Thoracic osteochondroma with spinal cord
Anuncio

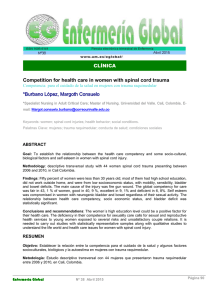
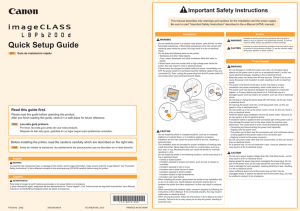
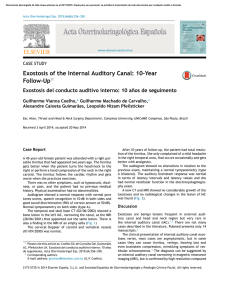
Thoracic osteochondroma with spinal cord compression 1. Vaquero; R. Martínez; J. C. Gómez-Angulo and P. Aragonés Service of Neurosurgery. Puerta de Hierro Clinic. Autonomous University. Madrid Summary «familial osteochondromatosis», and «hereditary multipIe exostoses».(1.7.12.16) A case of osteochondroma at T5 level, impinging on The cause of hereditary multiple osteochonthe spinal cord in a patient previously diagnosed of dromatosis is unknown, males are predominantly, and is presented. Spinal el 21/11/2016. hereditary osteochondromatosis, Documento descargado de http://www.revistaneurocirugia.com Copia para uso personal, se prohíbe la transmisión de este documento por cualquier m malignant neoplastic transformation occur in 5 % to compression is an infrequent event in the course of this 25 % of patients. (1.3, 6, 7, 9. 13-17) disease. Nevertheless, one must consider this possibility Osteochondromas usually arise at the end of long in the follow-up of the patients with this relatively combones, but they can involve the spine in 7% of the mon bone dysplasia. cases,'3) and although has been reported that spinal osteochondromas are 10cated mainly at the thoracic and KEY WORDS: Osteochondroma, Spinal cord, Spine. lumbar areas,(l3) a recent review of 94 cases of spinal osteochondromas showed that 39 % arose in the cervical spine, 28% in the lumbar spine, 29% in the thoracic spine, and 3% in the sacrum.(14) In any case, Resumen neurological complications due to spinal cord compression are rare,<2· 4.8,12.13.15,17) appearing in 0,5% of the paSe presenta un caso de osteocondroma espinal, a nivel tients, roughly(l2) T5, en una paciente previamente diagnosticada de In the present report, we describe a case of thoracic osteocondromatosis hereditaria. Aunque la aparición de spinal cord compression due to an osteochondroma, un cuadro de compresión medular por osteocondromas in a patient with hereditary multiple osteochonraquídeos es relativamente infrecuente en el curso de la dromatosis. osteocondromatosis hereditaria, su posibilidad debe ser tenida en cuenta en el control evolutivo de los pacientes con esta displasia ósea. Case report PALABRAS CLAVE: Osteocondroma, Médula espinal, Raquis. Introduction Multiple osteochondromatosis is a relatively common bone dysplasia which is usually hereditary. According to O'Connor and Roberts (12) it was first described by Stanley in 1849. Later, this entity was extensively reviewed by Ehrenfried, in 1917,(5) who called the process «hereditary deforming chondrodysplasia». It also has been designated as «diaphyseal aclasis», «multiple cartilaginous exostoses», This 29-year-old woman had been previously diagnosed of hereditary multiple osteochondromatosis. She was hit in the back approximately 18 months prior to admission. Initially, she suffered back pain, but the symptoms gradually progressed to pain radiating to the mid-scapular region, and weakness of both legs developed. Neurological exarnination showed muscle strenght of 4/5 on both legs. Her reflexes were hyperreactives on both legs, and Babinski sign was present bilaterally. Plain spine X-ray showed a lesion at the right side of the T5 vertebral body that suggested an ostochondroma. Numerous osteochondromas were radiologically disclosed at the ribs and left wrist. Myelography and 125 Neurocirugía Thoracic osteochondroma with spinal cord compression subsequent CT-scan showed a calcified mass impinging on the spinal cord (Figo 1 and 2)0 The lesion was originated in the head of the right rib at TS level. MRI study confirmed the lesion, impinging on the spinal cordo The tumor was hypointense, with zones of increased signal on T2-weighted images (Fig. 3). The patient underwent surgery via a posterior approach to the thoracic spine; through a laminectomy a mostly calcified epidural tumor was removed by drill- Documento descargado de http://www.revistaneurocirugia.com el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier m Fig. 2.-CT-scan after myelography, showing the tumor within the spinal canal and the spinal cord compression. Fig. 3.-Magnetic Resonance, showing the hypointense tumor, with areas of hyperintense signal, on T2 weighted images. Fig. l.-Myelographic study with intratecal metrizamide, showing the calcified tumor and the spinal cord compression (arrows). Discussion ing. The postoperative course was unremarkable, and she returned home within one week. Pathological study showed hyaline cartilage, bone and marrow with fat tissue (Fig. 4)0 A diagnosis of osteochondroma was establishedo 126 Recently, a case of osteochondroma of the thoracic spine was reported by Roblot et al.