Ischemic stroke in young adults: a diagnostic challenge
Anuncio

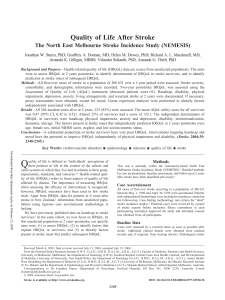
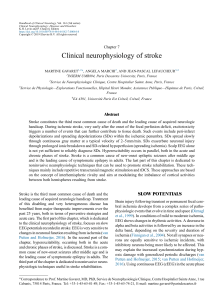
Neuroradiology Original article Ischemic stroke in young adults: a diagnostic challenge María Belén Nallino1, Adriana Ojeda2, Ana María Uriarte3 Resumen Abstract Introducción. El stroke isquémico en pacientes jóvenes (entre 15 y 45 años) es un evento inesperado, cuyas causas incluyen patologías diversas y poco frecuentes en la población adulta. Objetivo. Destacar el creciente rol de las neuroimágenes en el diagnóstico, la terapéutica y el pronóstico del accidente cerebrovascular isquémico (ACV) en pacientes jóvenes. Materiales y Métodos. Se incluyeron retrospectivamente 30 pacientes entre 15 y 45 años con stroke isquémico agudo estudiados en nuestra institución en el último año. Resultados. De los 30 pacientes, la mitad de ellos fueron hombres con una edad media de 35 años. En el 86% de los casos (n=26) se estableció la causa del ACV: el 7% (n=2) presentó ateroesclerosis de grandes vasos, el 10% (n=3) se relacionó a cardioembolismo, en el 27% (n=8) las disecciones arteriales fueron la causa y en el 43% (n=13) las etiologías fueron misceláneas. En el 13% (n=4) no se estableció la causa. Conclusiones. El rol de las neuroimágenes en el desafiante estudio de pacientes jóvenes con ACV incluye la confirmación de la naturaleza isquémica de la lesión, la determinación de su localización y extensión, y el estudio en forma rápida y no invasiva de los vasos extra e intracraneanos. En estos aspectos la tomografía multicorte (TCMS) y la resonancia magnética (RM) de alto campo ofrecen alta sensibilidad y especificidad. Palabras clave. Adulto joven. RM. Stroke isquémico. TCMS. Ischemic stroke in young adults: a challenging diagnosis Introduction. Ischemic stroke in patients between the ages of 15 and 45 is an unexpected event. Its causes involve diverse pathologies which are not frequent in the older population. Purpose. To highlight the important role of neuroimaging in the diagnosis, prognosis, and therapeutical approach of these patients. Materials and Methods. 30 young adult patients between the ages of 15 and 45 with diagnosis of acute ischemic stroke were retrospectively studied. Results. Of these 30 patients, half of them were men with a mean age of 35 years. Stroke etiology was established in 86% of the cases (n=26), 7% (n=2) due to atherosclerosis, 10% (n=3) due to cardioembolism, 27% (n=8) because of arterial dissection, and 43% (n=13) due to miscellaneous diseases. In 13% (n=4) of the cases the cause was undetermined. Conclusions. Neuroimages play a comprehensive role in the neuroradiological work-up which include: the confirmation of the presence of an acute ischemic lesion, determination of its topography, extension and evaluation of extracranial and intracranial arteries. In this sense, Magnetic Resonance Imaging (MRI) and Multislice Computed Tomography (MSCT) offer high sensitivity and resolution. Key words. Ischemic stroke. MRI. MSCT. Young adult. INTRODUCTION MATERIALS AND METHODS Ischemic stroke is defined as a focal neurologic deficit that is present for longer than 24 hours and with no apparent cause other than that of vascular origin. In young adults (15-45 years) it is an unexpected event, and its causes involve diverse pathologies which are infrequent in the older population (1-3). Thirty patients aged between 15 and 45 years admitted to our institution with acute ischemic stroke during the last year were retrospectively included in the study. Neuroimages with a particular emphasis on the neurovascular study were obtained from a 64- and 8-channel multislice computed tomography scanner and a high-field 1.5 Tesla MRI scanner using routine scan protocols and diffusion sequences. Clinical data, history, risk factors, cardiovascular