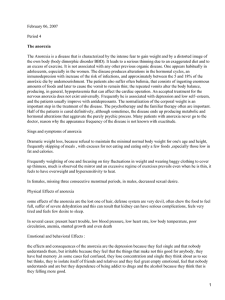
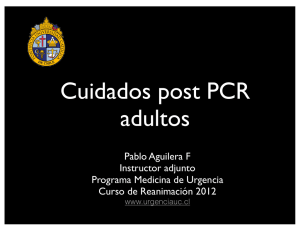
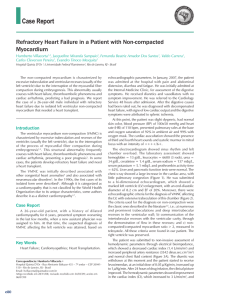
Vervoort et al Miscellaneous Global cardiac surgery: Access to cardiac surgical care around the world Dominique Vervoort, MD,a Bart Meuris, MD, PhD,b Bart Meyns, MD, PhD,b and Peter Verbrugghe, MD, PhDb ABSTRACT Methods: A scoping review was done on access to cardiac surgery for an undifferentiated population. Workforce data were collected from the Cardiothoracic Surgery Network database and used to calculate numbers and ratios of adult and pediatric cardiac surgeons to population. Results: A total of 12,180 adult cardiac surgeons and 3858 pediatric cardiac surgeons were listed in the Cardiothoracic Surgery Network in August 2017, equaling 1.64 (0-181.82) adult cardiac surgeons and 0.52 (0-25.97) pediatric cardiac surgeons per million population globally. Large disparities existed between regions, ranging from 0.12 adult cardiac surgeons and 0.08 pediatric cardiac surgeons per million population (sub-Saharan Africa) to 11.12 adult cardiac surgeons and 2.08 pediatric cardiac surgeons (North America). Low-income countries possessed 0.04 adult cardiac surgeons and 0.03 pediatric cardiac surgeons per million population, compared with 7.15 adult cardiac surgeons and 1.67 pediatric cardiac surgeons in high-income countries. Conclusions: This study maps the current global state of access to cardiac surgery. Disparities exist between and within world regions, with a positive correlation between a nation’s economic status and access to cardiac surgery. Low early mortality rates in low-resource settings suggest the possibility of high-quality cardiac surgery in low- and middle-income countries. There is the need to increase human and physical resources, while focusing on safety, quality, and efficiency to improve access to cardiac surgery for the 4.5 billion people without. (J Thorac Cardiovasc Surg 2019;-:1-10) Cardiovascular disease (CVD) is the leading cause of death in the world, accounting for approximately 17.5 million deaths worldwide every year, of which 80% occur in lowand middle-income countries.1 This burden is increasing because of the epidemiologic transition from From the aProgram in Global Surgery and Social Change, Harvard Medical School, Boston, Mass; and bDepartment of Cardiac Surgery, UZ Leuven, Leuven, Belgium. Received for publication Nov 11, 2018; revisions received April 2, 2019; accepted for publication April 10, 2019. Address for reprints: Dominique Vervoort, MD, Program in Global Surgery and Social Change, Harvard Medical School, 641 Huntington Ave, 02115 Boston, MA (E-mail: vervoortdominique@hotmail.com). 0022-5223/$36.00 Copyright Ó 2019 by The American Association for Thoracic Surgery https://doi.org/10.1016/j.jtcvs.2019.04.039 Cardiac surgeon density worldwide exacerbates disparities in access to cardiac surgery. Central Message Some 4.5 billion people lack access to cardiac surgery when needed. Availability of adult and pediatric cardiac surgical workforce is scarce in low- and middle-income countries, and disparities are widespread. MIS Objective: Cardiovascular disease is the leading cause of death worldwide, responsible for 17.5 million deaths every year, of which 80% occur in low- and middle-income countries. Some 75% of the world does not have access to cardiac surgery when needed because of lack of infrastructure, human resources, and financial coverage. This study aims to map access to cardiac surgery around the world. Perspective Global cardiac surgery addresses the lack of cardiac surgical care for the majority of the world. CVDs remain the leading cause of mortality globally, with surgical conditions such as rheumatic and congenital heart disease significant in low- and middle-income countries. Knowing the availability of specialist cardiac surgical workforce allows for targeted policy interventions. See Commentary on page XXX. communicable to noncommunicable diseases in low- and middle-income countries, with CVD and stroke mortality increasing rapidly. Despite the high prevalence of CVD in low- and middle-income countries, exact, high-quality data and imaging are scarce, thus potentially underestimating the true global state. Scanning this QR code will take you to the article title page to access supplementary information. The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 1 Miscellaneous Abbreviations and Acronyms CTSNet ¼ Cardiothoracic Surgery Network CVD ¼ cardiovascular disease DALY ¼ disability-adjusted life-year GDP ¼ gross domestic product NGO ¼ nongovernmental organization RHD ¼ rheumatic heart disease MIS Surgery has recently been recognized as an integral part of national health systems, yet approximately 5 billion people remain without timely access to safe and affordable surgical care when needed.2 More than 17 million people die of surgically preventable conditions every year, and only 6% of the 313 million surgical interventions taking place every year occurs in the poorest one-third of the world’s population, in whom the need for surgical care is highest. Unlike previous misconceptions about the costs of investing in surgical systems, emergency and essential surgical services are cost-effective on an individual and macro-economic level.2 Global cardiac surgery can be defined as an area for study, research, practice, and advocacy that places priority on improving health outcomes and achieving health equity for all people worldwide who are affected by cardiac surgical conditions or have the need for cardiac surgical care.3 In sub-Saharan Africa, excluding South Africa, there is only 1 cardiac surgery center per 38 million inhabitants.4 In Asia, there is only 1 per 25 million. In contrast, North America and Europe have 1 per 120,000 people.5 For cardiothoracic surgeons, a similar maldistribution follows gross domestic product (GDP) differences: With 27 and 28 cardiothoracic surgeons per million population, North America and Western Europe have 42% and 32% of the world’s capacity, respectively. Africa, with only 1 cardiothoracic surgeon per 4 million population, accounts for only 1% of the total global capacity.6 On a population level, ready access to cardiothoracic surgery is proportional to the economic status of the patient. As a result, approximately 4.5 billion people do not have access to cardiac surgery.7 In low- to middle-income countries, rheumatic heart disease (RHD) and congenital heart disease are the most common CVDs requiring surgical care. RHD affects 33.4 million people worldwide, yet 97% occurs in low- and middle-income countries and indigenous populations in high-income countries.8 In low-income countries, only 11% of patients undergo operation, underlining the fact that RHD is a disease of social injustice.9 Recently, the Cape Town Declaration on Access to Cardiac Surgery in the Developing World was released as an attempt to unite all stakeholders to tackle the