things i don`t want to forget
Anuncio

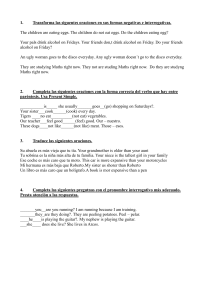
NAME: DATE: PROVIDER: THINGS I WANT TO REMEMBER What are the most important things I would like to talk about at my visit today? (provider: check if discussed) 1. ____________________________________ ____________________________________ ____________________________________ 2. ____________________________________ ____________________________________ ____________________________________ 3. _____________________________________ _____________________________________ _____________________________________ Anything else: _____________________________________ _____________________________________ _____________________________________ Examples: -Symptoms -Lab results -Referrals -Medications -Side effects -Concerns -Forms -Diet -Excercise For MA: Patient needs help to fill out? No Yes ------>Time spent for form_____mins. NAME: DATE: PROVIDER: COSAS QUE QUIERO RECORDARME ¿Cuáles son las cosas más Importantes que quiero hablar en mi visita de hoy? (provider: check if discussed) 1. ____________________________________ ____________________________________ ____________________________________ 2. ____________________________________ ____________________________________ ____________________________________ 3. _____________________________________ _____________________________________ _____________________________________ ¿Algo más? _____________________________________ _____________________________________ _____________________________________ Ejemplos: -Síntomas -Resultados de laboratorio -Medicinas -Necesidades Familiares -Efectos Segundarios - Referencias -Dieta -Ejercicio For MA: Pt. needs help to fill out? No Yes ------->Time spent for form_____mins.