evaluation and laboratory test results were collected. OBJECTIVE The objective is to highlight the increasingly important role of neuroimaging in the diagnosis, therapy and prognosis of ischemic stroke in young adults. Médica residente en Diagnóstico por Imágenes, Fundación J.R. Villavicencio. Médicas especialistas en Diagnóstico por Imágenes, Servicio de Neurorradiología, Diagnóstico Médico Oroño, Sanatorio Parque. Correspondencia: Dra. María Belén Nallino - belunallino@hotmail.com 1 2, 3 RAR - Volumen 75 - Número 2 - 2011 Recibido: enero 2011; aceptado: marzo 2011 Received: january 2011; accepted: march 2011 ©SAR-FAARDIT Página 1 Ischemic stroke in young adults a b c Fig. 1: Forty-year-old female with no previous history, with an acute episode of headache/neck pain, dizziness and vomiting. (a) FSE T2 (b) Diffusion. Small acute ischemic lesion in the lateral fossula of the left medulla. (c) SE T1. Mural hematoma of the left vertebral artery (arrow). a b c Fig. 2: Thirty-year-old female, with a history of severe car accident trauma, who developed aphasia and right-sided hemiparesis. MSCT angiography (a) sagittal MIP reconstruction (b) 3D image. Abrupt stenosis of the left internal carotid artery. (c) Axial slice at the level of stenosis. Pathognomonic finding for arterial dissection: intimal flap and double-lumen sign. a b c Fig. 3: Twenty-four year-old female with an acute episode of disorientation to time and place and expressive aphasia. (a) FLAIR: right lenticular and left temporo-parietal hyperintense lesions. (b) Diffusion and (c) ADC Map: show only acute ischemic lesions with cytotoxic edema and restricted diffusion (hyperintensity in diffusion and decreased ADC value). Lab: positive anti-nuclear antibodies and lupus anticoagulant and anticardiolipin antibodies. Antiphospholipid Syndrome. RESULTS Of the 30 patients, half were men with a mean age of 35 years. The cause of stroke was established in 86% of the cases (n=26). According to the modified TOAST (Trial of ORG 10172 in Acute Stroke Treatment) classification criteria, 7% (n=2) had large- vessel atherosclerosis. Moderate primary hypertension and dyslipide- Página 2 mia were found as risk factors for this disease. In 10% of patients (n=3) stroke was associated with cardioembolism (2 with patent foramen ovale and 1 with atrial septal aneurysm). Diagnosis was performed with transthoracic echocardiography in 2 patients and required transesophageal echocardiography in 1 patient. In 27% of patients (n=8), the cause was arterial dis- RAR - Volumen 75 - Número 2 - 2011 María Belén Nallino et al. a b c Fig.4: Thirty-year old male with a history of migraine with aura and ergotamine overuse, who experienced vomiting and impaired consciousness during a migraine attack. (a,b,c) FSE T2: Multiple acute ischemic lesions in the posterior territory. hypertension, diabetes, smoking history, family history of ischemia, etc.) had to be analyzed and drug consumption had to be documented. In 46% of cases (n=14) the vertebrobasilar territory was involved: in 43%, the carotid territory was affected (n=13), in 7% the cause was venous thrombosis (n=2), and in 1 patient multiple territories were affected by vasculitis. DISCUSSION Fig. 5: Fifteen-year-old male with small right sylvian ischemia. Magnetic resonance angiography of intracranial vessels. Note the development of small collateral vessels in the Willis´ polygon (arrow), with the appearance of a “puff of smoke”, a pathognomonic finding for Moyamoya disease. section (5 in vertebral arteries, 1 in the basilar artery and 2 in the internal carotid arteries). Only one of the patients had a history of trauma. This pathology was the leading cause of stroke in our cases (Figs. 1 and 2). In 43% (n=13), etiologies were miscellaneous (3 migrainous infarctions, 2 with Moyamoya disease, 2 venous thromboses, 