vesper HW, Botelho JC. Standardization of testosterone measurements in humans. J Steroid Biochem Mol Biol. 2010;121(3–5):513-519. 346. Bhasin S, Zhang A, Coviello A, et al. The impact of assay quality and reference ranges on clinical decision making in the diagnosis of androgen disorders. Steroids. 2008;73(13):1311-1317. 347. Rosner W, Auchus RJ, Azziz R, et al. Position statement: utility, limitations, and pitfalls in measuring testosterone: an Endocrine Society position statement. J Clin Endocrinol Metab. 2007;92(2):405-413. 348. Zakharov MN, Bhasin S, Travison TG, et al. A multi-step, dynamic allosteric model of testosterone’s binding to sex hormone binding globulin. Mol Cell Endocrinol. 2015;399:190-200. 349. Wu FC, Tajar A, Pye SR, et al; European Male Aging Study Group. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study. J Clin Endocrinol Metab. 2008;93(7):2737-2745. 350. Harman SM, Metter EJ, Tobin JD, et al; Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free CHAPTER 20 Sexual Dysfunction in Men and Women 351. 352. 353. 354. 355. 356. 357. 358. 359. 360. 361. 362. 363. 364. 365. 366. 367. 368. 369. 370. 371. 372. 373. 374. 375. 376. testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. Clin Endocrinol Metab. 2001;86(2):724-731. Orwoll E, Lambert LC, Marshall LM, et al. Testosterone and estradiol among older men. J Clin Endocrinol Metab. 2006;91(4):1336-1344. Mueller SC, Wallenberg-Pachaly H, Voges GE, Schild HH. Comparison of selective internal iliac pharmaco-angiography, penile brachial index and duplex sonography with pulsed Doppler analysis for the evaluation of vasculogenic (arteriogenic) impotence. J Urol. 1990;143: 928-932. Brock G. Tumescence monitoring devices: past and present. In: Hellstrom WJ, ed. Handbook of Sexual Dysfunction. San Francisco, CA: The American Society of Andrology; 1999:65-69. Rosen RC. Assessment of female sexual dysfunction: review of validated methods. Fertil Steril. 2002;77(S4):s89-s93. Brotto LA. The Female Sexual Function Index. J Sex Marital Ther. 2009;35:161-163. Mitchell KR, Ploubidis GB, Datta J, et al. The Natsal-SF: a validated measure of sexual function for use in community surveys. Eur J Epidemiol. 2012;27:409-418. Dundon CM, Rellini AH. More than sexual function: predictors of sexual satisfaction in a sample of women aged 40-70. J Sex Med. 2010; 7:896-904. Stephenson KR, Ahrold TK, Meston CM. The association between sexual motives and sexual satisfaction: gender differences and categorical comparisons. Arch Sex Behav. 2011;40:607-618. Steidle C, Schwartz S, Jacoby K, et al; North American AA2500 T Gel Study Group. AA2500 testosterone gel normalizes androgen levels in aging males with improvements in body composition and sexual function. J Clin Endocrinol Metab. 2003;88(6):2673-2681. Wang C, Swerdloff RS, Iranmanesh A, et al; Testosterone Gel Study Group. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. J Clin Endocrinol Metab. 2000;85(8):2839-2853. Wang C, Cunningham G, Dobs A, et al. Long-term testosterone gel (AndroGel) treatment maintains beneficial effects on sexual function and mood, lean and fat mass, and bone mineral density in hypogonadal men. J Clin Endocrinol Metab. 2004;89(5):2085-2098. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82(1):20-28. Snyder PJ, Ellenberg SS, Cunningham GR, et al. The Testosterone Trials: seven coordinated trials of testosterone treatment in elderly men. Clin Trials. 2014;11(3):362-375. Rosen RC. Psychogenic erectile dysfunction. Classification and management. Urol Clin North Am. 2001;28:269-278. Abrahamson DJ, Barlow DH, Beck JG, et al. The effects of attentional focus and partner responsiveness on sexual responding: replication and extension. Arch Sex Behav. 1985;14:361-371. Kilmann PR, Boland JP, Norton SP, et al. Perspectives of sex therapy outcome: a survey of AASECT providers. J Sex Marital Ther. 1986;12: 116-138. Melnik T, Soares BG, Nasselo AG. Psychosocial interventions for erectile dysfunction. Cochrane Database Syst Rev. 2007;(3):CD004825. Melnik T, Soares BG, Nasello AG. The effectiveness of psychological interventions for the treatment of erectile dysfunction: systematic review and meta-analysis, including comparisons to sildenafil treatment, intracavernosal injection, and vacuum devices. J Sex Med. 2008; 5(11):2562-2574. Schmidt HM, Munder T, Gerger H, et al. Combination of psychological intervention and phosphodiesterase-5 inhibitors for erectile dysfunction: a narrative review and meta-analysis. J Sex Med. 2014;11(6): 1376-1391. Hatzimouratidis K, Amar E, Eardley I, et al. