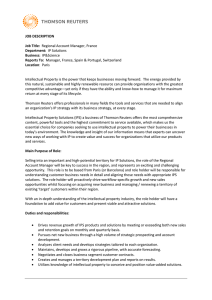
RESEARCH ARTICLE WISC-V Profiles and Their Correlates in Children with Autism Spectrum Disorder without Intellectual Developmental Disorder: Report from the ELENA Cohort Lee Audras-Torrent, Ela Miniarikova, Flore Couty, Florine Dellapiazza, Mathilde Berard, Cécile Michelon, Marie-Christine Picot, and Amaria Baghdadli The intellectual functioning of people with autism spectrum disorder (ASD) without intellectual developmental disorder (IDD) has not been widely studied. However, marked heterogeneity in assessment measures, samples, and results has been an obstacle for the generalization of findings. We aimed to (a) describe WISC-V intellectual functioning in a sample of children with autism spectrum disorder without intellectual developmental disorder, (b) identify WISC-V profiles, and (c) explore whether WISC-V intellectual functioning is related to ASD symptom severity and adaptive skills. Our sample consisted of 121 children from 6 to 16 years of age with ascertained ASD without an intellectual developmental disorder (IDD). The intellectual functioning of the participants was within the average range. Intra-individual analysis showed that children with ASD performed better on visual than auditory working-memory tasks. Moreover, the intellectual functioning of the participants correlated negatively with ASD symptom severity but positively with adaptive communication skills. Overall, we identified six intellectual profiles according to verbal and reasoning skills. These findings highlight the relevance of WISC-V assessment for children with ASD without an IDD to individualize intervention, especially remediation. Autism Res 2021, 14: 997–1006. © 2020 International Society for Autism Research, Wiley Periodicals, LLC Lay Summary: This study examined WISC-V intellectual functioning in 121 children with autism spectrum disorder (ASD) without an intellectual developmental disorder (IDD). We found their intellectual functioning to be within the average, as was that of their peers with typical development (TD), and their verbal and reasoning skills were the most discriminant. In addition, the better their intellectual functioning was, the better their adaptive communication skills and the less severe their ASD symptoms. These findings highlight the relevance of WISC-V assessment in ASD to individualize early psychological remediation. Keywords: autism spectrum disorder; children; intellectual functioning; WISC-V; profiles; adaptive functioning Introduction Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by social communication impairment, associated with stereotyped and repetitive patterns in behavior, interests, or activities [American Psychiatric Association, 2013]. Intellectual developmental disorders (IDDs) are frequently associated with ASD, its estimated prevalence in ASD being 50% in France [Mottron, 2010]. It is well known that IDDs have a negative impact on overall functioning in ASD [American Psychiatric Association, 2013; Matson & Shoemaker, 2009]. Intellectual functioning refers to complex, higher-order forms of cognition, such as reasoning, problem solving, and decision making [Dai & Sternberg, 2004]. It has been widely studied in ASD, but many studies have excluded participants with IDD from their sample to reduce clinical heterogeneity [Black, Wallace, Sokoloff, & Kenworthy, 2009; Lai et al., 2017; Mayes & Calhoun, 2008; Oliveras-Rentas, Kenworthy, Roberson 3rd, Martin, & Wallace, 2012]. Overall, available studies often report strengths and weaknesses in intellectual functioning of children with ASD. Indeed, they found that individuals with ASD commonly have higher performance reasoning (i.e., nonverbal performances) than verbal scores [Girardot et al., 2012; Hedvall et al., 2013; Oliveras-Rentas et al., 2012]. In addition, studies using various Wechsler Intelligence Scales (WIS; WPPSI-III, From the Centre de Ressource Autisme Languedoc-Roussillon, Centre d’Excellence sur l’Autisme et les Troubles Neurodéveloppementaux (CeAND), Montpellier, France (L.A.-T., E.M., F.C., F.D., M.B., C.M., A.B.); Université Paris-Saclay, UVSQ, Inserm, CESP, Team DevPsy, Villejuif, France (M.-C.P., A.B.); Department of Medical Information, University Hospital, Montpellier, France (M.