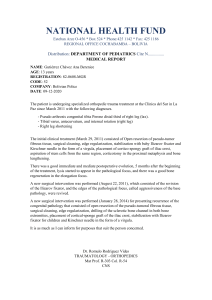
Review Article The Hill-Sachs Lesion: Diagnosis, Classification, and Management Abstract CDR Matthew T. Provencher, MD Rachel M. Frank, MD LCDR Lance E. LeClere, MD LCDR Paul D. Metzger, MD J. J. Ryu LT Andrew Bernhardson, MD Anthony A. Romeo, MD The Hill-Sachs lesion is an osseous defect of the humeral head that is typically associated with anterior shoulder instability. The incidence of these lesions in the setting of glenohumeral instability is relatively high and approaches 100% in persons with recurrent anterior shoulder instability. Reverse Hill-Sachs lesion has been described in patients with posterior shoulder instability. Glenoid bone loss is typically associated with the Hill-Sachs lesion in patients with recurrent anterior shoulder instability. The lesion is a bipolar injury, and identification of concomitant glenoid bone loss is essential to optimize clinical outcome. Other pathology (eg, Bankart tear, labral or capsular injuries) must be identified, as well. Treatment is dictated by subjective and objective findings of shoulder instability and radiographic findings. Nonsurgical management, including focused rehabilitation, is acceptable in cases of small bony defects and nonengaging lesions in which the glenohumeral joint remains stable during desired activities. Surgical options include arthroscopic and open techniques. T From the Department of Orthopaedic Surgery, Naval Medical Center San Diego, San Diego, CA (Dr. Provencher, Dr. LeClere, Dr. Metzger, and Dr. Bernhardson), the Naval Medical Center San Diego (Ms. Ryu), and the Department of Orthopedic Surgery, Rush University Medical Center, Chicago, IL (Dr. Frank and Dr. Romeo). The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. J Am Acad Orthop Surg 2012;20: 242-252 http://dx.doi.org/10.5435/ JAAOS-20-04-242 Copyright 2012 by the American Academy of Orthopaedic Surgeons. 242 he Hill-Sachs lesion is a compression fracture of the posterosuperolateral humeral head that occurs in association with anterior instability or dislocation of the glenohumeral joint. In 1940, Hill and Sachs1 described the lesion as a socalled line of condensation on the internal rotation shoulder radiograph. They attributed this line to the impression of the dense cortical glenoid on the humeral head during an anterior dislocation event. Improved understanding of the association between humeral head bony defects and recurrent glenohumeral instability has resulted in increased interest in identifying the optimal manner by which to classify and manage Hill-Sachs injuries. There is an historical body of evidence supporting an association between a combined engaging Hill-Sachs lesion and anterior glenoid bone loss in cases of recurrent instability.2-5 Although a substantial amount of literature exists on the well-established relationship between glenoid bony defects and shoulder instability,6-8 there is a relative paucity of literature on humeral head defects.9 Epidemiology The true incidence of Hill-Sachs lesions is unknown. However, they are associated with approximately 40% to 90% of all anterior shoulder instability events.10-14 The incidence may be as high as 100% in patients with recurrent anterior instability.13 Determining which Hill-Sachs lesions are associated with clinical symptoms and which are incidental remains challenging. This is espe- Journal of the American Academy of Orthopaedic Surgeons CDR Matthew T. Provencher, MD, et al cially important in patients with recurrent instability because humeral head bony deficits may contribute to continued instability. Reverse Hill-Sachs lesions are associated with posterior shoulder dislocation. The incidence of this type is equally difficult to quantify, although reverse lesions occur in up to 86% of posterior shoulder dislocations.12 However, posterior shoulder instability events are relatively uncommon, and reverse Hill-Sachs lesions are rare. Pathophysiology Hill-Sachs lesions most commonly occur during an anterior glenohumeral instability injury, typically with the shoulder in abduction and external rotation. As the humeral head is forced anteriorly, the capsulolabral structures of the shoulder are stretched and often torn. As the humeral head translates farther anteriorly, a compression fracture occurs along the posterosuperolateral aspect of the humeral head as it comes into contact with the anterior glenoid (Figure 1). The damaged anterior soft-tissue structures are particularly problematic in cases of recurrent instability because the static glenohumeral constraints (ie, capsule, labrum) become increasingly attenuated with each episode. This attenuation makes it easier for the relatively softer cancellous bone of the humeral head to sustain continued damage as it makes repeated contact with the harder cortical bone of the anterior glenoid.9 The traditional Hill-Sachs lesion is a bony defect of the posterosuperolateral humeral head, typically associated with anteroinferior glenohumeral dislocation. An engaging Hill-Sachs lesion, as described by Palmer and Widén15 and Burkhart and De Beer,2 occurs when the humeral head defect engages the rim of the glenoid while the shoulder is in a position of athletic function (ie, 90° abduction and 0 degrees to 135° of external rotation) (Figure 2, A and B). In an engaging lesion, the long axis of the humeral head defect is oriented parallel to the anterior glenoid rim and thus engages with it when the shoulder is in abduction and external rotation.9 When the humeral defect is not in parallel with the rim of the glenoid and thus does not engage with it in a position of