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010;57(5):804-814. Qaseem A, Snow V, Denberg TD, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Hormonal testing and pharmacologic treatment of erectile dysfunction: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2009;151(9):639-649. Nehra A, Jackson G, Miner M, et al. The Princeton III Consensus recommendations for the management of erectile dysfunction and cardiovascular disease. Mayo Clin Proc. 2012;87(8):766-778. Saenz de Tejada I, Angulo J, Cuevas P, et al. The phosphodiesterase inhibitory selectivity and the in vitro and in vivo potency of the new PDE5 inhibitor vardenafil. Int J Impot Res. 2001;13:282-290. Yu G, Mason H, Wu X, et al. Substituted pyrazolopyridopyridazines as orally bioavailable potent and selective PDE5 inhibitors: potential agents for treatment of erectile dysfunction. J Med Chem. 2003;46: 457-460. Seftel AD. Phosphodiesterase type 5 inhibitor differentiation based on selectivity, pharmacokinetic, and efficacy profiles. Clin Cardiol. 2004; 27:I14-I19. Sussman DO. Pharmacokinetics, pharmacodynamics, and efficacy of phosphodiesterase type 5 inhibitors. J Am Osteopath Assoc. 2004;104: S11-S15. 827 377. Kedia GT, Uckert S, Assadi-Pour F, et al. Avanafil for the treatment of erectile dysfunction: initial data and clinical key properties. Ther Adv Urol. 2013;5(1):35-41. 378. Limin M, Johnsen N, Hellstrom WJ. Avanafil, a new rapid-onset phosphodiesterase 5 inhibitor for the treatment of erectile dysfunction. Expert Opin Investig Drugs. 2010;19(11):1427-1437. 379. Katz EG, Tan RB, Rittenberg D, Hellstrom WJ. Avanafil for erectile dysfunction in elderly and younger adults: differential pharmacology and clinical utility. Ther Clin Risk Manag. 2014;10:701-711. 380. Cho MC, Paick JS. Udenafil for the treatment of erectile dysfunction. Ther Clin Risk Manag. 2014;10:341-354. 381. Rajagopalan P, Mazzu A, Xia C, et al. Effect of high-fat breakfast and moderate-fat evening meal on the pharmacokinetics of vardenafil, an oral phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction. J Clin Pharmacol. 2003;43:260-267. 382. Nichols DJ, Muirhead GJ, Harness JA. Pharmacokinetics of sildenafil after single oral doses in healthy male subjects: absolute bioavailability, food effects and dose proportionality. Br J Clin Pharmacol. 2002; 53(Suppl 1):5S-12S. 383. Rendell MS, Rajfer J, Wicker PA, Smith MD. Sildenafil for treatment of erectile dysfunction in men with diabetes: a randomized controlled trial. Sildenafil Diabetes Study Group [see comments]. JAMA. 1999;281: 421-426. 384. Blanker MH, Thomas S, Bohnen AM. Systematic review of Viagra RCTs. Br J Gen Pract. 2002;52:329. 385. Burls A, Gold L, Clark W. Systematic review of randomised controlled trials of sildenafil (Viagra) in the treatment of male erectile dysfunction. Br J Gen Pract. 2001;51:1004-1012. 386. Fink HA, Mac Donald R, Rutks IR, et al. Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med. 2002;162:1349-1360. 387. Montorsi F, McCullough A. Efficacy of sildenafil citrate in men with erectile dysfunction following radical prostatectomy: a systematic review of clinical data. J Sex Med. 2005;2:658-667. 388. Moore RA, Derry S, McQuay HJ. Indirect comparison of interventions using published randomised trials: systematic review of PDE-5 inhibitors for erectile dysfunction. BMC Urol. 2005;5:18. 389. Jarow JP, Burnett AL, Geringer AM. Clinical efficacy of sildenafil citrate based on etiology and response to prior treatment [see comments]. J Urol. 1999;162:722-725. 390. Vardi M, Nini A. Phosphodiesterase inhibitors for erectile dysfunction in patients with diabetes mellitus. Cochrane Database Syst Rev. 2007; (1):CD002187. 391. Markou S, Perimenis P, Gyftopoulos K, et al. Vardenafil (Levitra) for erectile dysfunction: a systematic review and meta-analysis of clinical trial reports. Int J Impot Res. 2004;16:470-478. 392. Brock G, Nehra A, Lipshultz LI, et al. Safety and efficacy of vardenafil for the treatment of men with erectile dysfunction after radical retropubic prostatectomy. J Urol. 2003;170:1278-1283. 393. Donatucci C, Eardley I, Buvat J, et al. Vardenafil improves erectile function in men with erectile dysfunction irrespective of disease severity and disease classification. J Sex Med. 2004;1:301-309. 394. Hatzichristou D, Montorsi F, Buvat J, et al. The efficacy and safety of flexible-dose vardenafil (Levitra) in a broad population of European men. Eur Urol. 2004;45:634-641, discussion 641. 395. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl. 2002;23:763-771. 396. Nehra A, Grantmyre J, Nadel A, et al. Vardenafil improved patient satisfaction with erectile hardness, orgasmic function and sexual experience in men with erectile dysfunction following nerve sparing radical prostatectomy. J Urol. 2005;173:2067-2071. 397. Rosen R, Shabsigh R, Berber M, et al. Efficacy and tolerability of vardenafil in men with mild depression and erectile dysfunction: the depression-related improvement with vardenafil for erectile response study. Am J Psychiatry. 2006;163:79-87. 398. Brock GB, McMahon CG, Chen KK, et al. Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol. 2002;168:1332-1336. 