-C.P.); Faculté de Médecine, Université de Montpellier, Montpellier, France (A.B.) Received July 15, 2020; accepted for publication November 9, 2020 Address for correspondence and reprints: Amaria Baghdadli, Centre de Ressource Autisme Languedoc-Roussillon, Centre d’excellence sur l’autisme et les troubles neurodéveloppementaux, 191 Avenue du Doyen Gaston Giraud, Montpellier 34000, France. E-mail: rech-clinique-autisme@chumontpellier.fr Published online 27 November 2020 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/aur.2444 © 2020 International Society for Autism Research, Wiley Periodicals, LLC INSAR Autism Research 14: 997–1006, 2021 997 WISC-III, WISC-IV, and WIAT-II) have shown that visual supports used during psychological examinations of children with ASD improved their overall intellectual skills [Girardot et al., 2012; Mayes & Calhoun, 2008; Samson, Mottron, Soulières, & Zeffiro, 2012]. Several authors have also suggested that discrepancies between verbal and performance reasoning skills found with WIS are markers of ASD [Black et al., 2009; Oliveras-Rentas et al., 2012]. Processing speed (PS) and working memory (WM) were found to be poor in people with ASD [Boucher, Bigham, Mayes, & Muskett, 2008; Habib, Harris, Pollick, & Melville, 2019; Mayes & Calhoun, 2008; Oliveras-Rentas et al., 2012; Wang et al., 2017]. A recent meta-analysis highlighted that individuals with ASD have poorer WM than those with typical development (TD), with spatial WM being poorer than verbal WM [Wang et al., 2017]. Finally, studies have highlighted that overall intellectual functioning is lower in people with ASD than those with TD [Dawson, Soulières, Gernsbacher, & Mottron, 2007; Nader, Courchesne, Dawson, & Soulières, 2016; Scheuffgen, Happé, Anderson, & Frith, 2000] but these findings were obtained using a wide range of IQ assessments. WIS are the most frequently administered instruments to measure overall intelligence in the general population [Oliveras-Rentas et al., 2012; Weiss, Saklofske, Holdnack, & Prifitera, 2015]. Various measures of intellectual functioning, such as Raven Progressive Matrices were used [Bölte, Dziobek, & Poustka, 2009; Dawson et al., 2007; Nader et al., 2016]. However, authors have found that WIS provides reliable measures of intellectual skills in individuals with ASD without IDD [Bölte et al., 2009; Oliveras-Rentas et al., 2012]. The latest version of the Wechsler Intelligence Scale for Children, the WISC-V (2016), has undergone changes that could make it useful for studying intellectual functioning in ASD. First, the Perceptual Reasoning Index (PRI) is now split into two domains: the Visuo-Spatial Index (VSI) and the Fluid-Reasoning Index (FRI), the FRI being a good marker of intellectual functioning in ASD [Terriot & Ozenne, 2015]. Second, the Comprehension Subtest Score, which often corresponds to a weak point in ASD [Dawson et al., 2007; Oliveras-Rentas et al., 2012], is no longer required to calculate the Full-Scale Intelligence Quotient (FSIQ). This change could be at the origin of higher scores for individuals with ASD for the Verbal Comprehension Index (VCI) with the WISC-V than with the WISC-IV [Kuehnel, Castro, & Furey, 2019]. Third, a new subtest, Picture Span, assesses visual WM, which can capture the strengths in visual and perceptive reasoning often reported in ASD [Girardot et al., 2012]. However, the intellectual functioning of children with ASD has not yet been thoroughly studied using the WISC-V, except for verbal skills [Kuehnel et al., 2019]. 998 Furthermore, studies using WIS have reported that intellectual functioning in ASD is linked to several clinical dimensions. Significant associations were found between intellectual functioning and ASD symptom severity: verbal skills (VCI) negatively correlated with ADOS communication and social-interaction scores [Black et al., 2009; Oliveras-Rentas et al., 2012], and processing speed (PSI) negatively correlated with the ADOS communication score [Oliveras-Rentas et al., 2012]. Black et al. [2009] also found a relationship between intellectual functioning and adaptive skills, verbal and non-verbal intellectual functioning being strongly associated with adaptive communication skills. Oliveras-Rentas et al. [2012] found that the VCI, PRI, WM index (WMI), and PSI were positively associated with adaptive communication skills. Hedvall et al. [2013] highlighted that processing speed influenced adaptive functioning in communication, motor, and daily living skills. These relationships between intellectual functioning in ASD without IDD, ASD symptom severity, and adaptive functioning require further investigation to better characterize the needs of this population. A recent study suggested the existence of distinct intellectual profiles among children with ASD [Silleresi et al., 2020]. The authors studied language abilities and non-verbal intellectual functioning using Raven’s Progressive