function, the lesion is referred to as nonengaging2 (Figure 2, C and D). The reverse Hill-Sachs lesion is a bony defect of the anterosuperomedial humeral head. This type most commonly is caused by posterior shoulder dislocation. The main differences between traditional and reverse Hill-Sachs lesions are listed in Table 1. Hill-Sachs lesions rarely occur in isolation. The injury most commonly sustained in conjunction with the Hill-Sachs lesion is the anterior capsulolabral lesion (ie, Bankart).11 Figure 1 Three-dimensional CT scan demonstrating the typical location of a Hill-Sachs lesion at the superolateral aspect of the posterior humeral head (arrows). The harder anteroinferior glenoid bone compresses the soft cancellous bone in this region as the humeral head dislocates, creating the characteristic osseous lesion. Other common coexisting injuries are anterior glenohumeral ligamentous pathology and glenoid bone loss (ie, bony Bankart lesion)5,16 (Figure 3). Anteroinferior glenoid bone loss may ultimately become large enough to create a glenoid with the appearance of an inverted pear; this presentation is associated with recurrent anterior shoulder instability.8,17 Optimal management requires close evaluation for glenoid bone loss because bone loss in the shoulder is frequently a bipolar phenomenon.7 It is also important to recognize normal anatomic structures of the posterior humeral head to avoid con- Dr. Provencher or an immediate family member serves as a board member, owner, officer, or committee member of the American Academy of Orthopaedic Surgeons; the American Orthopaedic Society for Sports Medicine; the Arthroscopy Association of North America; the International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine; and the Society of Military Orthopaedic Surgeons. Dr. Romeo or an immediate family member has received royalties from Arthrex; is a member of a speakers’ bureau or has made paid presentations on behalf of Arthrex, DJ Orthopaedics, and the Joint Restoration Foundation; serves as a paid consultant to or is an employee of Arthrex; has received research or institutional support from Arthrex and DJ Orthopaedics; has received nonincome support (such as equipment or services), commercially derived honoraria, or other non–research-related funding (such as paid travel) from Arthrex and DJ Orthopaedics; and serves as a board member, owner, officer, or committee member of the American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, and the Arthroscopy Association of North America. None of the following authors or any immediate family member has received anything of value from or owns stock in a commercial company or institution related directly or indirectly to the subject of this article: Dr. Frank, Dr. LeClere, Dr. Metzger, Ms. Ryu, and Dr. Bernhardson. April 2012, Vol 20, No 4 243 The Hill-Sachs Lesion: Diagnosis, Classification, and Management become the shaft. On the axial view, this groove is located more inferior and posterior (between 140° and 230°) than are Hill-Sachs lesions, which typically fall more laterally (between 170° and 260°). Figure 2 Clinical Evaluation History and Physical Examination A, Illustration of an engaging Hill-Sachs lesion (dark gray area). B, With the shoulder in a position of function or in abduction and external rotation, the lesion is oriented parallel with the anterior glenoid and thus engages it. C, Illustration of a nonengaging lesion (dark gray area), which is created in a nonfunctional position. D, When the shoulder is abducted and externally rotated, the lesion is not oriented parallel to the glenoid and thus does not engage. (Redrawn with permission from Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16[7]:677-694.) Table 1 Key Differences Between Traditional and Reverse Hill-Sachs Lesions Traditional Located on the posterosuperolateral humeral head Anterior or anteroinferior dislocation Posterior cartilage damage (usually less than in reverse lesions) fusing them with Hill-Sachs lesions. The bare spot of the humeral head, which has no direct attachment of the rotator cuff tendons, is located superior and slightly medial to the 244 Reverse A thorough history and physical examination are important in the clinical evaluation of the patient with a Hill-Sachs lesion associated with glenohumeral instability (Table 2). Special attention should be paid to the mechanism of injury, which likely involves an initial traumatic dislocation event with the arm in abduction and external rotation.16 In the presence of an intact glenoid, the HillSachs lesion may be clinically silent. The patient with glenoid bone loss and/or an engaging lesion may describe a sensation of catching as the humeral head falls outside the glenoid track during movement (Figure 4). (The glenoid track is described in detail below.) In such cases, instability may result from trivial events such as sleeping with the arm overhead.21 During the physical examination, the appearance, range of motion, strength, and sensation of the injured shoulder should be compared with those of the contralateral shoulder. Imaging Located on the anterosuperomedial humeral head Posterior shoulder dislocation (rare) Anterior cartilage damage that is much more extensive than the posterior cartilage damage seen in traditional lesions typical location of a Hill-Sachs lesion. As described by Richards et al,18 the anatomic groove of the humeral head is the normal flattening of the head as it moves caudad to Several imaging modalities can be used to assess humeral head osseous deficiency. A full shoulder radiographic series is typically obtained, including