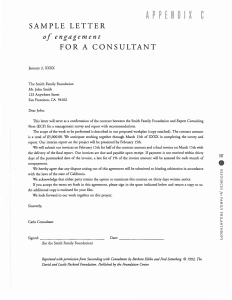
2/16/22, 12:10 PM Providers_VAX Invoice Submittal Tracking Number 1480 Providers VAX Secure Invoice Upload Date 2/13/2022 Contract Information Please enter the conract number first to automatically populate the fields listed with an asterisk (*) Please note that these fields are "Read Only" and edits are not permitted on the form. OTH-VAX-576 M Holdings LLC DBA My Pharmacy 83-1454255 7000297256 Contract Number (required) * Contractor Name * Tax ID * SCEIS Number James Hampton Manning Pharmacist, Owner (843) 845-7905 Contact (Full Name) Title Phone 808 Highway 378 Suite B * Address * STE # INVOICE NUMBER hamp@mypharmacyandoptical.com EXT Contact EMAIL Lexington SC 29072 * City * State * Zip INVOICE AMOUNT 22 20,459.22 Please Upload Invoice for Payment Review To ensure prompt processing of your invoice ensure that you include the invoice number in the file name that you upload. Please ensure that all required information is included on the invoice. Click below for more details ap rec 02/16/2022 Secure Document Upload Please upload the invoice PDF to our secure website using the buttons below. tent lightning receipt_GF_december_cov19 tent Spectrum internet_G Ferry december invoice office rental_Carolina_Mobile_Storage_GF_december misc receipts_combined_GF_dec 2021 M Ph i i 22 l ti GF D Signature (required) Click to Sign I certify that no other funds have been received or will be reimbursed by any James Hampton Manning other source for the amounts claimed on 2/13/2022 6:09:00 PM this invoice $20,459.22 Invoice Total ACC Testing Approval Bonner, Melissa 2/14/2022 8:54:24 AM Yes No b 2022 The attached invoice is acurate and the invoice total is correct. Budget and Finance Approval Samuels, Tierra B. Approved Funding Approved Invoices to Date 2/15/2022 10:36:12 AM Availible Funding Payment Processing Instructions Full Amount $20,459.22 31070000 Not Relevant J0402AZ998 J040X01058580130 5021310000 98000018 $0.00 Accounts Payable Approval Cate, Vasa 2/16/2022 12:10:12 PM If rejecting this form for any reason please provide a brief note to the agency. It will be included in the rejection email notification https://liquidoffice.dhec.sc.gov/lfserver?DFS__Action=RouteGetForm&DFS__EventID=a802cab6b3a7fc091d4e78a7_380017019&DFS__DataSource=… 1/1 COVID-19 Vaccination Reimbursement Request Community Vaccination Event Information* Provider Name: M Holdings LLC DBA My Pharmacy COVID-19 Vaccine Pin Number: 932016 Location Name: My Pharmacy - Garners Ferry Location Address (incl zip): 7501 Garners Ferry Rd Date & Times: December 1st 2021 - December 31st 2021 Columbia, SC 29209 Total # Vaccinations: 1543 Eligible Vaccinations**: Please select yes or no to the following questions to determine eligible reimbursement: Yes Did your organization provide event management, traffic control and logistics for this event? Yes Did your organization provide administrative staff for this event? Yes Did you organization provide vaccination staff for this event? Reimbursement Calculator Item Rate Event Mgmt, Traffic, Logistics $10 $15,430 Administrative Staff $5 $0 Vaccination Staff $15 Total Event Reimbursement Amount Additional Cost Summary***: Total additional cost: Less other funding/reimbursement: Net additional cost: Eligible Event $0 $15,430 $5,029.22 $5,029.22 Total Request Amount: $20,459.22 * Community Vaccination Events may span multiple days as long as the event location remains the same. All dates should be specified. ** If seeking third-party reimbursement for the services at the event was not appropriate or feasible, then all vaccinations are eligible for reimbursement. If billing third party payers was feasible, then only vaccinations not eligible for insurance reimbursement are eligible for Staffing Reimbursement. *** Claiming additional costs requires detailed justification and documentation. Please attach answers to the following questions: 1) Summary Description of Request and Costs 2) Describe Benefit to the State of South Carolina and Statewide Vacinnation Efforts including the future distribution and administering of vaccines. 