1 primary CNS vasculitis, 2 systemic vasculitis, 1 lupus vasculitis, 1 antiphospholipid syndrome and 1 vasospasm secondary to neurosurgery (Figs. 3, 4 and 5). In 4 patients (13%), the cause was undetermined, and only 3 of them were adequately studied (Fig. 6). For a study to be considered adequate, it had to include at least images of the brain, of intra- and extracranial and cardiac vascularization, routine lab testing, complete hematological tests, coagulation times and lipid profile. In addition, risk factors (blood RAR - Volumen 75 - Número 2 - 2011 Twelve percent of strokes occur in patients younger than 45 years old, and 45% of these strokes are ischemic (1) . Finding the etiology of an ischemic stroke in a young person is a true challenge for physicians (1, 2). The causes of stroke in young adults are widely diverse and these patients usually require more extensive and thorough diagnostic testing than older adults to determine the cause underlying ischemic infarction. This is particularly important, since many of the etiologies can be treated and their identification provides an opportunity to change their specific risk as a factor of relapse (1, 2, 3). Data from various studies indicate that approximately 20% of ischemic strokes in young adults are caused by the atherosclerotic occlusion of large arteries, 25% are due to non-atherosclerotic occlusive disease (dissections account for up to 10%-20% in some studies and Moyamoya disease also has a high incidence within this group – approximately 3.5%), and 17% are due to cardioembolism (mainly patent foramen ovale, atrial septal aneurysm, rheumatic disease and endocarditis), 3% are caused by perforating vessels disease, 5% by prothrombotic states and 10% are due to miscellaneous causes (including migraine, drug abuse and use of oral contraceptives). In 20%-30% of cases, the cause of stroke is undetermined and, if after a thorough study physicians do not come to a diagnosis, the stroke is said to be cryptogenic (4,5,6,7). Página 3 Ischemic stroke in young adults a b Fig. 6: Thirty-year-old female patient, with no previous history, with an episode of hemiparesis of the right arm and leg and aphasia with an onset time of less than 3 hours. CT perfusion maps (a) Mean Transit Time (b) Relative Cerebral Blood Volume, showing an area of penumbra (red line) with minimal necrotic tissue (yellow line). Thrombolysis was performed with good clinical outcome. Computed tomography (CT) and Magnetic Resonance (MR) are the most valuable tools for the diagnosis of stroke. Unenhanced CT, which is widely available, can help quickly identify early signs of ischemia (such as the hyperdense vessel sign and the loss of contrast between gray matter and white matter), and also rule out hemorrhage. Conventional MR imaging sequences can depict acute ischemic lesions within 6 hours after the onset of a neurological event. State-of-the-art diffusion MR imaging, which is based on the movement of water molecules, detects the presence of cytotoxic edema in areas of irreversible ischemic damage. These areas are characterized by restricted water diffusion and appear hyperintense on diffusion images with a decreased apparent diffusion coefficient. Diffusion has a high sensitivity (88%-100%) and specificity (86-100%) to detect areas of ischemia, even within 30 minutes of their occurrence. Multislice CT angiography and MR angiography of the intracranial and neck vessels allow visualization of the arterial tree in few minutes, in a non-invasive manner, searching the vascular pathology that triggered the acute neurological event. CT perfusion and MRI perfusion maps of Relative Cerebral Blood Flow, Relative Cerebral Blood Volume and Mean Transit Time predict the presence of penumbra (tissue that is potentially salvageable with adequate therapy) (8,9). In our