global burden of RHD.10 Meanwhile, congenital heart disease affects 1 million babies or 1 in 125 live births per year, of which approximately 2 Vervoort et al 70% will require medical or surgical treatment in the first year of life.11 Some 90% are denied treatment or receive suboptimal care, and up to 80% of cases are not diagnosed until advanced or irreversible stages of heart failure.12 With treatment, 85% of cases are expected to survive to adult life. Without treatment, 1 in 3 babies will die within their first month.13 The remaining patients are faced with multiple complications, including frequent pulmonary infections, bacterial endocarditis, irreversible pulmonary changes, myocardial fibrosis, neurologic events, increased operative risks, and an impaired functional status. In lowto middle-income countries, 66% of preventable deaths and 58% of disability-adjusted life-years (DALYs) due to congenital malformations are related to congenital heart defects, which could be averted by scaling up surgical care.14 In sub-Saharan Africa, CVD is responsible for 45 per 1000 DALYs, compared with 15 per 1000 for trauma.15,16 Although the cost-effectiveness of cardiac surgical care in low- and middle-income countries has not been studied widely, a recent cost-effectiveness analysis has proposed favorable cost-effectiveness of pediatric cardiac surgery in low- and middle-income countries ($171 per DALY averted) compared with other surgical (eg, trauma centers: $100-300 per DALY averted) and public health interventions (eg, antiretroviral therapy for human immunodeficiency virus: $800-1000 per DALY averted).17,18 Overall, the pediatric population in low- and middleincome countries has a higher incidence and prevalence of cardiac diseases requiring surgical care than children in industrialized countries.19 Developed countries are estimated to require 1 cardiac center performing 300 to 500 pediatric cardiac surgeries per year per 2 million population, whereas low- and middle-income countries are estimated to require 1 per 1 million population, although the exact need is still unknown.19 Nevertheless, many countries with populations up to 70 million people still remain without a single pediatric cardiac center. As a result, an estimated 15 million children die or become debilitated annually by potentially treatable or preventable cardiac diseases.19 With 47% of the population in sub-Saharan Africa being younger than 15 years old, global upscaling of pediatric cardiac surgery is highly needed. This study attempts to map the current global cardiac surgery capacity, to support health system strengthening, and to establish a framework to develop sustainable programs to scale up access to cardiac surgery on a global level. MATERIALS AND METHODS Literature Search A scoping review was done to identify quantitative data and descriptive studies on access to cardiac surgical care with a focus on cardiac surgical workforce, infrastructure, capacity, and quality. Literature searches were performed between August 1, 2018, and October 1, 2018, in the medical database PubMed using the search string below to identify articles describing the state of and disparities in accessing cardiac surgical care The Journal of Thoracic and Cardiovascular Surgery c - 2019 Vervoort et al Miscellaneous Search String The search string was as follows: ("Cardiac Surgical Procedures"[mh] OR "cardiac surgery"[tiab] OR "cardiothoracic surgery"[tiab] OR "heart surgery"[tiab] OR "interventional cardiology"[tiab] OR "interventional cardiology"[mh]) AND ("humanitarian"[tiab] OR "low-income"[tiab] OR "low income"[tiab] OR "middle-income"[tiab] OR "middle income"[tiab] OR "developing country"[tiab] OR "developing countries"[tiab] OR "developing nation"[tiab] OR "developing nations"[tiab] OR "developing world"[tiab] OR "Africa"[tiab] OR "Africa"[mh] OR "developing countries"[mh] OR "relief work"[mh] OR "global health"[mh]) NOT (Comment[ptyp] OR Editorial[ptyp] OR Letter[ptyp] OR Case Reports [ptyp] OR News[ptyp]). Data Identification Countries are stratified as defined by the World Bank regions: East Asia and Pacific, Europe and Central Asia, Latin America and the Caribbean, Middle East and North Africa, North America, South Asia, and subSaharan Africa. On the basis of the World Bank income groups, countries are further divided in low-, middle-, and high-income countries. Records identified through database searching (n = 903) Numbers of adult and pediatric cardiac surgeons per country were independently obtained from the registry of the Cardiothoracic Surgery Network (CTSNet, http://www.ctsnet.org) in August 2017 and checked for duplicates. The CTSNet database is overseen by the Society of Thoracic Surgeons, the American Association for Thoracic Surgery, and the European Association for Cardio-Thoracic Surgery and includes the membership registries of 29 cardiothoracic surgical societies from around the world. Cardiac surgeons not affiliated with these societies are invited, but not obliged, to join CTSNet independently. Pediatric cardiac surgeons were also registered as adult cardiac surgeons in the database, but no information on caseload or operative focus was available. The collected data were used to calculate numbers and ratios of adult and pediatric cardiac surgeons to population. Although available data did not provide details on surgeons practicing abroad, they demonstrate approximate densities of cardiac surgeons around the world. Pure thoracic or vascular surgeons registered with CTSNet and cardiac surgeons who were indicated to have retired were excluded. A sample of the data from low-, middle-, and highincome countries was validated against external data, including a subset analysis for English-speaking versus non–English-speaking countries (Appendix E1). RESULTS Literature Search Of the 903 identified articles, 15 were included in the study (Figure 1). The main findings are summarized in the Table E1. Additional records identified through other sources (n = 2) Eligibility Records screened (n = 896) Full-text articles assessed for eligibility (n = 34) Included Screening Records after duplicates removed (n = 896) Studies included in qualitative synthesis (n = 15) Records excluded (n = 862) Full-text articles excluded, with reasons (n = 19) (Personal and regional perspectives n = 19, editorial n = 4, letter n = 1) FIGURE 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 3 MIS in low- and middle-income countries. There were no restrictions to language or publication status. Commentaries, editorials, letters, and case reports were excluded. Articles describing novel procedures, outcomes, personal experiences, or perspectives; articles that are not related to cardiac surgery or interventional cardiology; and articles more than 20 years old (published before 1998) were excluded. Miscellaneous MIS Adult Cardiac Surgeons A total of 12,180 adult cardiac surgeons were listed in the CTSNet registry, which