AP, lateral, and axillary views. Several other views can be more helpful in evaluating humeral head bone loss specifically. The modified West Point axillary view is used in the evaluation of glenoid bone loss, and the Stryker notch view is specific for evaluating the Hill-Sachs Journal of the American Academy of Orthopaedic Surgeons CDR Matthew T. Provencher, MD, et al lesion.22 The Stryker notch view is useful because the internal rotation of the humeral head brings the posterolateral defect into direct view. CT, particularly three-dimensional CT, is a superior imaging option for evaluating bone loss. Three-dimensional CT allows full appreciation of the orientation of the defect, which is extremely useful in decision making and preoperative planning.23 Glenoid bone loss also can be precisely quantified following digital subtraction of the humeral head24 (Figure 1). Ultrasonography may be useful in detecting Hill-Sachs lesions. Cicak et al25 compared intraoperative findings with ultrasonography and found ultrasonography to be 100% specific and 96% sensitive for the detection of Hill-Sachs lesions, with an overall accuracy rate of 97%. MRI or magnetic resonance arthrography may provide information on the glenoid and/or humeral head defects (Figure 5). Without advanced imaging studies, it is difficult to accurately quantify the size and location of the Hill-Sachs lesion and to adequately assess any accompanying glenoid bone loss. Classification Several classification and grading systems for Hill-Sachs lesions have been described; controversy persists regarding which is optimal3,4,10,18,26 (Table 3). Although the classifications and grading systems can be useful in clinical decision making, especially with larger lesions, they have not yet proved to be helpful in determining successful management strategies. Figure 3 A, Arthroscopic view from the anterosuperior portal demonstrating significant bipolar bony defects, with a large Hill-Sachs lesion and concomitant anteroinferior glenoid bone loss measuring approximately 28% of the width of the glenoid. B, Arthroscopic view from the anterosuperior portal of the shoulder after it was brought into the position of function. On abduction and external rotation, the humeral defect clearly engages the anterior glenoid. Engagement was noted at only 45° of abduction and a few degrees of external rotation. Table 2 Important History and Physical Examination Findings for Hill-Sachs Lesions History Deep shoulder pain Previous shoulder instability event Recurrent instability with provocative positioning Mechanical symptoms (eg, crepitus, clicking, catching) History of shoulder reduction, especially manual reduction Progressive ease of dislocation events: Instability with daily events, likely concomitant glenoid defect, likely more significant bony defects Recurrent instability events: Often unprovoked, occurring with increasing frequency, occurring after stabilization procedure(s) Physical examination Assess for instability (ie, apprehension tests) Assess for laxity (ie, translation tests) Assess for concomitant injuries (eg, rotator cuff tear, biceps tendon pathology, superior labrum anterior-posterior lesion) Key findings Apprehension at lesser degrees of abduction (mid range19,20) Palpable clunk with engagement: Typically done under anesthesia. May become locked. In advanced cases, crepitus during range of motion, extension of the lesion to the central humerus, extensive anterior glenoid bone loss, and glenohumeral osteoarthritis Clinical Significance of the Lesion Determining the clinical significance of a Hill-Sachs lesion can be chalApril 2012, Vol 20, No 4 lenging. The most important consideration is establishing whether the lesion is responsible for the patient’s symptoms, especially with regard to the instability event. The most common factors used to 245 The Hill-Sachs Lesion: Diagnosis, Classification, and Management Figure 4 A, Illustration of the glenoid track, which is used in describing Hill-Sachs lesions based on the location and size of the humeral head defect and on the amount of glenoid bone loss. The gray area indicates the zone of contact between the glenoid and the humeral head. The dotted line indicates the contact area between the glenoid and the humeral head. B, The lesion lies within the track, and the lesion cannot override the glenoid rim. C, The lesion lies more medial than the track, thereby making it possible for the humeral head to override the glenoid rim. (Redrawn with permission from Yamamoto N, Itoi E, Abe H, et al: Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: A new concept of glenoid track. J Shoulder Elbow Surg 2007;16[5]:649-656.) determine the significance of a lesion are its size and whether it is engaging.2 Historically, lesions involving <20% of the humeral head articular surface are rarely of clinical significance, whereas lesions >40% of that surface are nearly always clinically significant and are responsible for recurrent instability.3,9 Treatment decision-making is most difficult in the setting of midsize lesions comprising 20% to 40% of the humeral head articular surface. Other factors to consider include the location and orientation of the lesion, the extent of concomitant glenoid bone loss, and the extent of engagement with the glenoid. The location and orientation of the lesion are important 246 factors for defects of any size. In midsize Hill-Sachs lesions, the injury must be recognized as a bipolar problem, with glenoid bone loss potentiating the humeral-side lesion and increasing the risk of instability. Yamamoto et al27 developed a novel approach to