399. Carson C, Shabsigh R, Segal S, et al. Efficacy, safety, and treatment satisfaction of tadalafil versus placebo in patients with erectile dysfunction evaluated at tertiary-care academic centers. Urology. 2005;65: 353-359. 400. Padma-Nathan H, McMurray JG, Pullman WE, et al. On-demand IC351 (Cialis) enhances erectile function in patients with erectile dysfunction. Int J Impot Res. 2001;13:2-9. 401. Porst H, Padma-Nathan H, Giuliano F, et al. Efficacy of tadalafil for the treatment of erectile dysfunction at 24 and 36 hours after dosing: a randomized controlled trial. Urology. 2003;62:121-125, discussion 125-126. 402. Saenz de Tejada I, Anglin G, Knight JR, Emmick JT. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care. 2002;25: 2159-2164. 403. Morales A, Gingell C, Collins M, et al. Clinical safety of oral sildenafil citrate (Viagra) in the treatment of erectile dysfunction. Int J Impot Res. 1998;10:69-73. 828 SECTION V Reproduction 404. Coelho OR. Tolerability and safety profile of sildenafil citrate (Viagra) in Latin American patient populations. Int J Impot Res. 2002;14(Suppl 2):S54-S59. 405. Giuliano F, Jackson G, Montorsi F, et al. Safety of sildenafil citrate: review of 67 double-blind placebo-controlled trials and the postmarketing safety database. Int J Clin Pract. 2010;64(2):240-255. 406. Goldstein I, Lue TF, Padma-Nathan H, et al. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group [see comments] [published erratum appears in N Engl J Med. 1998;339(1):59]. N Engl J Med. 1998;338(20):1397-1404. 407. Aversa A, Mazzilli F, Rossi T, et al. Effects of sildenafil (Viagra) administration on seminal parameters and post-ejaculatory refractory time in normal males. Hum Reprod. 2000;15:131-134. 408. Hellstrom WJG, Gittelman M, Jarow J, et al. An evaluation of semen characteristics in men 45 years of age after daily dosing with tadalafil 20 mg: results of a multicenter, randomized, double-blind, placebocontrolled, 9-month study. Eur Urol. 2008;53:1058-1065. 409. Hatzichristou DG. Phosphodiesterase 5 inhibitors and nonarteritic anterior ischemic optic neuropathy (NAION): coincidence or causality. J Sex Med. 2004;2:751-758. 410. Buono L, Foroozan R, Sergott RC, Savino PJ. Nonarteritic anterior ischemic optic neuropathy. Curr Opin Ophthalmol. 2002;13:357-361. 411. Snodgrass AJ, Campbell HM, Mace DL, et al. Sudden sensorineural hearing loss associated with vardenafil. Pharmacotherapy. 2010;30(1): 112. 412. McGwin G Jr. Phosphodiesterase type 5 inhibitor use and hearing impairment. Arch Otolaryngol Head Neck Surg. 2010;136(5):488-492. 413. Li WQ, Qureshi AA, Robinson KC, Han J. Sildenafil use and increased risk of incident melanoma in US men: a prospective cohort study. JAMA Intern Med. 2014;174:964-970. 414. Feenstra J, Drie-Pierik RJ, Lacle CF, Stricker BH. Acute myocardial infarction associated with sildenafil [letter] [see comments]. Lancet. 1998;352:957-958. 415. Zusman RM, Morales A, Glasser DB, Osterloh IH. Overall cardiovascular profile of sildenafil citrate. Am J Cardiol. 1999;83:35C-44C. 416. Herrmann HC, Chang G, Klugherz BD, Mahoney PD. Hemodynamic effects of sildenafil in men with severe coronary artery disease. N Engl J Med. 2000;342:1622-1626. 417. Thadani U, Smith W, Nash S, et al. The effect of vardenafil, a potent and highly selective phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction, on the cardiovascular response to exercise in patients with coronary artery disease. J Am Coll Cardiol. 2002;40: 2006-2012. 418. Jackson G. Hemodynamic and exercise effects of phosphodiesterase 5 inhibitors. Am J Cardiol. 2005;96:32M-36M. 419. Cheitlin MD, Hutter AM Jr, Brindis RG, et al. Use of sildenafil (Viagra) in patients with cardiovascular disease. Technology and Practice Executive Committee [published erratum appears in Circulation. 1999; 100(23):2389] [see comments]. Circulation. 1999;99(1):168-177. 420. Muller JE, Mittleman A, Maclure M, et al. Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants of Myocardial Infarction Onset Study Investigators [see comments]. JAMA. 1996;275:1405-1409. 421. Conti CR, Pepine CJ, Sweeney M. Efficacy and safety of sildenafil citrate in the treatment of erectile dysfunction in patients with ische­ mic heart disease. Am J Cardiol. 1999;83:29C-34C. 422. Carson CC 3rd. Cardiac safety in clinical trials of phosphodiesterase 5 inhibitors. Am J Cardiol. 2005;96:37M-41M. 423. Kloner RA. Novel phosphodiesterase type 5 inhibitors: assessing hemodynamic effects and safety parameters. Clin Cardiol. 2004;27:I20-I25. 424. Vlachopoulos C, Jackson G, Stefanadis C, Montorsi P. Erectile dys­ function in the cardiovascular patient. Eur Heart J. 2013;34(27): 2034-2046. 425. Highleyman L. Protease inhibitors and sildenafil (Viagra) should not be combined. BETA. 1999;12(2):3. 426. Bailey DG, Dresser GK. Interactions between grapefruit juice and cardiovascular drugs. Am J Cardiovasc Drugs. 