translates to 1 adult cardiac surgeons per 0.61 million people globally, or, conversely, 1.64 adult cardiac surgeons per million people (Figure 2). Regional distribution ranged from 11.12 adult cardiac surgeons per million population (32.82% of total) in North America to 0.12 adult cardiac surgeons per million (1.05% of total) in sub-Saharan Africa (Figure 3). Furthermore, large disparities were found within regions. In subSaharan Africa, no cardiac surgeon in the Democratic Republic of the Congo and Ethiopia was registered for a population of 78.7 million and 102.4 million people, respectively. The other regional spectrum was South Africa, with 58 adult cardiac surgeons for a population of 55.9 million people, or 1.04 adult cardiac surgeons per million population. In contrast, the United States had 11.54 adult cardiac surgeons per million, whereas the highest density was found in Monaco, with 181.82 adult cardiac surgeons per million (7 adult cardiac surgeons covering 38,500). Similar disparities existed when dividing countries per income group (Figure 3). Low-income countries possessed 0.04 adult cardiac surgeons per million population, compared with 7.15 adult cardiac surgeons per million people in high-income countries. Regional distribution of adult cardiac surgeons was correlated with GDP per capita, with sub-Saharan Africa ($1450 GDP per capita) on the lower end of the spectrum, and North America ($55,928 GDP per capita) on the higher end of the spectrum (Figure 4). Vervoort et al Pediatric Cardiac Surgeons A total of 3858 pediatric cardiac surgeons were registered in the CTSNet database, equaling 0.52 pediatric cardiac surgeons per million population (Figure 5). Disparities in distribution of pediatric cardiac surgeons were similar to those for adult cardiac surgeons, ranging from a minimum of 0.08 pediatric cardiac surgeons per million population (2.20% of total) in sub-Saharan Africa to 2.08 pediatric cardiac surgeons per million (19.37% of total) in North America. On a country level, registered numbers varied from no pediatric cardiac surgeons in Ethiopia (102.4 million people) and the Democratic Republic of the Congo (78.7 million people) to 2.12 per million population in the United States and the United Kingdom, with Monaco (1 pediatric cardiac surgeons for 38,500 people, or 25.97 per million) at the higher end of the spectrum. Based on income groups, distribution ranged from 0.071 pediatric cardiac surgeons per million in low-income countries up to 9.505 pediatric cardiac surgeons per million in high-income countries (Figure 3). Similar to adult cardiac surgeons, lower and upper middle-income countries did not significantly differ from each other in the numbers of pediatric cardiac surgeons per population. Regional distribution of pediatric cardiac surgeons was also correlated with GDP per capita (Figure 4). When adjusting for the pediatric (<15 years old) population, there were 1.99 pediatric cardiac surgeons per million population. Sub-Saharan Africa and South Asia possessed 0.19 and 1.16 pediatric cardiac surgeons per million FIGURE 2. Adult cardiac surgeons per million population registered with the CTSNet in August 2017 (n ¼ 12,180). Map created at www.mapchart.net. CTSNet, Cardiothoracic Surgery Network. 4 The Journal of Thoracic and Cardiovascular Surgery c - 2019 Vervoort et al Miscellaneous 8 7 6 5 4 3 2 1 0 Lower Middle-Income Countries Upper Middle-Income Countries ACS High-Income Countries PCS FIGURE 3. Adult and pediatric cardiac surgeons per million population for the different World Bank Income Groups registered with the CTSNet in 2017. ACS, Adult cardiac surgeon; PCS, pediatric cardiac surgeon. population, respectively, compared with 11.1 and 6.28 pediatric cardiac surgeons per million population in North America and Europe and Central Asia. Disparities of pediatric cardiac surgeons distribution between regions are more apparent when adjusting for pediatric population, with a difference in density of pediatric cardiac surgeons per million population of factor 25.3 between North America and sub-Saharan Africa, running up to a difference factor of 57.9 between North America and sub-Saharan Africa for pediatric cardiac surgeons per million population aged less than 15 years. These differences can be due to higher relative pediatric populations in sub-Saharan Africa (42.88% of total population) compared with North America (18.72% of total population). 100000 10000 1000 100 10 1 0.1 Sub-Saharan Africa South Asia Middle East & Latin America & Caribbean North Africa East Asia & Pacific Europe & Central Asia North America 0.01 GDP per capita (in USD) Adult cardiac surgeons per million population Pediatric cardiac surgeons per million population FIGURE 4. Regional correlation between GDP per capita and distribution of adult and pediatric cardiac surgeons registered with the CTSNet in 2017. GDP, Gross domestic product. The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 5 MIS Low-Income Countries Miscellaneous Vervoort et al FIGURE 5. Pediatric cardiac surgeons per million population registered with the CTSNet in August 2017 (n ¼ 3858). Map created at www.mapchart.net. CTSNet, Cardiothoracic Surgery Network. MIS Data validation highlighted valid data for the majority of sampled countries not covered by societies participating in CTSNet. Data validity was comparable across countries from different income groups and countries with official languages other than English (Appendix E1). Cardiac Centers Several low- and middle-income countries have established cardiac surgical centers of excellence for their country or region in an attempt to effectively centralize the scarcely available resources. These dedicated centers of excellence form centralized hubs providing clinical, educational, research, and administrative support to local cardiac centers in their respective regions, as well as direct domestic and foreign patient care. In the Asian region, centers of excellence exist in Malaysia, Singapore, South Korea, Japan, Australia, and New Zealand, supporting neighboring and nearby countries lacking (complex) cardiac surgical care. If restarted, Ghana (5 centers) and Nigeria (7 centers) could provide West Africa with 12 centers covering a population of 376.3 million people.4 Likewise, in the next 20 years, the 12 centers in East Africa (Kenya, Rwanda, Tanzania, and Uganda), 2 centers in Southern Africa (Mozambique, Namibia), and 2 centers in Eritrea and Ethiopia could aim at performing at least 30 open surgeries per million people.4 However, disparities may exist within countries. For example, the availability of cardiac surgical care in China is particularly prominent in the East of the country (eg, Beijing and Shanghai), whereas availability thereof in the West is scarce.20 Likewise, many countries only have centers in 6 the capital, limiting access to care for patients living far away.21 DISCUSSION Global surgery is a relatively new