describing Hill-Sachs lesions. They based their description on the location and size of the humeral head defect and on the amount of glenoid bone loss. Using a cadaver model, they measured the contact area between the glenoid and humeral head at various degrees of abduction. With the shoulder in 60° of abduction and maximum external rotation to simulate anterior apprehension, the authors found that the distance from the contact area to the medial margin of the footprint was 84% of the glenoid width. The authors proposed that a Hill-Sachs lesion outside this so-called glenoid track was at high risk for engagement and, therefore, recurrent instability. Their classification also takes into account the amount of glenoid bone loss.27 As an osseous glenoid lesion increases in size, the glenoid track decreases accordingly, thereby placing the construct at risk of engagement. Large amounts of glenoid bone loss increase the clinical relevance of even small Hill-Sachs injuries (Figure 4). This biomechanical association was studied clinically by Provencher et al,28 with the goal of determining the clinical significance of Hill-Sachs lesions in the setting of glenoid bone loss. The authors found that 22 of 140 patients (15.7%) had Hill-Sachs lesions outside the glenoid track, as determined by measuring the size of the humeral head lesion and glenoid bone loss on magnetic resonance arthrography. These patients were felt to be at increased risk of glenohumeral engagement. The concept of the glenoid track may be the most clinically relevant system for classifying Hill-Sachs lesions, but additional work is necessary to validate its routine clinical use. Nonsurgical Management Nonsurgical management is warranted in cases of small osseous defects and nonengaging lesions. Even when surgery is warranted, these Hill-Sachs lesions are often left alone intraoperatively, and other clinically relevant pathology (eg, Bankart lesion) is addressed instead. Patients with larger, more clinically significant lesions who may be poor surgical candidates (eg, elderly persons, Journal of the American Academy of Orthopaedic Surgeons CDR Matthew T. Provencher, MD, et al persons at high medical risk) may be best treated nonsurgically. A focused rehabilitation program is essential to nonsurgical management, under the guidance of an experienced physical therapist or athletic trainer. The program must focus on strengthening the deltoid, the rotator cuff muscles, and in particular, the scapular stabilizers. Months of rehabilitation may be required. Surgical Management The indications for surgical management of Hill-Sachs lesions depend on the clinical significance of the defect and on symptoms of instability (Table 4). A variety of arthroscopic and open options is available.9,16,21 Most clinically significant Hill-Sachs injuries may be successfully managed by addressing the primary instability problem, that is, labral tear and/or glenoid bone loss. Thus, glenoid-side techniques are usually adequate. However, several surgical techniques manage the Hill-Sachs lesion directly. Surgical management of osseous lesions related to anterior instability must take into account the bipolar nature of the injury. Several surgical options exist for the patient with an engaging Hill-Sachs injury. Most involve glenoid bone augmentation alone. Anterior glenoid bone loss may be augmented with the Latarjet procedure or iliac crest bone graft to increase the size of the glenoid track and prevent engagement.2,29 Procedures of historical interest include rotational humeral osteotomy and a technique involving tightening the anterior soft-tissue structures to limit external rotation and shift the glenoid track medially and superiorly.11,30 Rotational humeral osteotomy has been used for large HillSachs defects. By externally rotating the proximal humerus surgically, humeral head retroversion is reduced, and the defect ceases to fall into the anterior glenoid on internal rotation. This procedure has fallen out of fa- vor because of concerns regarding nonunion, delayed union, overrotation, risk of fracture, and posttraumatic arthritis. Many procedures directly address the defect, including humeral head autograft or allograft, tissue filling (ie, remplissage; see below), disimpaction, and prosthesis replacement. Regardless of the method chosen, the goal is to prevent further engagement of the HillSachs lesion with the glenoid. Capsular Shift Glenohumeral capsular shift is performed to surgically tighten the cap- Figure 5 Axial (A) and coronal (B) magnetic resonance arthrograms demonstrating a classic Hill-Sachs lesion (arrows). Table 3 Classifications of Hill-Sachs Lesions Grading System Imaging Rowe et al4 Axillary radiograph Calandra et al10 Direct visualization Franceschi et al26 Flatow and Warner3 Direct visualization Direct visualization Hall et al22 Richards et al18 Notch view radiograph Axillary MRI April 2012, Vol 20, No 4 Description Mild, 2 cm long × ≤0.3 cm deep; moderate, 2–4 cm long × 0.3–1 cm deep; severe, 4 cm long × ≥1 cm deep Grade I, confined to articular cartilage; grade II, extension into subchondral bone; grade III, large subchondral defect Grade I, cartilaginous; grade II, bony scuffing; grade III, hatchet fracture Clinically insignificant, <20%; variable significance, 20% to 40%; clinically significant, >40% Percent involvement in 180° articular arc Axillary degrees involved (anterior articular margin, zero degrees) 247 The Hill-Sachs Lesion: Diagnosis, Classification, and Management Figure 6 Table 4 Indications for Surgical Management of Hill-Sachs Lesions Absolute Displaced humeral head