2004;4:281-297. 427. McCullough AR, Barada JH, Fawzy A, et al. Achieving treatment optimization with sildenafil citrate (Viagra) in patients with erectile dysfunction. Urology. 2002;60:28-38. 428. McMahon C. Comparison of efficacy, safety, and tolerability of on-demand tadalafil and daily dosed tadalafil for the treatment of erectile dysfunction. J Sex Med. 2005;2(3):415-425, discussion 425-427. 429. Porst H, Rajfer J, Casabé A, et al. Long-term safety and efficacy of tadalafil 5 mg dosed once daily in men with erectile dysfunction. J Sex Med. 2008;5:2160-2169. 430. Lau DHW, Kommu S, Mumtaz FH, et al. The management of phosphodiesterase inhibitor failure. Curr Vasc Pharmacol. 2006;4:89-93. 431. Martinez JM. Prognostic factors for response to sildenafil in patients with erectile dysfunction. Eur Urol. 2001;40:641-646. 432. Wespes E, Rammal A, Garbar C. Sildenafil no-responders: hemodynamic and morphometric studies. Eur Urol. 2005;48:136-139. 433. McGarvey MR. Tough choices: the cost-effectiveness of sildenafil [editorial; comment]. Ann Intern Med. 2000;132:994-995. 434. Smith KJ, Roberts MS. The cost-effectiveness of sildenafil [see comments]. Ann Intern Med. 2000;132:933-937. 435. Tan HL. Economic cost of male erectile dysfunction using a decision analytic model: for a hypothetical managed-care plan of 100,000 members. Pharmacoeconomics. 2000;17:77-107. 436. Sun P, Seftel A, Swindle R, et al. The costs of caring for erectile dysfunction in a managed care setting: evidence from a large national claims database. J Urol. 2005;174:1948-1952. 437. Plumb JM, Guest JF. Annual cost of erectile dysfunction to UK Society. Pharmacoeconomics. 1999;16:699-709. 438. Vrijhof HJ, Delaere KP. Vacuum constriction devices in erectile dysfunction: acceptance and effectiveness in patients with impotence of organic or mixed aetiology. Br J Urol. 1994;74:102-105. 439. Cookson MS, Nadig PW. Long-term results with vacuum constriction device. J Urol. 1993;149:290-294. 440. Lewis JH, Sidi AA, Reddy PK. A way to help your patients who use vacuum devices. Contemp Urol. 1991;3:15-21. 441. Engelhardt PF, Plas E, Hubner WA, Pfluger H. Comparison of intraurethral liposomal and intracavernosal prostaglandin-E1 in the management of erectile dysfunction. Br J Urol. 1998;81:441-444. 442. Kim ED, McVary KT. Topical prostaglandin-E1 for the treatment of erectile dysfunction [see comments]. J Urol. 1995;153:1828-1830. 443. Peterson CA, Bennett AH, Hellstrom WJ, et al. Erectile response to transurethral alprostadil, prazosin and alprostadil-prazosin combinations. J Urol. 1998;159:1523-1527. 444. Fulgham PF, Cochran JS, Denman JL, et al. Disappointing initial results with transurethral alprostadil for erectile dysfunction in a urology practice setting. J Urol. 1998;160:2041-2046. 445. Linet OI, Ogrinc FG. Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. The Alprostadil Study Group. N Engl J Med. 1996;334:873-877. 446. El-Sakka AI. Intracavernosal prostaglandin E1 self vs office injection therapy in patients with erectile dysfunction. Int J Impot Res. 2006; 18:180-185. 447. Heaton JP, Lording D, Liu SN, et al. Intracavernosal alprostadil is effective for the treatment of erectile dysfunction in diabetic men. Int J Impot Res. 2001;13:317-321. 448. Tsai YS, Lin JS, Lin YM. Safety and efficacy of alprostadil sterile powder (S. Po., CAVERJECT) in diabetic patients with erectile dysfunction. Eur Urol. 2000;38:177-183. 449. Shabsigh R, Padma-Nathan H, Gittleman M, et al. Intracavernous alprostadil alfadex is more efficacious, better tolerated, and preferred over intraurethral alprostadil plus optional actis: a comparative, randomized, crossover, multicenter study. Urology. 2000;55:109-113. 450. Chew KK. Intracavernosal injection therapy. Does it still have a role in erectile dysfunction? Aust Fam Physician. 2001;30:43-46. 451. The European Alprostadil Study Group. The long-term safety of alprostadil (prostaglandin-E1) in patients with erectile dysfunction. Br J Urol. 1998;82:538-543. 452. Dinsmore WW, Gingell C, Hackett G, et al. Treating men with predominantly nonpsychogenic erectile dysfunction with intracavernosal vasoactive intestinal polypeptide and phentolamine mesylate in a novel auto-injector system: a multicentre double-blind placebocontrolled study. BJU Int. 1999;83:274-279. 453. Mulhall JP, Daller M, Traish AM, et al. Intracavernosal forskolin: role in management of vasculogenic impotence resistant to standard 3-agent pharmacotherapy. J Urol. 1997;158:1752-1758, discussion 1758-1759. 454. Hellstrom WJ, Usta MF. Surgical approaches for advanced Peyronie’s disease patients. Int J Impot Res. 2003;15(Suppl 5):S121-S124. 455. Carson CC, Mulcahy JJ, Govier FE. Efficacy, safety and patient satisfaction outcomes of the AMS 700CX inflatable penile prosthesis: results of a long-term multicenter study. AMS 700CX Study Group. J Urol. 2000;164:376-380. 