field, and subspecialization with a focus on specific surgical subdisciplines is limited. This study is a comprehensive review of the global state of access to cardiac surgery. Tables 1 and 2 provide a summary of the current state and ways forward for cardiac surgery in low- and lower middle-income, upper middleincome, and high-income countries. CVDs have a 32% chance of requiring a surgical intervention in low- and middle-income countries.22 However, 93% of the population in low- and middle-income countries do not have access to cardiac surgery, leaving approximately 2.5 million people in need of cardiac surgery untreated. Although costs for cardiac surgery are lower in low- and middle-income countries, open surgery is relatively expensive as GDP per capita income is low compared with high-income countries.23 Generally, low- and middleincome countries do not possess universal health coverage packages, and thus rely on sponsoring or out-of-pocket payments. If open surgery is not performed in that country, costs are even higher, requiring surgery abroad. In the Pacific region, island nations spend between 4% and 12% of their total health budget on sending patients with RHD to other countries for the needed surgery.24 Patients without health insurance have to find alternate sources of financing to meet surgical costs, including borrowing from friends and relatives, and pledging or selling assets such as their property.25 The Journal of Thoracic and Cardiovascular Surgery c - 2019 Vervoort et al Miscellaneous Income group Burden of cardiac disease Workforce Infrastructure and medicines Access to care Low- and lower middle-income countries High burden of RHD Unmet burden of CHD, CMP, EMF Growing burden of IHD (epidemiologic transition) Low density or absence of cardiac surgeons and anesthesiologists No or few cardiac surgery residency and fellowship programs Shortages of ancillary staff Low numbers or complete absence of cardiac centers Frequent stockouts of essential medicines and anticoagulation Lack of (functional) equipment (eg, electrocardiograph) Limited or no health insurance coverage for cardiac surgery Long waiting lists where cardiac centers exist High relative costs for patient, if surgery performed Upper middle-income countries Lower, rural or poverty-linked burden of RHD Lower unmet burden of CHD, CMP Growing burden of IHD (epidemiologic transition) Low density of cardiac surgeons and anesthesiologists No or few cardiac surgery residency and fellowship programs Shortages of ancillary staff Inadequate numbers and distribution of cardiac centers Few stockouts of essential medicines and anticoagulation Limited (functional) equipment (eg, CT scan) Public (universal) or private health insurance coverage for cardiac surgery Long waiting lists High relative costs for patient, if surgery performed High-income countries Absence of RHD Met burden of CHD, CMP High burden of IHD Adequate numbers of cardiac surgical workforce Adequate numbers of cardiac surgery residency and fellowship programs Adequate numbers and distribution of cardiac centers Availability of essential medicines and anticoagulation Adequate availability of functional equipment Public (universal) or private health insurance coverage for cardiac surgery Short to medium waiting lists Low or high relative costs for patient RHD, Rheumatic heart disease; CHD, congenital heart disease; CMP, cardiomyopathy; EMF, endomyocardial fibrosis; IHD, ischemic heart disease; CT, computed tomography. In most countries, healthcare expenditure, including the growth of cardiac surgery, parallels GDP. High-income countries spend an average of 11.8% of GDP on health, compared with just 5.8% of GDP in low- and middleincome countries, severely restricting health services to essential priorities in those countries.26 Despite lacking sufficient access to cardiac surgery services, delivery thereof has proven to be as effective and efficient as high-income countries. For example, the Narayana Hrudayalaya Heart Hospital in India provides cost-effective and high-quality cardiac surgical care in India, including in areas without established programs.27 Early mortality of pediatric cases operated on by visiting teams in sub-Saharan Africa ranged from 2% to 4%.4 Outcomes in Samoa, Fiji, Pakistan, Cambodia, and Mozambique further show that early mortality rates after open surgery in low-resource settings can be low and comparable to outcomes in the rest of the world, suggesting the possibility of performing high-quality cardiac surgery in low- and middle-income countries.24,28,29 In an attempt to bridge the gap in existing fragile health systems, humanitarian efforts have led 77 nongovernmental organizations (NGOs) to develop cardiac surgical programs in low- and middle-income countries.30 These programs range from overseas treatment to fly-in fly-out missions. However, no comprehensive quality control or impact assessment is in place to evaluate the benefit or harm introduced by surgical NGOs. It is important to recognize that some fly-in fly-out organizations may not take into account the postoperative care of patients, leaving a setting after operating without knowledge of follow-up care or availability and monitoring of anticoagulation. We propose the adoption of capacity-building programs for local care teams and the establishment of sustainable preoperative and postoperative frameworks to enable timely, quality, and holistic cardiac care. NGOs increasingly collaborate with each other, whereas the European Union reaches out to Eastern Europe and former colonies.31 Likewise, China, India, Mexico, Brazil, and Russia have developed satellite programs in rural areas, ensuring widespread upscaling around the world.5 Maghreb countries have taken the lead in open surgery in the African region, which could inspire sub-Saharan African countries to follow the example.4 Twinning programs pair 2 cardiac programs in the world, an established center of excellence and an evolving program, to teach cardiac surgery locally.31 As a result, Mozambique, Sudan, and Ethiopia have seen open surgery introduced through collaborative programs between local institutions and NGOs from Europe and North America. We mapped existing disparities between and within regions with regard to cardiac surgeons based on data available by CTSNet. Relative shortages are highest in subSaharan Africa, with 0.12 adult cardiac surgeons per million population and 0.19 pediatric cardiac surgeons per million pediatric population. In comparison, North America possesses 11.12 adult cardiac surgeons per million The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 7 MIS TABLE 1. Current state of the provision of cardiac surgical care in low-, lower middle-, upper middle-, and high-income countries Miscellaneous Vervoort et al TABLE 2. Proposed way forward for low-, lower middle-, upper middle-, and high-income countries in the provision of cardiac surgical care