fracture with humeral head fracture-dislocation and associated Hill-Sachs injury Lesion >30% to 40% of the humeral head with chronic dislocation or recurrent anterior instability. These cases typically require glenoid augmentation and/or management of the humeral head (eg, remplissage, allograft). Reverse lesion with >20% to 40% of humeral head articular surface involvement and symptoms of posterior instability, catching, or pain Relative Lesion >20% to 35% of the humeral head with glenoid engagement on examination Lesion >20% of the articular surface and signs of humeral head engagement on examination Lesion >10% to 25% of the humeral head that does not remain well-centered in the glenoid fossa after arthroscopic instability repair Reverse lesion with humeral head cartilage involvement on 10% to 30% of the humeral head, with symptoms of posterior instability, catching, or pain sule in an attempt to limit external rotation and anterior translation. This procedure can be performed arthroscopically or via an open approach.31 Although this technique can be effective in enhancing shoulder stability, it is not necessarily an anatomic solution. Additionally, the loss of external rotation may be problematic for young patients, especially overhead-throwing athletes. Even though capsular plication techniques are among the most commonly performed procedures for anterior shoulder stabilization, they address only the soft tissue and may not be adequate in cases of instability with significant Hill-Sachs lesions. Glenoid Bone Augmentation Glenoid bone augmentation has been well-documented as the primary procedure in addressing significant HillSachs defects associated with recurrent glenohumeral instability. The most common procedures used include coracoid transfer (ie, Latarjet) and iliac crest bone grafting.6,16,32,33 Recently, augmentation with various allograft tissues, including femoral 248 head34 and distal tibia allograft,35 has been described (Figure 6). These procedures effectively lengthen the articular arc of the glenoid. Although they do not address the humeral head defect directly, they prevent engagement of the Hill-Sachs lesion during normal range of motion. Humeral Head Bone Augmentation Procedures that directly address HillSachs lesions are traditionally indicated in the setting of significant Hill-Sachs injuries without concomitant glenoid bone loss. In the rare instance of a large Hill-Sachs lesion without concomitant glenoid bone loss, restoration of the anatomy has been advocated, in addition to a variety of soft-tissue procedures. Bone augmentation of the humeral defect has been described to manage large defects with or without glenoid bone injury. The intent with these procedures is to fill the defect and restore native anatomy by effectively increasing the articular arc of the humerus as it rotates on the glenoid, thereby preventing engagement and instability. Bone plugs are typically size-matched to Intraoperative photograph demonstrating the use of iliac crest autograft harvested from the contralateral hip (white arrows) to reconstruct a 25% anterior glenoid bone deficiency. The capsule was sutured to washers under the screw heads (black arrows) on the anterior aspect of the iliac crest, thus making an intra-articular graft of the iliac crest material. This patient also had a 30% Hill-Sachs lesion that easily engaged prior to the iliac crest bone graft. Once grafted, the lesion was unable to engage the glenoid. the defect. These plugs may be autograft (typically from the iliac crest), fresh or frozen allograft, or synthetic (ie, metal, polyethylene) material. Fresh humeral head osteoarticular allografts have been used with success, either with entire humeral head replacement or with grafts size-matched to the defect (Figure 7). Clinical studies describing outcomes following humeral head bone augmentation procedures are limited to small cohorts and case reports. Diklic et al36 reported on the outcomes of 13 patients treated with fresh-frozen femoral head allograft for humeral head defects measuring approximately 25% to 50% (mean age, 42 years). At an average of 54 months postoperatively, 12 patients had stable shoulders, and 1 patient had evidence of osteonecrosis. The mean Constant score for the cohort was 86.8. In a slightly larger cohort Journal of the American Academy of Orthopaedic Surgeons CDR Matthew T. Provencher, MD, et al Figure 7 Intraoperative photographs illustrating the use of fresh proximal humerus allograft to replace a large symptomatic HillSachs lesion. The humeral head is exposed through a deltopectoral approach (A), and the large Hill-Sachs lesion is visualized (B) (arrows). C, The donor humeral head allograft is marked in preparation for harvest of a size-matched graft with an oscillating saw (arrows). D, The size-matched allograft. E, The graft is secured to the native humeral head with buried screws. study, Miniaci and Gish37 described 18 patients with recurrent traumatic instability and Hill-Sachs defects >25% who underwent augmentation with size-matched, fresh-frozen humeral head allografts. At an average follow-up of 50 months postoperatively, 16 patients were able to return April 2012, Vol 20, No 4 to work. However, several complications were noted, including partial radiographic graft collapse (two patients), early radiographic osteoarthritis (three patients), mild subluxation (one patient), and hardware complications (two patients). The mean Constant score was 78.5. Tissue Filling (Remplissage) The Connolly procedure has been successfully used to fill humeral head defects by converting them into extra-articular