3) Describe activities conducted and outcomes expected or achieved 4) Is the cost being covered by any other funding source or insurance? Please explain. 5) Were all avenues of funding exhausted before using Vaccine Reserve Account funds? Please explain. Please fill in the green cells in this document to calculate the eligible reimbursement for your event. This form will need to be submitted in the invoice portal either as a PDF or XLSX file for each testing event. Sign Rental 280.8 Mobile Office-Rental GF 246.6 Misc / Supplies 38.26 41.96 98.03 41.96 550.71 451.07 32.78 101.4 22.68 1378.85 Internet Sign Rental Mobile Storage Misc/Supplies Site Rental Total 122.97 280.8 246.6 1378.85 3000 5029.22 Site Rental 3000 Internet-Spectrum 122.97 My Pharmacy 808 Hwy 378 Ste B Lexington, SC 29072 Invoice #22 Additional Expense Explanation Explanation of expenses for Covid 19 drive thru Immunization Clinic expenses from 12/1/2021 – 12/31/2021 Off Site Location 7501 Garners Ferry Rd Columbia, SC 29209 General description: We have a two-lane drive thru Covid 19 immunization tent located in the front parking lot of Southeastern Salvage. This is an off-site clinic we set up due to the need in the area for vaccines. It required a great deal of expense to set-up but this clinic is on-going. This clinic requires a lot of expenses that are specifically related to the tent and our workflow process for vaccinating the public. From 12/01/2021 thru 12/31/2021 we have immunized 1543 patients. Due to the fact this site is not attached to a physical location we had to make arrangements to secure supplies, equipment, vaccine, etc. and set up a mobile office/storage unit to be able to effectively run and serve the patients in the surrounding areas. This has benefited and continues to benefit South Carolina’s COVID 19 vaccination effort due to our ease of access to the public, by taking walk ins, advertising extensively to underserved populations, and providing access to key rural areas surrounding the midlands. We provide a high quality and very efficient process for patients to be vaccinated with convenient hours. Currently the clinic runs Monday thru Friday from 9am to 6pm and Saturday 9am to 3 pm. The below submitted costs are not being covered by any other funding source and have been fully paid for by our business. All other avenues were exhausted before using this fund. Summary of Expenses: 1. 2. 3. 4. 5. 6. Direction/Operational hours signing: a. This was needed to direct traffic and display operating hours. Lease/Rent: a. We are having to lease the drive thru space (parking lot) from property owner. Mobile Office: a. We had to rent and have this unit delivered to store our supplies, draw up doses and house freezer, fridge to store vaccines, and for general admin usage. Propane: a. Used to run heaters. Cold weather has been extreme. Internet: a. Used to process vaccines and input data. Misc Supplies: a. We had to purchase specific supplies directly used for the purpose of the drive thru tent. The receipts have details of the expense or the file type has the detail/explanation. Thank you. Hamp Manning, PharmD/Owner Brent Munnerlyn, PharmD/Owner 1/6/2021 To whom it may concern: As part of the COVID-19 response, DHEC has many partners and vendors who are assisting with testing, contact tracing, and other critical response activities. In order to maintain good working relationships with all our partners and vendors, as well as avoid interruption in services provided, we are requesting the ability process all invoices related to COVID-19 as a Zspecial to expedite payments. If you need additional detail or have any questions or concerns regarding these invoices, please do not hesitate to reach out to