(14) and after an excellent review of the literature, these authors collect on1y 94 previous cases of spinal osteochondroma. According to this review also, osteochondromas are rarely Thoracic osteochondroma with spinal cord compression Neurocirugía seen on the spine, and this localization represents between Many authors consider osteochondromas as 2,5 % and 3,3 % of the localizations of osteochondromas. developmental anomalies rather than true tumors. These Nevertheless, osteochondromas represent 7,6 % of the lesions begin in early childhood, and they grow at the benign cartilaginous neoplasms of the spine. (14) same time as the host bone until the nearest epiphyseal center ossifiesY' 12) Nevertheless, it is obvious that, in Our present case is added to the previous reports about spinal cord compression in hereditary osteochondromasorne cases, osteochondromas with spinal involvement may produce spinal cord compression. They usually tosis. In our patient, the osteochondroma arose from become symptomatic during the 2nd or 3rd decades, (8) the head of a rib, and caused spinal cord compression. Pathologically, osteochondromas occur within the like in our present case. Surgical removal usually obperiosteum of bones with endochondral ossification, tains excellent clinical results in these patients. and usually grow progressively by endochondral ossification of their cartilaginous caps. They are surrounded by a thin layer of hyaline cartilage, and References covered by the periosteum of the parent bone. (1, 7) The 1. AERGERTER, E.; K!RKPATRICK, 1. A.: Orthopaedíc Díseases, ed most part ofDocumento the tumor is composed of cancellous bone 4. Philadelphia. WBpersonal, Saunders, 1975, lapp. 121-128.de este documento por cualquier m descargado de http://www.revistaneurocirugia.com el 21/11/2016. Copia para uso se prohíbe transmisión 2. BUCKLER, R. A.; CHAO, D. A.; SMITH, T. W.; DAVIDSON, R. I.: interspersed with marrow. (1, ll) In our case microscopical SCIATICA: An early manifestation of thoracic vertebral osteochondroma. study disclosed a great amount of fat within the marNeurosurgery, 1987; 21:98-100. 3. CARMEL, P. W.; CRAMER, F. J.: Cervical cord compression due row, and this fact led us to explain the increase signal to exostosis in a patient with hereditary multiple exostoses. Case report within the tumor on MRI images. J. Neurosurg. 1968; 28:500-503. Fig. 4.-Histological aspect ofthe resected tumor, showing cartilage, bone, and marrow wíth fat cells. H. E. techníque, original magnification x250. As previously reported cases of spinal osteochondroma have demonstrated, CT-scan is useful for establishing the origin of the lesion and for delineating the tumor from the spinal cord. (2,8, 10,13,14) In 75 % of patients with multiple osteochondromatosis a strong familial inheritance is disclosed, and when farnily trees are studied, a clear predominance of males is present. (12,14) A single autosomal-dominant gene may be responsible for the clinical disease in heterozygote patients while it could be suppressed by an independently segregated autosomal-dominant gene, this gene would be frequently latent in females, and this could be the reason by which the sex ratio líeavily favours the males. (9,12) 4. CHIURCO, A. A.: Multiple exostoses of bone with fatal spinal cord compression. Report of a case and review of the literature. Neurology, 1970; 20:275-278. 5. EHRENFRIED, A.: Hereditary deforming chondrodysplasiamultiple cartilaginous exostoses. A review of the American literature and report of twelve cases. JAMA, 1917; 68:502-508. 6. FIELDING, 1. W.; RATZAN, S.:Osteochondroma of the cervical spine, J. Bone Joint, Surg. (Am) 1973; 55: 640-641. 7. JAFFE, M. L.: Tumors and Tumorous Conditions of Bones and ¡omts. Philadelphia, Lea and Febiger, 1958, pp. 150-165. 8. KARIAN, J. M.; DEFILIPP, G.; BUCHHEIT, W. A.; BONAKDARPUR, A.; ECKHARDT, W.: Vertebral osteochondroma causing spinal cord compression: Case report, Neurosurgery, 1984; 14:483-484. 9. KROOTH, R. S.; MACKLIN, M. T.; HILBISH, T. F.: Diaphysial aclasis (multiple exostoses) on Guam. Am. J. Hum. Genet. 1961; 13:340-347. 10. LOFTus, C. M.; ROZARlO, R. A.; PRAGER, R.; SCOTT, R. M.: Solitary osteochondroma of T4 with thoracic cord compression. Surg. Neurol. 1980; 13:355-357. 11. MAC CEE, E. E.: Osteochondroma of the cervical spine: a cause of transient quadriplegia. Neurosurgery, 1979; 4:259-260. 12. O'CONNOR, G. A.; ROBERTS, T. S.: Spinal cord compression by an osteochondroma in a patient with multiple osteochondromatosis. J. Neurosurg. 1984; 60:420-423. 13. PALMER, F. J.; BLUM, P. W.: Osteochondroma with spinal cord compression: Report of three cases. J. Neurosurg. 1980; 52:842-845. 14. ROBLOT, P.; ALCALAY, M.; CAZENAVE-RoBLOT, F.; LEVY, P.; BONTOUX, D.: Osteochondroma of the thoracic spine. Report of a case and review of the literature. Spine, 1990; 15:240-243. 15. SLEPIAN, A.; HAMBY, W. B.: Neurologic complications associated with hereditary deforming chondrodysplasia. Review of the literature and report on two cases occurring in the same family. 1. Neurosurg. 1951; 8:529-535. 16. TUREK, S. L.: Orthopedics, ed 3. Philadelphia. J. P. Lippincott, 1977, pp. 321-322. 17. VINSTEIN, A. L.; FRANKEN, E. A. JR.: Hereditary multiple exostoses. Report of a case with spinal cord compression. Am. J, Roentgenol. 1971; 112:405-407. Vaquero, J.; Martínez, R.; Gómez-Angulo, J. C. and Aragonés, P.: Thoracic osteochondroma with spinal cord compression. Neurocirugía, 1991; 2: 125-127.