456. Wilson SK, Cleves MA, Delk JR 2nd. Comparison of mechanical reliability of original and enhanced Mentor Alpha I penile prosthesis. J Urol. 1999;162:715-718. 457. Usta MF, Bivalacqua TJ, Sanabria J, et al. Patient and partner satisfaction and long-term results after surgical treatment for Peyronie’s disease. Urology. 2003;62:105-109. 458. Fink HA, MacDonald R, Rutks IR, Wilt TJ. Trazodone for erectile dysfunction: a systematic review and meta-analysis. BJU Int. 2003;92: 441-446. 459. Lebret T, Herve JM, Gorny P, et al. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. Eur Urol. 2002;41:608-613, discussion 613. 460. Fleshner N, Harvey M, Adomat H, et al. Evidence for pharmacological contamination of herbal erectile function products with type 5 phosphodiesterase inhibitors (abstract). J Urol. 2004;171:314. 461. Hong B, Ji YH, Hong JH, et al. A double-blind crossover study evaluating the efficacy of Korean red ginseng in patients with erectile dysfunction: a preliminary report. J Urol. 2002;168:2070-2073. 462. Jang DJ, Lee MS, Shin BC, et al. Red ginseng for treating erectile dysfunction: a systematic review. Br J Clin Pharmacol. 2008;66(4): 444-450. 463. Ho CC, Tan HM. Rise of herbal and traditional medicine in erectile dysfunction management. Curr Urol Rep. 2011;12(6):470-478. CHAPTER 20 Sexual Dysfunction in Men and Women 464. Shindel AW, Xin ZC, Lin G, et al. Erectogenic and neurotrophic effects of icariin, a purified extract of horny goat weed (Epimedium spp.) in vitro and in vivo. J Sex Med. 2010;7(4 Pt 1):1518-1528. 465. Harraz A, Shindel AW, Lue TF. Emerging gene and stem cell therapies for the treatment of erectile dysfunction. Nat Rev Urol. 2010;7(3): 143-152. 466. Strong TD, Gebska MA, Burnett AL, et al. Endothelium-specific gene and stem cell-based therapy for erectile dysfunction. Asian J Androl. 2008;10(1):14-22. 467. Deng W, Bivalacqua TJ, Hellstrom WJ, Kadowitz PJ. Gene and stem cell therapy for erectile dysfunction. Int J Impot Res. 2005;17(Suppl 1):S57-S63. 468. Garban H, Marquez D, Magee T, et al. Cloning of rat and human inducible penile nitric oxide synthase. Application for gene therapy of erectile dysfunction. Biol Reprod. 1997;56:954-963. 469. Christ GJ, Rehman J, Day N, et al. Intracorporal injection of hSlo cDNA in rats produces physiologically relevant alterations in penile function. Am J Physiol. 1998;275:H600-H608. 470. Bivalacqua TJ, Champion HC, Mehta YS, et al. Adenoviral gene transfer of endothelial nitric oxide synthase (eNOS) to the penis improves age-related erectile dysfunction in the rat. Int J Impot Res. 2000;12(Suppl 3):S8-S17. 471. Champion HC, Bivalacqua TJ, Hyman AL, et al. Gene transfer of endothelial nitric oxide synthase to the penis augments erectile responses in the aged rat. Proc Natl Acad Sci U S A. 1999;96:11648-11652. 472. Burchardt M, Burchardt T, Anastasiadis AG, et al. Application of angiogenic factors for therapy of erectile dysfunction: protein and DNA transfer of VEGF 165 into the rat penis. Urology. 2005;66:665-670. 473. Rogers RS, Graziottin TM, Lin CS, et al. Intracavernosal vascular endothelial growth factor (VEGF) injection and adeno-associated virusmediated VEGF gene therapy prevent and reverse venogenic erectile dysfunction in rats. Int J Impot Res. 2003;15:26-37. 474. Deng W, Bivalacqua TJ, Chattergoon NN, et al. Adenoviral gene transfer of eNOS: high-level expression in ex vivo expanded marrow stromal cells. Am J Physiol Cell Physiol. 2003;285:C1322-C1329. 475. Gholami SS, Rogers R, Chang J, et al. The effect of vascular endothelial growth factor and adeno-associated virus mediated brain derived neurotrophic factor on neurogenic and vasculogenic erectile dysfunction induced by hyperlipidemia. J Urol. 2003;169(4):1577-1581. 476. Deng W, Bivalacqua TJ, Chattergoon NN, et al. Engineering ex vivoexpanded marrow stromal cells to secrete calcitonin gene-related peptide using adenoviral vector. Stem Cells. 2004;22:1279-1291. 477. Melman A, Bar-Chama N, McCullough A, et al. Plasmid-based gene transfer for treatment of erectile dysfunction and overactive bladder: results of a phase I trial. Isr Med Assoc J. 2007;9(3):143-146. 478. Melman A, Bar-Chama N, McCullough A, et al. hMaxi-K gene transfer in males with erectile dysfunction: results of the first human trial. Hum Gene Ther. 2006;17(12):1165-1176. 479. Magee TR, Kovanecz I, Davila HH, et al. Antisense and short hairpin RNA (shRNA) constructs targeting PIN (Protein Inhibitor of NOS) ameliorate aging-related erectile dysfunction in the rat. J Sex Med. 2007;4(3):633-643. 480. Condorelli RA, Calogero AE, Vicari E, et al. Vascular regenerative therapies for the treatment of erectile dysfunction: current approaches. Andrology. 2013;1(4):533-540. 481. Melman A, Davies K. Gene therapy for erectile dysfunction: what is the future? Curr Urol Rep. 2010;11(6):421-426. 