Infrastructure and medicines MIS Income group Burden of cardiac disease Workforce Access to care Low- and lower middle-income countries Increased surveillance of rheumatic fever, RHD, CHD, and other cardiac diseases Introduce public campaigns and patient counseling to empower lifestyle changes to reduce IHD Expand South-South partnerships Regulate task-sharing for nonsurgical care (eg, nurse anesthetist) Establish or increase national or regional cardiac surgery residency and fellowship programs Train ancillary health staff Establish fewer, but highvolume cardiac centers Establish public-private partnerships Regulate and standardize cardiac surgical supply chain Establish or expand public insurance schemes Increase government spending on health Introduce economies of scale Upper middle-income countries Increased surveillance of rheumatic fever, RHD, CHD, and other cardiac diseases Introduce public campaigns and patient counseling to empower lifestyle changes to reduce IHD Expand South-South partnerships Regulate task-sharing for nonsurgical care (eg, nurse anesthetist) Establish or increase national or regional cardiac surgery residency and fellowship programs Train ancillary health staff Strengthen existing cardiac centers to become highvolume centers of excellence Establish public-private partnerships Regulate and standardize cardiac surgical supply chain Establish or expand public insurance schemes Increase government spending on health Introduce economies of scale High-income countries Introduce public campaigns and patient counseling to empower lifestyle changes to reduce IHD Expand North-South partnerships Establish team training programs for cardiac surgery teams from low- and lower middle-income countries Regulate quality of procurement of functional cardiac surgical equipment and consumables Increase developmental aid Introduce economies of scale RHD, Rheumatic heart disease; CHD, congenital heart disease; IHD, ischemic heart disease. population and 11.1 pediatric cardiac surgeons per million pediatric population. Disparities are even clearer when comparing World Bank income groups. Low-income countries possess 0.04 adult cardiac surgeons per million population and 0.07 pediatric cardiac surgeons per million pediatric population, compared with 7.15 adult cardiac surgeons per million population and 9.51 pediatric cardiac surgeons per million pediatric population in high-income countries. Because of the complexity of interventions, cardiac surgeons are concentrated in large urban areas, limiting available services for rural populations. However, it is important to recognize that mere availability of cardiac surgeons does not necessarily translate to access to cardiac surgery. Adequate preoperative (eg, imaging, laboratory services, cardiology, general medical care), intraoperative (eg, blood banking, cardiopulmonary bypass equipment, perfusionists, technicians), and postoperative services (eg, intensive care unit, follow-up cardiology services, anticoagulation) are essential to facilitate true access. Central to the human resources crisis underlying cardiac surgical care, the need arises for high-volume and high-quality training facilities adapted to local needs. Budding centers and visiting surgeons have to be fully 8 capable of handling, among others, the higher prevalence of endomyocardial fibrosis in equatorial African countries, the widespread prevalence of RHD, conditions with more advanced disease processes due to delayed diagnosis or access to care, and the use of materials that are low cost and easily accessible, which are notable challenges in lowand middle-income countries. Accordingly, the establishment of centers of excellence and training centers should include a focus on training of surgeons and supporting staff on the management of the regionally prevalent and growing cardiac disease burden. Increasing cardiac surgical workforce in low- and middle-income countries without parallel increase in financial risk protection (ie, health insurance coverage) will have limited effects on access. The high costs for patients to pay for the procedure (direct costs) and indirect costs related to the visit to the hospital (eg, transportation and food costs) further limit access to care through imposed catastrophic expenditure for patients and their families.32 Traditionally, cardiac surgery has been perceived as a high-cost luxury lacking priority in low- and middle-income countries. Nevertheless, although cost-effectiveness analyses on cardiac surgery are scarce in low- and middle-income The Journal of Thoracic and Cardiovascular Surgery c - 2019 Vervoort et al Miscellaneous Study Limitations Data presented in this article have important limitations. The database of the CTSNet was not fully up-to-date with some errors in country allocation and thus only provides an estimate of the exact number of cardiac surgeons in each country. The CTSNet database combines databases of regional cardiac societies, in addition to voluntary participation by professionals not registered with other societies. Because of less accurate registration of surgeons in low- and middle-income countries (eg, Papua New Guinea) and countries where the English language is not widespread (eg, Japan), these numbers were particularly underestimated. Unregistered surgeons may exist and operate through alternative circuits. For example, CTSNet did not register any cardiac surgeon in the Democratic Republic of Congo and Ethiopia, even though cardiac centers exist in Kinshasa and Addis Ababa, respectively. A follow-up study aims to include a worldwide survey among registered surgeons to assess current and recent work commitment to further specify availability of cardiac surgery. Moreover, surgeons registered as pure thoracic surgeons and general surgeons should be inquired about the number of cardiac interventions they perform in areas lacking pure cardiac surgeons. Last, because of the lack of a database and available literature for the number of interventional cardiologists and surgical and minimally invasive interventions, the establishment of global inclusive databases is warranted. CONCLUSIONS This is a comprehensive study mapping the global state of access to cardiac surgery. Disparities in distribution of cardiac surgical workforce and availability of open surgery exist between and within world regions. The establishment of centralized, high-volume centers providing high-quality training programs adapted to local needs is essential to populate low- and middle-income countries with adequate numbers of skilled native cardiac surgeons and other cardiac surgical workforce in the next decades. International support from international bodies and NGOs is critical to create a sustainable framework supporting clinical research and educational programs contextualized within existing socioeconomic and political systems. There is the need to increase human and physical resources, while focusing on safety, quality, and efficiency to improve access to cardiac surgery for the 4.5 billion people without. Conflict of Interest Statement B.M. is a consultant for Edwards and LivaNova. All other authors have nothing to disclose with regard to commercial support. References 1. World Health Organization. Global Status Report on Noncommunicable Diseases 2010. Geneva; 2011. 2. Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA, et al. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569-624. 3. Vervoort D. Global cardiac surgery: a wake-up call. Eur J Cardiothorac Surg. September 27, 2018 [Epub ahead of print]. 4. Yankah C, Fynn-Thompson F, Antunes M, Edwin F, Yuko-Jowi C, Mendis S, et al. Cardiac surgery capacity in sub-Saharan Africa: Quo vadis? J Thorac Cardiovasc Surg. 2014;62:393-401. 5. Pezzella AT. Global aspects of cardiothoracic surgery with focus on developing countries. Asian Cardiovasc Thorac Ann. 2010;18:299-310. 6. Turina MI. European Association for Cardio-Thoracic Surgery: carrying the torch. Eur J Cardiothorac Surg. 2002;22:857-63. 7. Reichert HA, Rath TE. Cardiac surgery in developing countries. J Extra Corpor Technol. 2017;49:98-106. 8. Wang H, Naghavi M, Allen C, Barber RM, Bhutta ZA, Carter A, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1459-544. 9. Z€uhlke L, Engel ME, Karthikeyan G, Rangarajan S, Mackie P, Cupido B, et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: the global rheumatic heart disease registry (the REMEDY study). Eur Heart J. 2015;36:1115-22. 10. Zilla P, Bolman RM, Yacoub MH, Beyersdorf F, Sliwa K, Z€uhlke L, et al. The Cape Town Declaration on access to cardiac surgery in the developing world. Eur J Cardiothorac Surg. 2018;54:407-10. 11. Sandoval N, Kreutzer C, Jatene M, Sessa T Di, Novick W, Jacobs JP, et al. Pediatric cardiovascular surgery in South America. World J Pediatr Congenit Heart Surg. 2010;1:321-7. 12. Van Der Linde D, Konings EEM, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJM, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58:2241-7. 13. Hewitson J, Zilla P. Children’s heart disease in sub-Saharan Africa: challenging the burden of disease. South Afr Med J. 2010;7:18-29. 14. Bickler SW, Weiser TG, Kassebaum NJ, Higashi H, Chang DC, Barendregt JJ, et al. Global burden of surgical conditions. In: Debas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN, eds. Disease Control Priorities Third Edition: Essential Surgery. Washington, DC: World Bank Group; 2015. 15. Sakran JV, Greer SE, Werlin E, McCunn M. Care of the injured worldwide: trauma still the neglected disease of modern society. Scand J Trauma Resusc Emerg Med. 2012;20:64. 16. IHME GHDx. GBD Results Tool. 2016. Available at: http://ghdx.healthdata.org /gbd-results-tool. Accessed August 20, 2018. 17. Cardarelli M, Vaikunth S, Mills K, Disessa T, Molloy F, Sauter E, et al. Costeffectiveness of humanitarian pediatric cardiac surgery programs in low- and middle-income countries. JAMA Netw Open. 2018;1:1-12. 18. Grimes CE, Henry JA, Maraka J, Mkandawire NC, Cotton M. Cost-effectiveness of surgery in low- and middle-income countries: a systematic review. World J Surg. 2014;38:252-63. 19. Yacoub MH. Establishing pediatric cardiovascular services in the developing world: a wake-up call. Circulation. 2007;116:1876-8. 20. Wan S, Yim APC. Cardiothoracic Surgery in China: Past, Present and Future. Hong Kong: The Chinese University Press; 2007. 21. Yacoub M, ElGuindy A, Afifi A, Yacoub L, Wright G. Taking cardiac surgery to the people. J Cardiovasc Transl Res. 2014;7:797-802. 22. Rose J, Chang DC, Weiser TG, Kassebaum NJ, Bickler SW. The role of surgery in global health: Analysis of United States inpatient procedure frequency by The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 9 MIS countries, available data indicate a financially beneficial comparison of congenital heart surgery compared with other surgical interventions.33,34 These considerations point to the importance of integrating cardiac surgical systems strengthening within wider surgical and health systems strengthening through National Surgical, Obstetric, and Anesthesia Plans, strategic and comprehensive plans embedded within national health plans to scale access to surgical care on a national level. Altogether, scaling cardiac services support and rely on efforts toward universal health coverage. Miscellaneous 23. 24. 25. 26. 27. 28. 29. condition using the global burden of disease 2010 framework. PLoS One. 2014;9: e89693. Kumar RK, Shrivastava S. Paediatric heart care in India. Heart. 2008;94:984-90. Davis PJ, Wainer Z, O’Keefe M, Nand P. Cardiac surgery in the Pacific Islands. ANZ J Surg. 2011;81:871-5. Raj M, Paul M, Sudhakar A, Varghese AA, Haridas AC, Kabali C, et al. Microeconomic impact of congenital heart surgery: results of a prospective study from a limited-resource setting. PLoS One. 2015;10:1-13. Leirner AA. The health and wealth of nations-coping with limited resources. Artif Organs. 2006;30:493-7. Henry JA, Price R. The Transforming power of high-quality surgical care: surgery’s role in improving public health. In: Park A, Price R, eds. Global Surgery: The Essentials. New York: Springer; 2017. Mirabel M, Lachaud M, Offredo L, Lachaud C, Zuschmidt B, Ferreira B, et al. Cardiac surgery in low-income settings: 10 years of experience from two countries. Arch Cardiovasc Dis. 2017;110:82-90. Mocumbi AO, Lameira E, Yaksh A, Paul L, Ferreira MB, Sidi D. Challenges on the management of congenital heart disease in developing countries. Int J Cardiol. 2011;148:285-8. Vervoort et al 30. Ng-Kamstra JS, Riesel JN, Arya S, Weston B, Kreutzer T, Meara JG, et al. Surgical non-governmental organizations: global surgery’s unknown nonprofit sector. World J Surg. 2016;40:1823-41. 31. Velebit V, Montessuit M, Bednarkiewicz M, Khatchatourian G, Mueller X, Neidhart P. The development of cardiac surgery in an emerging country: a completed project. Tex Heart Inst J. 2008;35:301-6. 32. Sadoh WE, Nwaneri DU, Owobu AC. The cost of out-patient management of chronic heart failure in children with congenital heart disease. Niger J Clin Pract. 2011;14:65-9. 33. Chao TE, Sharma K, Mandigo M, Hagander L, Resch SC, Weiser TG, et al. Costeffectiveness of surgery and its policy implications for global health: a systematic review and analysis. Lancet Glob Heal. 2014;2:334-45. 