lesions.38 Originally described in 1972, this open procedure involves transfer of the infraspi- 249 The Hill-Sachs Lesion: Diagnosis, Classification, and Management natus tendon with a portion of the greater tuberosity into the humeral head defect. Recently, surgeons have begun to manage Hill-Sachs lesions arthroscopically using available glenohumeral capsulotendinous tissue. The term remplissage, French for filling, is a surgical technique in which a bony intra-articular defect is converted to an extra-articular defect with soft-tissue coverage, with the goal of preventing engagement.29,39-42 Originally described by Wolf et al,42 the technique involves arthroscopic posterior capsulodesis and infraspinatus tenodesis, with fixation of the tissue to the surface of the Hill-Sachs defect. In 2009, the technique was modified by Koo et al,41 who described a double-pulley suture technique in which two anchors were used to insert the infraspinatus tendon into the entire Hill-Sachs defect. This modification created a broader footprint of fixation, and tying the sutures over rather than through the infraspinatus tendon allowed for a more anatomic and tissue-preserving approach. Remplissage is performed in patients with moderate to large HillSachs defects associated with glenoid defects of <20% to 25%. Patients with larger glenoid defects may require conversion to an open Latarjet procedure. Potential disadvantages associated with remplissage are decreased postoperative range of motion and sequelae of a nonanatomic repair construct. In 2008, Deutsch and Kroll40 described a case of significant postoperative loss of external rotation following remplissage. Motion was improved following arthroscopic release of the infraspinatus tenodesis; the authors proposed that the infraspinatus tendon and posterior capsular tissue created a mechanical block to motion. In their series, Purchase et al29 noted unpublished findings indicating good re- 250 sults with remplissage, with no notable loss of external rotation. Most patients did not experience recurrent instability. Advantages of remplissage include the arthroscopic approach, the ability to perform concomitant procedures, and fast recovery time. Additionally, this approach has none of the risks and morbidity associated with bone grafting procedures. Disimpaction Disimpaction of a humeral head defect (ie, humeroplasty) involves elevating the impaction fracture and supporting it with bone graft, thereby allowing for approximate restoration of humeral head geometry without internal fixation.43,44 The procedure can be performed using bone tamps inserted retrograde through a distal cortical window.43 Alternatively, disimpaction can be performed percutaneously using an 8-mm cannulated reamer drilled to within 1 cm of the posterior surface, followed by backfilling of the defect with cancellous bone chips.44 This technique is relatively new, and little biomechanical and clinical research has been published on the topic. Disimpaction may be most suited to acute lesions <3 weeks old and with <40% involvement of the articular surface.19 Resurfacing and Prosthesis Replacement Complete and partial resurfacing of the humeral head articular surface has been described. Limited resurfacing of the defect with a metal implant is done in an attempt to restore the humeral head articular arc.20,45 Although partial resurfacing is promising in theory, only limited case reports with short-term follow-up are available in the literature. Outcomes have been reported to be positive at 1 to 2 years postimplantation.20,45 With this technique there is no risk of disease transmission or resorption, as can occur with allograft. However, disadvantages include loss of fixation, incomplete geometric restoration, and eventual glenoid wear. Complete humeral head resurfacing (ie, humeral head hemiarthroplasty) is an option for Hill-Sachs lesions that cause recurrent instability, in particular lesions that involve >40% of the articular surface.46 However, indications are not clearly defined. Older (>65 years), low-demand patients may benefit from hemiarthroplasty or total shoulder arthroplasty (TSA) in the presence of concomitant glenoid degeneration. However, outcomes of hemiarthroplasty and TSA are much less predictable, with high failure rates in young, active patients. In these patients, hemiarthroplasty should be considered a salvage procedure in cases of severe defects causing recurrent instability. Pritchett and Clark46 described humeral hemiarthroplasty and TSA in seven patients with chronic dislocations and significant Hill-Sachs lesions. Average patient age was 55 years (range, 36 to 67 years). Five patients had good results, and there were no occurrences of repeat dislocation. These procedures should be reserved for older or less active patients with defects involving >40% of the articular surface and/or significant articular cartilage degeneration. Surgical Management of Reverse Hill-Sachs Lesions Management of reverse Hill-Sachs lesions is based on the same philosophy as management of traditional Hill-Sachs lesions. The primary cause of the instability is addressed with a procedure that prevents engagement of the lesion through direct or indirect means. One fundamental difference between a traditional and a reverse Hill-Sachs lesion is that, in Journal of the American Academy of Orthopaedic Surgeons CDR Matthew T. Provencher, MD, et al reverse injury, the anterior humeral head cartilage is more extensively injured and involved. As such, softtissue filling of the defect has been advocated. However, concerns persist regarding loss of articulation