482. Garcia MM, Fandel TM, Lin G, et al. Treatment of erectile dysfunction in the obese type 2 diabetic ZDF rat with adipose tissue-derived stem cells. J Sex Med. 2010;7(1 Pt 1):89-98. 483. Bivalacqua TJ, Deng W, Kendirci M, et al. Mesenchymal stem cells alone or ex vivo gene modified with endothelial nitric oxide synthase reverse age-associated erectile dysfunction. Am J Physiol Heart Circ Physiol. 2007;292(3):H1278-H1290. 484. Abdel Aziz MT, El-Haggar S, Mostafa T, et al. Effect of mesenchymal stem cell penile transplantation on erectile signaling of aged rats. Andrologia. 2010;42(3):187-192. 485. Lin CS, Xin Z, Dai J, et al. Stem-cell therapy for erectile dysfunction. Expert Opin Biol Ther. 2013;13(11):1585-1597. 486. Lin CS, Xin ZC, Wang Z, et al. Stem cell therapy for erectile dysfunction: a critical review. Stem Cells Dev. 2012;21(3):343-351. 487. Albersen M, Kendirci M, Van der Aa F, et al. Multipotent stromal cell therapy for cavernous nerve injury-induced erectile dysfunction. J Sex Med. 2012;9(2):385-403. 488. Kim Y, de Miguel F, Usiene I, et al. Injection of skeletal muscle-derived cells into the penis improves erectile function. Int J Impot Res. 2006; 18(4):329-334. 489. Song YS, Lee HJ, Park IH, et al. Potential differentiation of human mesenchymal stem cell transplanted in rat corpus cavernosum toward endothelial or smooth muscle cells. Int J Impot Res. 2007;19:378-385. 490. Nolazco G, Kovanecz I, Vernet D, et al. Effect of muscle-derived stem cells on the restoration of corpora cavernosa smooth muscle and erectile function in the aged rat. BJU Int. 2008;101:1156-1164. 491. Tomasi PA, Fanciulli G, Delitala G. Successful treatment of retrograde ejaculation with the alpha1-adrenergic agonist methoxamine: case study. Int J Impot Res. 2005;17(3):297-299. 829 492. Ochsenkühn R, Kamischke A, Nieschlag E. Imipramine for successful treatment of retrograde ejaculation caused by retroperitoneal surgery. Int J Androl. 1999;22(3):173-177. 493. Safarinejad MR. Midodrine for the treatment of organic anejaculation but not spinal cord injury: a prospective randomized placebocontrolled double-blind clinical study. Int J Impot Res. 2009;21(4): 213-220. 494. Kamischke A, Nieschlag E. Treatment of retrograde ejaculation and anejaculation. Hum Reprod Update. 1999;5:448-474. 495. Webster L. Management of sexual problems in diabetic patients. Br J Hosp Med. 1994;51(9):465-468. 496. Gerig NE, Meacham RB, Ohl DA. Use of electroejaculation in the treatment of ejaculatory failure secondary to diabetes mellitus. Urology. 1997;49(2):239-242. 497. Zhao Y, Garcia J, Jarow JP, Wallach EE. Successful management of infertility due to retrograde ejaculation using assisted reproductive technologies: a report of two cases. Arch Androl. 2004;50(6):391-394. 498. Frühauf S, Gerger H, Maren Schmidt H, et al. Efficacy of psychological interventions for sexual dysfunction: a systematic review and metaanalysis. Arch Sex Behav. 2013;42:915-933. 499. Middleton LS, Kuffel SW. Effects of experimentally adopted sexual schemas on vaginal response and subjective sexual arousal: a comparison between women with arousal disorder and sexually healthy women. Arch Sex Behav. 2008;37:950-961. 500. Brotto LA, Basson R, Luria M. A mindfulness research group psychoeducational intervention targeting sexual arousal disorder in women. J Sex Med. 2008;5:1646-1659. 501. Brotto LA, Basson R. Group mindfulness-based therapy significantly improves sexual desire in women. Behav Res Ther. 2014;57:43-54. 502. Brotto L, Heiman J, Goff B, et al. A psychoeducational intervention for sexual dysfunction in women with gynecologic cancer. Arch Sex Behav. 2008;37(2):317-329. 503. Brotto LA, Basson R, Driscoll M, et al. Mindfulness-based group therapy for women with provoked vestibulodynia. Mindfulness. 2014;6:417-432. 504. Zeidan F, Gordon NS, Merchant J, et al. The effects of brief mindfulness meditation training on experimentally induced pain. J Pain. 2010; 11(3):199-209. 505. Zeidan F, Martucci KT, Kraft RA, et al. Brain mechanisms supporting the modulation of pain by mindfulness meditation. J Neurosci. 2011; 31(14):5540-5548. 506. Ives-Deliperi VL, Solms M, Meintjes EM. The neural substrates of mindfulness: an fMRI investigation. Soc Neurosci. 2011;6(3):231-242. 507. Basson R, Smith KB. Incorporating mindfulness meditation into the treatment of provoked vestibulodynia. Curr Sex Health Rep. 2013; DOI 10. 1007/s1 1930-013-008-0. 508. Brotto LA, Basson R, Carlson M, et al. Impact of an integrated mindfulness and cognitive behavioural treatment for provoked vestibulodynia (IMPROVED): a qualitative study. Sex Rel Ther. 2013;28:3-19. 509. Harley TS. Interventions for sexual problems following treatment for breast cancer: a systematic review. Breast Cancer Res Treat. 2011;130: 711-724. 510. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404. 