ACC-FinAdmin@dhec.sc.gov. Sincerely, Darbi C MacPhail, MHA Chief Finance and Operations Officer SC Department of Health and Environmental Control East Pointe Station LLC Tenant Name: My Pharmacy Billing Address: 808 Highway 378 Brent Munnerlyn BLACKSBURG, SC, US 29702 The following charges are due on 12/01/2021. Late fees can be assessed accordingly Item # Bill Code Description 0007936788 TMP Temporary Rent - Dec 2021 Master Occupant Id: MOC-00024578 Invoice No.: R010663-028876-20211101 Invoice Date: 12/01/2021 Page: 1 Lease ID: 028876 Lease Exp.: 03/15/2022 Due Date: 12/01/2021 Email: Brent@mypharmacyandoptical.com If you have questions about your invoice, please contact your Customer Solutions Specialist, Debbe Webster at 513-338-2837 or send us a message by visiting www.DashComm.com and submitting a Billing Request. Charges $3,000.00 Total Invoice Amount: $3,000.00 Total Outstanding: For more information on your total outstanding balance access ARC through DashComm to view your detailed invoices Please Pay online through ARC or send a check to the below address. EAST POINTE STATION LLC NW 601202 P.O. Box 1450 Minneapolis MN, 554851202 $0.00 Invoice Carolina Mobile Storage, LLC 139 Jed Park Place Summerville, SC 29486 Bill To Invoice# 12/14/2021 52274 Ship To My Pharmacy and Optical Brent Munnerlyn 808 US Hwy 378 Lexington, SC 29072 P.O. Number Date 7501 Garners Ferry Rd Columbia, SC 29209 Brent - 803-261-8615 Terms Rep Ship Doors Toward Due on receipt RTG 12/14/2021 Cab Quantity Description Price Each 1 Monthly rental of a 20' ground level office combo container O20516 Rent Period Sales Tax 245.00 Amount 245.00T 12/21/21 - 1/20/22 8.00% 19.60 We thank you for your business! Total Phone # Fax # E-mail (843) 851-2661 (843) 851-2664 rick@carolinamobilestorage.com Balance Due $264.60 $0.00 December 14, 2021 Invoice Number: Account Number: Security Code: Service At: Auto Pay Notice 257436901121421 202-257436901-001 9594 7501 GARNERS FERRY RD BLDG CONS APT TRLR COLUMBIA, SC 29209-2627 Contact Us Visit us at SpectrumBusiness.net Or, call us at 1-866-892-4249 Summary Services from 12/13/21 through 01/12/22 details on following pages Previous Balance Payment Received - Thank You Remaining Balance Spectrum Business™ Internet Spectrum Business™ Voice Current Charges 247.60 -247.60 $0.00 102.98 19.99 $122.97 YOUR AUTO PAY WILL BE PROCESSED 12/30/21 Total Due by Auto Pay $122.97 NEWS AND INFORMATION NOTE. Taxes, Fees and Charges listed in the Summary only apply to Spectrum Business TV and Spectrum Business Internet and are detailed on the following page. Taxes, Fees and Charges for Spectrum Business Voice are detailed in the Billing Information section. _________________________ REMITTANCE PAYMENT NAME CHANGE: The name of the company that you remit payment to for your monthly Spectrum Business services will be updated to Charter Communications. The new name is included on this month's billing statement. To ensure your payments are received and processed on time, please update any bill-payment software or service that your business may use to reflect this new name. You can download an updated W9 at www.SpectrumBusiness.net/W9. _________________________ Add Spectrum Business TV Essentials for only $19.99/mo and get the best programming, reliable service and unbeatable value. Call 1-866-463-9897 today! _________________________ Presenting Spectrum Mobile, the best mobile deal for your business for only $29.99/line for 2 or more lines. Call 1-877-819-1691 to save up to 60%! _________________________ Thank you for choosing Spectrum Business. We appreciate your prompt payment and value you as a customer. December 14, 2021 MY PHARMACY AND OPTICAL 4145 S. Falkenburg Rd Riverview, FL 33578-8652 6810 0232 NO RP 14 12142021 NNNNNNNN 01 997480 MY PHARMACY AND OPTICAL 7501 GARNERS FERRY RD BLDG CONS APT TRLR COLUMBIA SC 29209-2627 Invoice Number: 257436901121421 Account Number: 