34. Saxton AT, Poenaru D, Ozgediz D, Ameh EA, Farmer D, Smith ER, et al. Economic analysis of children’s surgical care in low- and middle-income countries: a systematic review and analysis. PLoS One. 2016;11:e0165480. Key Words: global health, health policy, education MIS 10 The Journal of Thoracic and Cardiovascular Surgery c - 2019 Miscellaneous APPENDIX E1. SUPPLEMENTAL VALIDATION Supplemental Document: Cardiothoracic Surgery Network Data Validation Validation of data obtained on the number of cardiac surgeons registered with the CTSNet database was done for a sample of countries whose national societies are not participating organizations of CTSNet (and thus not automatically register with CTSNet), using data from Fellow registries, national and regional public databases, national health reports, and academic literature. Sample low-, middle-, and high-income countries were validated. A subset analysis of English-speaking and non–English-speaking countries was performed. Low-Income Countries Ethiopia COSECSA Member/Fellow DirectoryE1: 8 cardiothoracic surgeons CTSNet database: 0 cardiac surgeons, 0 thoracic surgeons (0 total) Mozambique COSECSA Member/Fellow DirectoryE1: 1 cardiothoracic surgeon CTSNet database: 0 cardiac surgeons, 1 thoracic surgeon (1 total) Nepal Hosain and colleaguesE2: 15 cardiac surgeons CTSNet database: 16 cardiac surgeons Tanzania COSECSA Member/Fellow DirectoryE1: 5 cardiothoracic surgeons CTSNet database: 3 cardiac surgeons, 2 of which thoracic surgeons (3 total) Uganda COSECSA Member/Fellow DirectoryE1: 3 cardiothoracic surgeons CTSNet database: 2 cardiac surgeons, 2 thoracic surgeons (2 total) Zimbabwe COSECSA Member/Fellow DirectoryE1: 2 cardiothoracic surgeons CTSNet database: 2 cardiac surgeons, 1 thoracic surgeon (3 total) Middle-Income Countries Bolivia Sandoval and colleaguesE3: 6 pediatric cardiac surgeons CTSNet database: 6 pediatric cardiac surgeons Colombia Sandoval and colleaguesE3: 24 pediatric cardiac surgeons CTSNet database: 23 pediatric cardiac surgeons Ghana Edwin and colleaguesE4: 6 cardiothoracic surgeons CTSNet database: 5 cardiac surgeons, 5 thoracic surgeons (6 total) Kenya COSECSA Member/Fellow DirectoryE1: 5 cardiothoracic surgeons CTSNet database: 5 cardiac surgeons, 5 thoracic surgeons (5 total) Nigeria Ekure and colleaguesE5: 31 cardiac surgeons CTSNet database: 29 cardiac surgeons Pakistan Hosain and colleaguesE2: 140 cardiac surgeons CTSNet database: 84 cardiac surgeons Paraguay Sandoval and colleaguesE3: 5 pediatric cardiac surgeons CTSNet database: 3 pediatric cardiac surgeons Peru Sandoval and colleaguesE3: 8 pediatric cardiac surgeons CTSNet database: 13 pediatric cardiac surgeons Sri Lanka Hosain and colleaguesE2: 24 cardiac surgeons CTSNet database: 19 cardiac surgeons Zambia COSECSA Member/Fellow DirectoryE1: 0 cardiothoracic surgeons CTSNet database: 0 cardiac surgeons, 0 thoracic surgeons (0 total) High-Income Countries Canada Royal College Directory of FellowsE6: 267 active cardiac surgeons CTSNet database: 267 cardiac surgeons Singapore College of Surgeons Singapore Chapter of Cardiothoracic Surgeons Annual Report 2016E7: 36 local cardiac surgeons CTSNet database: 31 cardiac surgeons Subset Analysis A subset analysis of English-speaking versus non–English-speaking countries included above to assess whether the CTSNet database is biased toward higher inclusion of English-speaking cardiac surgeons indicates comparable accuracy of data among countries from different language groups. However, it is reiterated that data from most other countries are not readily available beyond the CTSNet database. The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - 10.e1 MIS Vervoort et al Miscellaneous E-References E1. College of Surgeons of Eastern Central and Southern Africa. COSECSA Members and Fellows Directory. Available at: http://www.cosecsa.org/membersfellows-directory. Accessed January 15, 2019. E2. Hosain N, Amin F, Rehman S, Koirala B. Know thy neighbors: the status of cardiac surgery in the South Asian countries around India. Indian Heart J. 2017; 69:790-6. E3. Sandoval N, Kreutzer C, Jatene M, Sessa T Di, Novick W, Jacobs JP, et al. Pediatric cardiovascular surgery in South America: current status and regional differences. World J Pediatr Congenit Heart Surg. 2010;1:321-7. E4. Edwin F, Tettey M, Aniteye E, Tamatey M, Sereboe L, Entsua-Mensah K, et al. The development of cardiac surgery in West Africa–the case of Ghana. Pan Afr Med J. 2011;9:15. E5. Ekure EN, Sadoh WE, Bode-Thomas F, Orogade AA, Animasahun AB, Ogunkunle OO, et al. Audit of availability and distribution of paediatric cardiology services and facilities in Nigeria. Cardiovasc J Afr. 2017;28:54-9. E6. Royal College of Physicians and Surgeons of Canada. Royal College Directory. Available at: https://rclogin.royalcollege.ca/webcenter/portal/rcdirectory_en. Accessed January 15, 2019. E7. College of Surgeons Singapore. Chapter of Cardiothoracic Surgeons College of Surgeons Singapore Annual Report 2016. Available at: https://ams.edu.sg/ view-pdf.aspx?file¼media%5C4701_fi_488.pdf&ofile¼ChapterþReport þ2016þ-þCTS.pdf. Accessed January 15, 2019. E8. Pezzella AT. Global aspects of cardiothoracic surgery with focus on developing countries. Asian Cardiovasc Thorac Ann. 2010;18:299-310. E9. Doherty C, Holtby H. Pediatric cardiac anesthesia in the developing world. Paediatr Anaesth. 2011;21:609-14. Vervoort et al E10. Yacoub M, ElGuindy A, Afifi A, Yacoub L, Wright G. Taking cardiac surgery to the people. J Cardiovasc Transl Res. 2014;7:797-802. E11. Yankah C, Fynn-Thompson F, Antunes M, Edwin F, Yuko-Jowi C, Mendis S, et al. Cardiac surgery capacity in sub-Saharan Africa: Quo vadis? J Thorac Cardiovasc Surg. 2014;62:393-401. E12. Edwin F, Entsua-Mensah K, Sereboe LA, Tettey MM, Aniteye EA, Tamatey MM, et al. Conotruncal heart defect repair in Sub-Saharan Africa: remarkable outcomes despite poor access to treatment. World J Pediatr Congenit Heart Surg. 2016;7:592-9. E13. Okwuosa IS, Lewsey SC, Adesiyun T, Blumenthal RS, Yancy CW. Worldwide disparities in cardiovascular disease: challenges and solutions. Int J Cardiol. 2016;202:433-40. E14. Kwan GF, Mayosi BM, Mocumbi AO, Miranda JJ, Ezzati M, Jain Y, et al. Endemic cardiovascular diseases of the poorest billion. Circulation. 2016; 133:2561-75. E15. Mirabel M, Lachaud M, Offredo L, Lachaud C, Zuschmidt B, Ferreira B, et al. Cardiac surgery in low-income settings: 10 years of experience from two countries. Arch Cardiovasc Dis. 2017;110:82-90. E16. Reichert HA, Rath TE. Cardiac surgery in developing countries. J Extra Corpor Technol. 