511. Fooladi E, Bell RJ, Jane F, et al. Testosterone improves antidepressantemergent loss of libido in women: findings from a randomized, double-blind, placebo-controlled trial. J Sex Med. 2014;11:831-839. 512. Danielsson I, Sjoberg I, Stelund H, et al. Prevalence and incidence of prolonged and severe dyspareunia in women: results from a population study. Scand J Public Health. 2003;31:113-118. 513. Morin M, Bergeron S, Khalifé S, et al. Morphometry of the pelvic floor muscles in women with and without provoked vestibulodynia using 4D ultrasound. J Sex Med. 2014;11:776-785. 514. Heddini U, Bohm-Starle N, Gronbladh A, et al. GCH1-polymorphism and pain sensitivity among women with provoked vestibulodynia. Mol Pain. 2012;8:68. 515. Bouchard C, Brisson J, Fortier M, et al. Use of oral contraceptive pills and vulvar vestibulitis: a case-control study. Am J Epidemiol. 2002;156: 254-261. 516. Basson R. The recurrent pain and sexual sequelae of provoked vestibulodynia: a perpetuating cycle. J Sex Med. 2012;9:2077-2092. 517. Desrochers G, Bergeron S, Khalife S, et al. Provoked vestibulodynia: psychological predictors of topical and cognitive-behavioral treatment outcome. Behav Res Ther. 2010;48:106-115. 518. Spoelstra SK, Dijkstra JR, van Driel MF, et al. Long-term results of an individualized, multifaceted, and multidisciplinary therapeutic approach to provoked vestibulodynia. J Sex Med. 2011;8:489-496. 519. Tommola P, Unkila-Kallio L, Paavonen J. Surgical treatment of vulvar vestibulitis: a review. Acta Obstet Gynecol Scand. 2010;89:1385-1395. 520. Vachon-Presseau E, Roy M, Martel MO, et al. The stress model of chronic pain: evidence from basal cortisol and hippocampal structure and function in humans. Brain. 2013;136:815-827. 521. Borsook D, Maleki N, Becerra L, et al. Understanding migraine through the lens of maladaptive stress responses: a model disease of allostatic load. Neuron. 2012;73(2):219-234. 830 SECTION V Reproduction 521a. Basson R, Driscoll M, Correia S. Flibanserin for low sexual desire in women: a molecule from bench to bed? E BioMed. 2015;2:772-773. 522. McEwen BS, Stellar E. Stress and the individual. Mechanisms leading to disease. Arch Intern Med. 1993;153:2903-3101. 523. Khandker M, Brady SS, Vitonis AF, et al. The influence of depression and anxiety on risk of adult onset vulvodynia. J Women’s Health. 2011; 20:1445-1451. 524. Brotto LA, Basson R, Gehring D. Psychological profiles among women with vulvar vestibulitis syndrome: a chart review. J Psychosom Obstet Gynecol. 2003;24:195-203. 525. Danielsson I, Sjoberg I, Wikman M. Vulvar vestibulitis: medical, psychosexual and psychosocial aspects, a case control study. Acta Obstet Gynecol Scand. 2000;79:872-878. 526. Jantos M, White G. The vestibulitis syndrome: medical and psychosexual assessment of a cohort of patients. J Reprod Med. 1997;42: 145-152. 527. Ehrström S, Kornfeld D, Rylander E, et al. Chronic stress in women with localized provoked vulvodynia. J Psychosom Obstet Gynecol. 2009;30:73-79. 528. Bergeron S, Khalifé S, Glazer HI, et al. Surgical and behavioral treatments for vestibulodynia: two-and-one-half year follow-up and predictors of outcome. Obstet Gynecol. 2008;111:159-166. 529. Schweinhardt P, Kuchinad A, Pukall CF, et al. Increased gray matter density in young women with chronic vulvar pain. Pain. 2008;140: 411-419. 530. van Lankveld JJ, ter Kuile MM, de Groot HE, et al. Cognitivebehavioral therapy for women with lifelong vaginismus: a randomized waiting-list controlled trial of efficacy. J Consult Clin Psychol. 2006;74:168-178. 531. Rosenbaum TY. An integrated mindfulness-based approach to the treatment of women with sexual pain and anxiety: promoting autonomy and mind/body connection. Sex Rel Ther. 2013;28:20-28. 532. Ter Kuile MM, Melles R, de Groot HE, et al. Therapist-aided exposure for women with lifelong vaginismus: a randomized waiting-list control of efficacy. J Consult Clin Psychol. 2013;81(6):1127-1136. 533. Braunstein GD, Sundwall DA, Katz M, et al. Safety and efficacy of a testosterone patch for the treatment of hypoactive sexual desire disorder in surgically menopausal women: a randomized, placebo-controlled trial. Arch Intern Med. 2005;165:1582-1589. 534. Arlt W. Androgen therapy in women. Eur J Endocrinol. 2006;154: 1-11. 535. Shifren JL, Davis SR, Moreau M, et al. Testosterone patch for the treatment of hypoactive sexual desire disorder in naturally menopausal women: results from the INTIMATE NM1 Study. Menopause. 2006;13: 770-779. 536. Davis SR, Moreau M, Kroll R, et al. Testosterone for low libido in postmenopausal women not taking estrogen. N Engl J Med. 2008;359: 2005-2017. 537. Panay N, Al-Azzawi F, Bouchard C, et al. Testosterone treatment of HSDD in naturally menopausal women: the ADORE study. Climacteric. 2010;13(2):121-131. 538. Snabes MC, Zborowski J, Simes S. Libigel (testosterone gel) does not differentiate from placebo therapy in the treatment of hypoactive sexual desire in postmenopausal women. J Sex Med. 2012;S3:S171. 