series, in agreement with other papers, dissections were the main cause of stroke in young adults. Multislice CT angiography with multiplanar reconstruction, MR angiography of the neck vessels and MR T1-weighted sequences with fat saturation can demonstrate, with excellent resolution, pathognomonic findings of arterial dissection such as intimal Página 4 flap, double lumen, and the presence of irregular stenosis and of pseudoaneurysms (10,11,12). Among miscellaneous etiologies, we highlight stroke-associated migraine. Different papers have reported an association between migraine and the risk of stroke, especially in premenopausal women, women who smoke and women who use oral contraceptives. Classic migraine with aura may be a more powerful predictor of stroke than migraine without aura. Of the patients included in our study, 2 were women of 28 and 30 years of age and 1 was a 30-yearold man. All of them had a history of migraine with aura (13,14). Unlike findings reported in the literature, atherosclerosis was an infrequent cause of stroke in our population sample, and strokes of undetermined etiology accounted for a lower percentage than those reported in other studies. In our study, the sample is small and has selection bias. We think that multicenter, randomized and prospective studies are needed to analyze the causes, incidence and prognosis of stroke in young adults. CONCLUSION The role of neuroimaging in the workup of young adults with stroke includes confirmation of the ischemic nature of the lesion, determination of its location and extension, and a quick and non-invasive study of extra- and intracranial vessels. In this sense, multislice CT and high-field MRI provide high sensitivity and specificity. RAR - Volumen 75 - Número 2 - 2011 María Belén Nallino et al. References 8. 1. 2. 3. 4. 5. 6. 7. Bevan H, Sharma K, Bradley W. Stroke in young adults. Stroke 1990; 21:382-6. Ibiapina Siqueira J, Santos AC, Soraria Ramos Cabete F, Sakamoto A. Cerebral infarction in patients aged 15 to 40 years, Stroke 1996; 26:2016-9. Kristensen B, Malm J, Carlberg B, et al. Epidemiology and Etiology of Ischemic Stroke in Young Adults Aged 18 to 44 Years in Northern Sweden. Stroke 1997; 28:1702-9. Varona JF, Guerra JM, Bermejo F, Molina JA, Gomez de la Cámara A. Causes of ischemic Stroke in Young Adults, and Evolution of the Etiological Diagnosis over the Long Term. European Neurology 2007; 57:210-8. Khan FY. Risk factors of young ischemic stroke in Qatar. Clinical Neurology and Neurosurgey 2007; 109:770-3. Epub 2007 Aug 27. Chan MT, Nadareishvili ZG, Norris JW. Diagnostic Strategies in Young Patients with Ischemic Stroke in Canada. Can J Neurol Sci 2000; 27:120-4. Kimchi TJ, Agid R, Lee SK, Ter Brugge KG. Arterial Ischemic RAR - Volumen 75 - Número 2 - 2011 9. 10. 11. 12. 13. 14. Stroke in Children. Neuroimag. Clin N Am 2007; 17:175-87. Srinivasan A, Goyal M, Al Azri F, Lum C. State-of-the-Art Imaging of Acute Stroke. Radiographics 2006; 26: S75-S95. Uggetti C. Stroke in young people: imaging. Neurol Sci 2003; 24:S15-S16. Flis, CM Jâger HR, Sidhu PS. Carotid and vertebral dissections: clinical aspects, imaging features and endovascular treatment. Eur Radiol 2007; 17: 820-34. Rodallec MH, Marteau V, Gerber S, Desmonttes L, Zins M. Craniocervical Arterial Dissection: Spectrum of Imaging Findings and Differential Diagnosis. Radiographics 2008; 28: 1711-28. Vertinsky AT, Schwartz NE, Fischbein NJ, Rosenberg J, Albers GW, Zaharchuk G. Comparison of Multidetector CT Angiography and MR Imaging of Cervical Artery Dissection. AJNR Am J Neuroradiol 2008; 29: 1753-60. Bousser MG, Welch MA. Relation between migraine and stroke. Lancet Neurol 2005; 4:533-42. Kurth T, Gaziano JM, Cook NR, Logroscino G, Diener HC, Buring JE. Migraine and risk of cardiovascular disease in women. JAMA 2006; 296: 283-91. Página 5