of the humeral head resulting from the generally large and extensive cartilage injury. The well-described McLaughlin procedure involves an open transfer of the subscapularis tendon and lesser tuberosity to fill the humeral head defect.47 The tuberosity transfer involves creation of an osteotomy of the lesser tuberosity while maintaining attachment of the subscapularis tendon and anterior capsule, followed by elevation and transfer to the site of the defect bed. This procedure can result in restriction of internal rotation postoperatively. Krackhardt et al48 described an arthroscopic modification of the McLaughlin procedure and reported successful outcomes and no major complications in 12 patients. Fresh osteoarticular allograft is a viable option for reverse Hill-Sachs lesions because of the increased extent of cartilage involvement compared with a traditional Hill-Sachs injury. Prosthetic reconstruction may also be considered for patients with extremely large reverse Hill-Sachs lesions (ie, >40%). Summary Osseous lesions of the humeral head create challenging clinical scenarios. The most difficult aspect of these cases involves determining which Hill-Sachs lesions are clinically significant and need to be addressed surgically. Lesion size, orientation, location, and concomitant glenoid bone loss must be evaluated in light of the patient’s symptoms. Recent literature suggests that Hill-Sachs lesions are best approached as bipolar April 2012, Vol 20, No 4 problems in which a glenoid defect is magnified in the setting of glenoid bone loss. The concept of the glenoid track advanced the understanding of engagement and recurrent instability by defining the humeral head deficiency in relation to glenoid width and bone loss. A meticulous approach to the diagnostic workup is essential and must include a complete history and thorough physical examination. Imaging and arthroscopic findings can aid in the decision-making process. Small lesions may be addressed solely on the glenoid side to increase the articular arc and prevent engagement. However, large Hill-Sachs defects may require combined procedures that directly address the humeral defect, including arthroplasty, humeral head allograft, remplissage, and resurfacing. References Evidence-based Medicine: Levels of evidence are described in the table of contents. In this article, references 10 and 13 are level II studies. References 5 and 17 are level III studies. References 2, 4, 11, 12, 14, 15, 18, 24, 26, 27, 30-34, 39, 40, 45, and 46 are level IV studies. References 7-9, 16, 20-23, 29, 35, 38, 41, 42, 44, 47, and 48 are level V expert opinion. References printed in bold type are those published within the past 5 years. 1. Hill HA, Sachs MD: The grooved defect of the humeral head: A frequently unrecognized complication of dislocations of the shoulder joint. Radiology 1940;35:690-700. 2. Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16(7):677-694. 3. Flatow EL, Warner JI: Instability of the shoulder: Complex problems and failed repairs. Part I: Relevant biomechanics, multidirectional instability, and severe glenoid loss. Instr Course Lect 1998;47: 97-112. 4. Rowe CR, Zarins B, Ciullo JV: Recurrent anterior dislocation of the shoulder after surgical repair: Apparent causes of failure and treatment. J Bone Joint Surg Am 1984;66(2):159-168. 5. Kim DS, Yoon YS, Yi CH: Prevalence comparison of accompanying lesions between primary and recurrent anterior dislocation in the shoulder. Am J Sports Med 2010;38(10):2071-2076. 6. Ghodadra N, Gupta A, Romeo AA, et al: Normalization of glenohumeral articular contact pressures after Latarjet or iliac crest bone-grafting. J Bone Joint Surg Am 2010;92(6):1478-1489. 7. Provencher MT, Bhatia S, Ghodadra NS, et al: Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am 2010;92(suppl 2):133151. 8. Piasecki DP, Verma NN, Romeo AA, Levine WN, Bach BR Jr, Provencher MT: Glenoid bone deficiency in recurrent anterior shoulder instability: Diagnosis and management. J Am Acad Orthop Surg 2009;17(8):482-493. 9. Armitage MS, Faber KJ, Drosdowech DS, Litchfield RB, Athwal GS: Humeral head bone defects: Remplissage, allograft, and arthroplasty. Orthop Clin North Am 2010;41(3):417-425. 10. Calandra JJ, Baker CL, Uribe J: The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy 1989;5(4):254-257. 11. Rowe CR, Patel D, Southmayd WW: The Bankart procedure: A long-term end-result study. J Bone Joint Surg Am 1978;60(1):1-16. 12. Saupe N, White LM, Bleakney R, et al: Acute traumatic posterior shoulder dislocation: MR findings. Radiology 2008;248(1):185-193. 13. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25(3):306-311. 14. Yiannakopoulos CK, Mataragas E, Antonogiannakis E: A comparison of the spectrum of intra-articular lesions in acute and chronic anterior shoulder instability. Arthroscopy 2007;23(9):985990. 15. Palmer I, Widén A: The bone block method for recurrent dislocation of the shoulder joint. J Bone Joint Surg Br 1948;30(1):53-58. 251 The Hill-Sachs Lesion: Diagnosis, Classification, and Management 16. 17. Lynch JR, Clinton JM, Dewing CB, Warme WJ, Matsen FA III: Treatment of osseous defects associated with anterior shoulder instability. J Shoulder Elbow Surg 2009;18(2):317-328. Richards RD, Sartoris DJ, Pathria MN, Resnick D: Hill-Sachs lesion and normal humeral groove: MR imaging features allowing their differentiation. Radiology 1994;190(3):665-668. 19. Chen AL, Hunt SA, Zuckerman JD: Humeral head impression fractures and head-splitting fractures, in Zuckerman JD, Koval KJ, eds: Shoulder Fractures: The Practical Guide to Management. New York, NY, Thieme Medical Publishers, 2005, pp 120-145. 