2017;49:98-106. E17. Edwin F, Zuhlke L, Farouk H, Mocumbi AO, Entsua-Mensah K, DelsolGyan D, et al. Status and challenges of care in Africa for adults with congenital heart defects. World J Pediatr Congenit Heart Surg. 2017;8: 495-501. E18. Zilla P, Bolman RM, Yacoub MH, Beyersdorf F, Sliwa K, Z€uhlke L, et al. The Cape Town Declaration on access to cardiac surgery in the developing world. Eur J Cardiothorac Surg. 2018;54:407-10. MIS 10.e2 The Journal of Thoracic and Cardiovascular Surgery c - 2019 Author(s) Year Country/region Data source Surgical infrastructure Surgical workforce Surgical capacity >6000 cardiac centers >2 million open surgeries per year Surgical quality Additional findings Pezzella 2010 Global Literature review >10,000 cardiothoracic surgeons Sandoval and colleaguesE3 2010 South America Primary survey data Literature review >195 cardiac surgeons 138 cardiac centers 41% (24,081) of CHD Not specified cases per year left untreated Edwin and colleaguesE4 2011 National CardioPrimary institutional thoracic Center, Korle data Bu, Accra, Ghana Literature review 6 cardiothoracic surgeons 2 operating rooms 1 catheterization lab 464 cardiac surgeries 5.3% in-hospital Open surgery spans (2008) mortality for pediatric decades in West mechanical valve Africa replacement Cardiac surgery relies on stable political climate, economic growth, leadership, and prudent fiscal management Doherty and colleaguesE9 2011 Global Literature review NA NA NA Yacoub and colleaguesE10 2014 Aswan Heart Center, Egypt Primary institutional data Literature review Not specified 752 cardiac surgeries 5% in-hospital 2 cardiac operating (2013) mortality rooms 2 catheterization labs Advanced imaging suite Yankah and colleaguesE11 2014 Africa (excluding South Primary survey data Africa) CTSNet South Africa E8 NA NA Descriptive capacity summary CHD prevalence 58,718 cases per year No training and qualifications consensus for pediatric cardiac anesthesia; often nonexistent in lowand middle-income countries Need for local staff trained in pediatric cardiac anesthesia for safer surgery for more children Descriptive comparison and sustainable model of cardiac programs 75% of world does not have access to cardiac surgery 10.e3 China: 158 open surgeries per million population Germany: 1038 open (Continued) MIS Miscellaneous The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - Africa (excluding Africa (excluding Africa (excluding South Africa): 156 South Africa): 78 South Africa): cardiac surgeons cardiac centers (22 10,725 open (57 in sub-Saharan in sub-Saharan operations (2012): NA Vervoort et al TABLE E1. Global cardiac surgery capacity studies MIS TABLE E1. Continued Year Country/region Data source Surgical infrastructure Surgical workforce Surgical capacity The Journal of Thoracic and Cardiovascular Surgery c - 2019 Africa; 56 in North Africa; 99 in North Africa) Africa) South Africa: 35 South Africa: 50 cardiac centers cardiac surgeons 1277 in subSaharan Africa; 9448 in North Africa South Africa: 8280 open surgeries Surgical quality Additional findings surgeries per million population In Africa, only 51.4% of cardiac surgeons registered with CTSNet performed open surgery in 2012 Primary institutional 2016 National Cardiothoracic Center, Korle data Bu, Accra, Ghana Not specified 1 cardiac center Nigeria, Democratic Access to surgery for Modified Blalock– Republic of the conotruncal Taussig shunt: 0% Congo, Ethiopia, anomalies within 30-d mortality Tanzania, Uganda, 2 y of birth <1% Intracardiac repair: 4% and Kenya account 30-d mortality for 53.5% of CHD cases in sub-Saharan Africa Okwuosa and colleaguesE13 2016 Global Literature review NA NA NA NA Descriptive summary of social determinants of health and global disparities to cardiac care Kwan and colleaguesE14 2016 Global NA Primary data Global Burden of Disease study 2013 NA NA NA Ischemic heart disease 12% of total CVD burden in poorest countries; 51% in high-income countries 53% of CVD burden attributed to behavioral or metabolic risk factors in poorest countries; 85% in high-income countries 34% of CVD burden in people aged <30 y in poorest countries; 3% in people aged <30 y in high-income countries (Continued) Vervoort et al Edwin and colleaguesE12 Miscellaneous 10.e4 Author(s) Author(s) Year Country/region Data source Surgical infrastructure Surgical workforce Surgical capacity Surgical quality Additional findings 2017 MozambiqueCambodia Primary institutional data NA NA NA 55.63% of patients in Mozambique: 6.10% Cambodia and 14.6% early (30-d) in Mozambique lost postoperative to follow-up at 30 d mortality rate Cambodia: 3.05% early due to remoteness postoperative mortality rate Ekure and colleaguesE5 2017 Nigeria Primary institutional and survey data 31 cardiac surgeons 6 cardiac centers NA NA Hosain and colleaguesE2 2017 Bangladesh India Nepal Pakistan Sri Lanka Primary institutional and survey data Bangladesh: 80 cardiac surgeons India: 700 cardiac surgeons Nepal: 15 cardiac surgeons Pakistan: 140 cardiac surgeons Sri Lanka: 24 cardiac surgeons Bangladesh: 25 cardiac centers India: number not specified Nepal: number not specified Pakistan: over 40 cardiac centers Sri Lanka: 11 cardiac centers Bangladesh: 11,121 NA cardiac surgeries (2012) India: 150,000 cardiac surgeries per year Nepal: 2000 cardiac surgeries (2016) Pakistan: >20,000 cardiac surgeries per year Sri Lanka: 5500 cardiac surgeries (2016) Bangladesh, Nepal, Pakistan, Sri Lanka important sources of medical tourism in India; USD3 billion annually Reichert and colleaguesE16 2017 Global Literature review NA NA NA North America, Australia, Europe: 860 cardiac surgeries per million people South America, the Russian Federation, Asia, Africa: 60 cardiac surgeries per million people 4.5 billion people in low- and middleincome countries no access to cardiac surgery Edwin and colleaguesE17 2017 Africa Previous estimates (7) NA Literature review South Africa: 35 cardiac centers Egypt: 48 cardiac centers Shisong, Cameroon: NA 35-50 congenital heart surgeries per year Africa cumulative CHD prevalence 300,486 cases Cost of open surgery between US$6230 and US$11,200 10.e5 (Continued) MIS Miscellaneous The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number - Mirabel and colleaguesE15 Vervoort et al TABLE E1. Continued MIS The Journal of Thoracic and Cardiovascular Surgery c - 2019 Author(s) Year Country/region Data source Surgical workforce Surgical infrastructure Surgical capacity South Africa: 8280 open surgeries per year Egypt: >16,000 procedures per year Zilla and colleaguesE18 2018 16 countries Primary survey National databases Annual reports data 0.06 (Nigeria) to 11.5 0.08 (Nigeria) to 1.6 0.5 cardiac surgeries NA per million in (Brazil) public (Germany) cardiac assessed lowcardiac centers per surgeons per income countries million population million population and lower-middlein assessed in assessed income countries to countries countries 500 per million in upper-middleincome countries Surgical quality Additional findings 51.4% of total birth prevalence in 7 countries Increase in adult CHD pool not met by care capacity Miscellaneous 10.e6 TABLE E1. Continued Need estimates: 200 operations per million in low-income countries to >1000 per million in highincome countries NA, Not available; CHD, congenital heart disease; CTSNet, Cardiothoracic Surgery Network; CVD, cardiovascular disease. Vervoort et al Vervoort et al Global cardiac surgery: Access to cardiac surgical care around the world Dominique Vervoort, MD, Bart Meuris, MD, PhD, Bart Meyns, MD, PhD, and Peter Verbrugghe, MD, PhD, Boston, Mass, and Leuven, Belgium Some 4.5 billion people lack access to cardiac surgery when needed. Availability of adult and pediatric cardiac surgical workforce is scarce in low- and middle-income countries, and disparities are widespread. MIS 000 Miscellaneous The Journal of Thoracic and Cardiovascular Surgery c Volume -, Number -