202-257436901-001 Service At: 7501 GARNERS FERRY RD BLDG CONS APT TRLR COLUMBIA, SC 29209-2627 Total Due by Auto Pay CHARTER COMMUNICATIONS PO BOX 4617 CAROL STREAM, IL 60197-4617 05005001202257436901780012297 $122.97 Page 2 of 4 December 14, 2021 Invoice Number: Account Number: Security Code: MY PHARMACY AND OPTICAL 257436901121421 202-257436901-001 9594 Charge Details Previous Balance Payment Received - Thank You Remaining Balance 11/23 247.60 -247.60 $0.00 Contact Us Visit us at SpectrumBusiness.net Or, call us at 1-866-892-4249 6810 0232 NO RP 14 12142021 NNNNNNNN 01 997480 Spectrum Terms and Conditions of Service – In accordance with the Spectrum Business Services Agreement, Spectrum services are billed on a monthly basis. Spectrum does not provide credits for monthly subscription services that are cancelled prior to the end of the current billing month. Payments received after 12/14/21 will appear on your next bill. Terms & Conditions - Spectrum's detailed standard terms and conditions for service are located at spectrum.com/policies . Services from 12/13/21 through 01/12/22 Past Due Fee / Late Fee Reminder - A late fee will be assessed for past due charges for service. Spectrum Business™ Internet Franchise Administrator - South Carolina Department of Consumer Affairs PO Box 5757 Columbia, SC 29250 Phone: (803) 734-4200 Spectrum Business Internet Ultra Business WiFi Promotional Discount 199.99 7.99 -105.00 $102.98 Spectrum Business™ Internet Total $102.98 Spectrum Business™ Voice Phone Number (803) 708-6520 Spectrum Business Voice Promotional Discount Promo Discount 49.99 -20.00 -10.00 $19.99 For additional call details, please visit SpectrumBusiness.net Spectrum Business™ Voice Total Current Charges Total Due by Auto Pay The following taxes, fees and surcharges are included in the price of the applicable service - Federal USF $1.21, Sales Tax $1.15, State Excise Tax $0.49, Local GRT Recovery Fee $0.41, E911 Fee $0.35, Regulatory Recovery Fee $0.22, State USF $0.03. Voice Fees and Charges - These include charges, to recover or defray government fees imposed on Spectrum, and certain other costs related to Spectrum's Voice service, including a Federal Universal Service Charge and, if applicable, a State Universal Service Charge to recover amounts Spectrum must pay to support affordable telephone service, and may include a state Telecommunications Relay Service Fee to support relay services for hearing and speech impaired customers. Please note that these charges are not taxes and are subject to change. For more information, visit spectrum.net/taxesandfees. Complaint Procedures - You have 60 days from the billing date to register a complaint if you disagree with your charges. $19.99 $122.97 $122.97 Authorization to Convert your Check to an Electronic Funds Transfer Debit - If your check is returned, you expressly authorize your bank account to be electronically debited for the amount of the check plus any applicable fees. The use of a check for payment is your acknowledgment and acceptance of this policy and its terms and conditions. Tax and Fees - This statement reflects the current taxes and fees for your area (including sales, excise, user taxes, etc.). These taxes and fees may change without notice. Visit Spectrum.com/stores for store locations. For questions or concerns, visit Spectrum.net/support. For questions or concerns, please call 1-866-892-4249. Page 3 of 4 December 14, 2021 Invoice Number: Account Number: Security Code: MY PHARMACY AND OPTICAL 257436901121421 202-257436901-001 9594 Contact Us Visit us at SpectrumBusiness.net Or, call us at 1-866-892-4249 6810 0232 NO RP 14 12142021 NNNNNNNN 01 997480 Page 4 of 4 December 14, 2021 Invoice Number: Account Number: Security Code: MY PHARMACY AND OPTICAL 257436901121421 202-257436901-001 9594 Contact Us Visit us at SpectrumBusiness.net Or, call us at 1-866-892-4249 6810 0232 NO RP 14 12142021 NNNNNNNN 01 997480