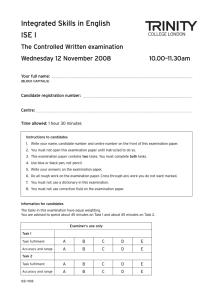
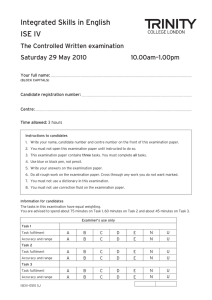
This is not the official DMV Medical Examination Report, it was
Anuncio

/I.Jf A Public Service Agency 051 MEDICAL EXAMINATION REPORT FOR COMMERCIAL DRIVER FITNESS DETERMINATION 1. DRIVIER INFORMATM;)N Qriver completes thla HQUon. PRINT IN CAPITAL LETTERS · USING BLACK ot:t DARK BLUE INK. DRIVER LICENSE NUMBER FIRST LAST NA ME t, po l r a o i ep r c u i f p f DR n D I D e o n tio Ds De IDA o i h t DF at eta tDM o in rpI r n m PLEASE READ THE "INSTRUCTIONS TO THE DRIVER" BEFOREANSWERING. s xa i e t s n E i i Dh T ical for 0 ed IMG M y V b M d D te a FOLWWING INFORMATION e r c s a w M.USI t i STATE CITY ADDRESS SOCIAL SECURITY NUMBER LICENSE CLASS , ZIP STATE OF ISSUE New certification SEX AGE BIRTH DATE . s se Recertification Follow up EYES MARK ONE OF THE DRIVING TYPES BELOW 0 D Nl Non-Excepted Interstate El Excepted Interstate (Not available in California) NA Non-Excepted Intrastate EA Excepted Intrastate (Not available in California) CHECK ONE OF THE BOXES BELOW 0 0 1 am NOI. submitting this medical examination report to obtain a certificate to operate a School Bus, School Pupil Activity Bus, Youth Bus, General Public Paratransit Vehicle, or Farm Labor Vehicle. �submitting this medical examination report to apply for or retain a certificate to operate a School Bus, School Pupil Activity Bus, Youth Bus, General Public Paratransit Vehicle, or Farm Labor Vehicle. PLEASE READ THE If you indicated you have submitted this medical examination report for one or more of the certificates listed above, your medical examination a Physician Assistant, Advanced Practice Registered Nurse, Doctor of Medicine (MD), Doctor of Osteopathy (DO), or a Doctor of Chiropractic (Chiropractor) listed on the most current National Registry of Certified Medical Examiners. Your medical examination report and medical certificate be signed by the physician who performed the examination. If your medical examination report does not indicate your medical examination was performed by an MD, DO, Physician Assistant, Advanced Practice Registered Nurse or a Chiropractor listed on the most current National Registry of Certified Medical Examiners; D MV will not process your certificate application or accept your medical examination report, and your medical examination report will be returned to you. M..1J.SI be performed by 2. HEALTH HISTORY Driver completes ttlla aectlon• .,_ medical examiner Ia encouraged to dlacua with driver. Yes No Yes No enfermedad o lastimadura enyears los últimos 5 años DD Shortness Dificultad paraofrespirar DDAlguna Any illness or injury in last 5 breath Enfermedades pulmonares, enfisema, asma, o lastimaduras de la cabeza/cerebro DDEnfermedades Head/Brain injuries, disorders or illnesses DD Lung disease, emphysema, asthma, bronquitis crónica DD Convulsiones/ataques, Seizures, epilepsy epilepsia chronic bronchitis Enfermedades del riñón, diálisis D Medicación medication DD Kidney disease, dialysis Enfermedades del hígado de or los impaired ojos o dificultad D D Liver disease DD Enfermedades Eye disorders vision (except para ver (excepto cuando usa lentes) Problemas digestivos corrective lenses) D D Digestive problems Diabetes o azúcar alta en la sangresugar de los oídos, pérdida del o balance DD Diabetes or elevated blood D DEnfermedades Ear disorders, loss of hearing oroído balance controlada con: del or corazón controlled by: D D Enfermedades Heart disease hearto ataque attack,alother corazón, otra condición cardiovascular DDieta diet cardiovascular condition D Píldoras pills D Medicación medication corazón(valve (reemplazo de DInsulina insulin D D Cirugía Heart del surgery replacement/ válvula, bypass/derivación, angioplastía, marcapaso) bypass, angioplasty, pacemaker) Presión arterialpressure alta High blood DD DMedicación medication musculares D D Enfermedades Muscular disease nerviosas o psiquiátricas, D D Enfermedades Nervous or psychiatric disorders, por ejemplo depresión severa e.g., severe depression Medicación medication Yes No mareos DDDesmayos, Fainting, dizziness del sueño, pausas in al respirar DDDesórdenes Sleep disorders, pauses breathing cuando duerme, somnolencia durante el día, while asleep, daytime sleepiness, loud rónquidos fuertes snoring Ataque o parálisis Strokecerebral or paralysis DD o deterioro de función de la mano, brazo,leg, DDFalta Missing or impaired hand, arm, foot, pie, pierna, dedo de la mano o del pie finger, toe o enfermedad de la columna vertebral DD Lastimadura Spinal injury or disease Dolor de espalda baja pain crónico DD Chronic low back Uso regularfrequent o frecuentealcohol del alcohol DD Regular, use o uso de narcóticos o drogas DD Hábito Narcotic orformado habit forming drug use · D o alteración de la consciencia DDPérdida Loss of, or altered consciousness _________ For any YES answer, indicate onset date, diagnosis, treating physician's name and address, and any current limitation. List all medications (including over-the-counter medications) used regularly or recently. (Attach additional sheet, if needed). I certify (or declare) under penalty of perjury under the laws of the State of California that the foregoing is true and correct. I understand that inaccurate, false or missing information may invalidate the examination and my Medical Examiner's Certification. DRIVER"S SIGNATURE L.:: X REV. 11/2014) Page 1 of 4