21. Bollier MJ, Arciero R: Management of glenoid and humeral bone loss. Sports Med Arthrosc 2010;18(3):140-148. Hall RH, Isaac F, Booth CR: Dislocations of the shoulder with special reference to accompanying small fractures. J Bone Joint Surg Am 1959; 41(3):489-494. 23. Miniaci A, Gish M: Management of anterior glenohumeral instability associated with large Hill-Sachs defects. Techniques in Shoulder & Elbow Surgery 2004;5(3):170-175. 25. 26. 27. 252 Griffith JF, Yung PS, Antonio GE, Tsang PH, Ahuja AT, Chan KM: CT compared with arthroscopy in quantifying glenoid bone loss. AJR Am J Roentgenol 2007; 189(6):1490-1493. Cicak N, Bilić R, Delimar D: Hill-Sachs lesion in recurrent shoulder dislocation: Sonographic detection. J Ultrasound Med 1998;17(9):557-560. Franceschi F, Longo UG, Ruzzini L, Rizzello G, Maffulli N, Denaro V: Arthroscopic salvage of failed arthroscopic Bankart repair: A prospective study with a minimum follow-up of 4 years. Am J Sports Med 2008;36(7):1330-1336. Yamamoto N, Itoi E, Abe H, et al: Contact between the glenoid and the Provencher MT, Metzger PD, Peace WJ, Barlow B, Leonardelli D, Solomon DJ: Poster P294: Clinical grading of HillSachs injuries: Association with glenoid bone loss and humeral engagment. 77th Annual Meeting Proceedings. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2010, pp 617-618. 29. Purchase RJ, Wolf EM, Hobgood ER, Pollock ME, Smalley CC: Hill-Sachs “remplissage”: An arthroscopic solution for the engaging Hill-Sachs lesion. Arthroscopy 2008;24(6):723-726. 30. Weber BG, Simpson LA, Hardegger F: Rotational humeral osteotomy for recurrent anterior dislocation of the shoulder associated with a large HillSachs lesion. J Bone Joint Surg Am 1984; 66(9):1443-1450. 31. Pagnani MJ: Open capsular repair without bone block for recurrent anterior shoulder instability in patients with and without bony defects of the glenoid and/or humeral head. Am J Sports Med 2008;36(9):1805-1812. Scalise J, Miniaci A, Iannotti J: Resurfacing arthroplasty of the humerus: Indications, surgical technique, and clinical results. Techniques in Shoulder & Elbow Surgery 2007;8:152-160. 22. 24. 28. Mologne TS, Provencher MT, Menzel KA, Vachon TA, Dewing CB: Arthroscopic stabilization in patients with an inverted pear glenoid: Results in patients with bone loss of the anterior glenoid. Am J Sports Med 2007;35(8): 1276-1283. 18. 20. humeral head in abduction, external rotation, and horizontal extension: A new concept of glenoid track. J Shoulder Elbow Surg 2007;16(5):649-656. 32. 33. 34. 35. 36. Boileau P, Bicknell RT, El Fegoun AB, Chuinard C: Arthroscopic Bristow procedure for anterior instability in shoulders with a stretched or deficient capsule: The “belt-and-suspenders” operative technique and preliminary results. Arthroscopy 2007;23(6):593601. Burkhart SS, De Beer JF, Barth JR, Cresswell T, Roberts C, Richards DP: Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. Arthroscopy 2007;23(10): 1033-1041. Weng PW, Shen HC, Lee HH, Wu SS, Lee CH: Open reconstruction of large bony glenoid erosion with allogeneic bone graft for recurrent anterior shoulder dislocation. Am J Sports Med 2009;37(9):1792-1797. Provencher MT, Ghodadra N, LeClere L, Solomon DJ, Romeo AA: Anatomic osteochondral glenoid reconstruction for recurrent glenohumeral instability with glenoid deficiency using a distal tibia allograft. Arthroscopy 2009;25(4):446452. Diklic ID, Ganic ZD, Blagojevic ZD, Nho SJ, Romeo AA: Treatment of locked chronic posterior dislocation of the shoulder by reconstruction of the defect in the humeral head with an allograft. J Bone Joint Surg Br 2010;92(1):71-76. 37. Miniaci A, Gish MW: Management of anterior glenohumeral instability associated with large Hill–Sachs defects. Techniques in Shoulder & Elbow Surgery 2004;5(3):170-175. 38. Connolly JF: Humeral head defects associated with shoulder dislocation: Their diagnostic and surgical significance. Instr Course Lect 1972;21: 42-54. 39. Abdelhady AM: Neglected anterior shoulder dislocation: Open remplissage of the Hill-Sachs lesion with the infraspinatus tendon. Acta Orthop Belg 2010;76(2):162-165. 40. Deutsch AA, Kroll DG: Decreased range of motion following arthroscopic remplissage. Orthopedics 2008;31(5): 492. 41. Koo SS, Burkhart SS, Ochoa E: Arthroscopic double-pulley remplissage technique for engaging Hill-Sachs lesions in anterior shoulder instability repairs. Arthroscopy 2009;25(11):1343-1348. 42. Wolf EM, Pollock ME, Smalley CC: HillSachs “remplissage”: An arthroscopic solution for the engaging Hill-Sachs lesion. Arthroscopy 2007;23(6):e1-e2. 43. Kazel MD, Sekiya JK, Greene JA, Bruker CT: Percutaneous correction (humeroplasty) of humeral head defects (Hill-Sachs) associated with anterior shoulder instability: A cadaveric study. Arthroscopy 2005;21(12):1473-1478. 44. Re P, Gallo RA, Richmond JC: Transhumeral head plasty for large HillSachs lesions. Arthroscopy 2006;22(7): 798, e1-e4. 45. Moros C, Ahmad CS: Partial humeral head resurfacing and Latarjet coracoid transfer for treatment of recurrent anterior glenohumeral instability. Orthopedics 2009;32(8). 46. Pritchett JW, Clark JM: Prosthetic replacement for chronic unreduced dislocations of the shoulder. Clin Orthop Relat Res 1987;(216):89-93. 47. McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;24(3):584-590. 48. Krackhardt T, Schewe B, Albrecht D, Weise K: Arthroscopic fixation of the subscapularis tendon in the reverse HillSachs lesion for traumatic unidirectional posterior dislocation of the shoulder. Arthroscopy 2006;22(2):227, e1-e227, e6. Journal of the American Academy of Orthopaedic Surgeons