539. Davis S, Papalia MA, Norman RJ, et al. Safety and efficacy of a testosterone metered-dose transdermal spray for treatment of decreased sexual satisfaction in premenopausal women: a placebo-controlled randomized, dose ranging study. Ann Intern Med. 2008;148:569-577. 540. Van der Nadem F, Bloemers J, Yassem WE, et al. The influence of testosterone combined with a PDE5-inhibitor on cognitive, effective, and physiological sexual functioning in women suffering from sexual dysfunction. J Sex Med. 2009;6:777-790. 541. Cain VS, Johannes CB, Avis NE, et al. Sexual functioning and practices in a multi-ethnic study of midlife women: baseline results from SWAN. J Sex Res. 2003;40:266-276. 542. Carvalheira AA, Brotto LA, Leal I. Women’s motivations for sex: exploring the diagnostic and statistical manual, fourth edition, text revision criteria for hypoactive sexual desire and female sexual arousal disorders. J Sex Med. 2010;7:1454-1463. 543. Basson R. Testosterone supplementation to improve women’s sexual satisfaction: complexities and unknowns [editorial]. Ann Intern Med. 2008;148:620-621. 544. Padero MC, Bhasin S, Friedman TC. Androgen supplementation in older women: too much hype, not enough data. J Am Geriatr Soc. 2002;50:1131-1140. 545. Schover LR. Androgen therapy for loss of desire in women: is the benefit worth the breast cancer risk? Fertil Steril. 2008;90:129-140. 546. Bradford A, Meston CM. Placebo response in the treatment of women’s sexual dysfunctions: a review and commentary. J Sex Marital Ther. 2009;35:164-181. 547. Braunstein GD. Management of female sexual dysfunction in postmenopausal women by testosterone administration: safety issues and controversies. J Sex Med. 2007;4(4 Pt 1):859-866. 548. Wierman M, Arlt W, Basson R, et al. Androgen therapy in women: a reappraisal: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(10):3489-3510. 549. Wild RA. Endogenous androgens and cardiovascular risk. Menopause. 2007;14:609-610. 550. Bell RJ, Davison SL, Papalia MA, et al. Endogenous androgen levels and cardiovascular risk profile in women across the adult life span. Menopause. 2007;14:630-638. 551. Guthrie JR, Dennerstein L, Taffe JR, et al. The menopausal transition: a 9-year prospective population-based study. The Melbourne Women’s Midlife Health Project. Climacteric. 2004;7:375-389. 552. Sutton-Tyrrell K, Zhao X, Santoro N, et al. Reproductive hormones and obesity: 9 years of observation from the Study of Women’s Health Across the Nation. Am J Epidemiol. 2010;171:1203-1213. 553. Elraiyah T, Sonbol MB, Wang Z, et al. The benefits and harms of systemic testosterone therapy in postmenopausal women with normal adrenal function. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99:3543-3550. 554. Brotto LA, Petkau AJ, Labrie F, Basson R. Predictors of sexual desire disorders in women. J Sex Med. 2011;8:742-753. 555. Dennerstein L, Dudley E, Burger H. Are changes in sexual functioning during midlife due to aging or menopause? Fertil Steril. 2011;76: 456-460. 556. Woods NF, Mitchell ES, Smith-Di Julio K. Sexual desire during menopause transition and early postmenopause: observations from the Seattle Midlife Women’s Health Study. J Women’s Health. 2010;19: 209-218. 557. Elraiyah T, Sonbol MB, Wang Z, et al. Clinical review: The benefits and harms of systemic dehydroepiandrosterone (DHEA) in postmenopausal women with normal adrenal function. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99(10):3536-3542. 558. Labrie F, Archer D, Bouchard C, et al. Effect of intravaginal prasterone (DHEA) on libido and sexual dysfunction in postmenopausal women. Menopause. 2009;16:923-931. 559. Pelletier G, Ouillet J, Martel C, et al. Effects of ovariectomy and dehydroepiandrosterone (DHEA) on vaginal wall thickness and innervation. J Sex Med. 2012;9:2525-2533. 560. Kao A, Binik YM, Amsel R, et al. Challenging atrophied perspectives on postmenopausal dyspareunia: a systematic description and synthesis of clinical pain characteristics. J Sex Marital Ther. 2012;38: 128-150. 561. Kendal A, Dowsett M, Folkerd E, et al. Caution: vaginal estradiol appears to be contraindicated in postmenopausal women on adjunct aromatase inhibitors. Ann Oncol. 2006;17:584-587. 562. Krychman ML, Katz A. Breast cancer and sexuality: multi-modal treatment options. J Sex Med. 2012;9:5-213. 563. Chen J, Geng L, Song X, et al. Evaluation of the efficacy and safety of hyaluronic acid vaginal gel to ease vaginal dryness: a multicenter, randomized, controlled, open-label, parallel-group, clinical trial. J Sex Med. 2013;10:1575-1584. 564. Bachman GA, Schaefers M, Uddin A, et al. Microdose transdermal estrogen therapy for relief of vulvovaginal symptoms in postmenopausal women. Menopause. 2009;16:877-882. 565. Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med. 2003;348:1839-1854.