Matrices (RPM) and WISC-IV Matrix Reasoning and Block Design in a sample of 51 verbal children with ASD without IDD. Their results showed five intellectual profiles according to the participants’ language skills: (a) ASD with normal language (LN) and low non-verbal intellectual quotient (NVIQ), (b) ASD with impaired language (LI) and low NVIQ, (c), ASD with LN and average NVIQ, (d), ASD with LI and average NVIQ, and (e) ASD with LN and high NVIQ. The strengths of this study were that it provided an accurate description of the intellectual functioning of children with ASD without IDD using WISC-V and that it investigated its links with language functioning. The study of the multiple dimensions of intellectual functioning, such as working memory, visuospatial treatment, processing speed, and fluid reasoning, in children with ASD without IDD could help to identify specific characteristics of their intellectual profile. The literature shows that it is possible to identify distinct intellectual profiles in children with ASD [Black et al., 2009] using various measurement instruments. WISC-V appears to be a relevant and efficient tool to measure, in particular, verbal intellectual functioning in ASD [Kuehnel et al., 2019], but its use has not yet been extended to all intellectual domains of interest in clinical practice. One of the important benefits would be the tailoring of intervention and education to individual functioning [Oliveras-Rentas et al., 2012]. We aimed to assess WISC-V intellectual functioning in children with ASD without IDD and to explore the associations between WISC-V Audras-Torrent et al./WISC-V in children with ASD without IDD INSAR profiles, ASD symptom severity, and adaptive functioning. Indeed, only a limited number of studies have investigated the intellectual profiles of children with ASD without IDD [Baghdadli et al., 2019; Joseph, Steele, Meyer, & Tager-Flusberg, 2005]. Moreover, there are currently few studies that used WISC-V to study the intellectual functioning of children with ASD without IDD. The challenge of using WISC-V is to contribute to a detailed description of the intellectual profiles of children with ASD and study their relationship with ASD symptom severity and adaptive functioning to improve our understanding of their individual functioning and tailor treatment approaches. Based on the literature, we hypothesized that there would be considerable heterogeneity in intellectual functioning, characterized by strengths in the VSI and FSI and weaknesses in the PSI and WMI and that, within the WMI, participants would perform better on the visual Picture Span subtest than on the verbal Digit Span subtest. We also hypothesized that ASD symptom severity would be negatively associated with WISC-V indexes, particularly the VCI and PSI. Finally, we predicted that there would be positive associations between adaptive communication skills and WISC-V indices, especially the VCI. Exploring this link may help to better understand the impact of language difficulties in ASD without IDD. Methods Participants Participants were recruited from the ELENA cohort, a large multi-center, longitudinal, prospective cohort of children with an ascertained ASD [Baghdadli et al., 2019]. Participants were recruited from 15 centers across nine of the 18 French regions. Overall, 900 children were recruited for this longitudinal study with parental consent. The inclusion criteria for the ELENA cohort were to be aged from 2 to 16 years at the moment of the diagnosis of ASD and to have a diagnosis ascertained by a multidisciplinary, clinical, and standardized process administered by licensed and trained psychologists. Measures included the Autism Diagnostic Observation Schedule 2 (ADOS-2) [Lord et al., 2012], the Autism Diagnostic Interview-Revised (ADI-R) [Le Couteur, Lord, & Rutter, 2003], a direct psychological examination to estimate the Intellectual Quotient (WISC-V) [Wechsler, 2014], and a parental interview about the child’s adaptive functioning using the parent/caregiver Vineland Adaptive Behavior Scale (VABS-II) [Sparrow, Cicchetti, & Balla, 2005]. Parents also completed online questionnaires and medical and interventional data. For the present study, we used a subgroup of 121 participants from the ELENA cohort selected according to the following inclusion criteria: aged from 6 to 16 years, INSAR having completed all 10 subtests of the WISC-V, and having scores on both the WISC-V and VABS-II ≥70. The children included in our study were only those who were able to participate in the full WISC-V protocol, implying that they had adequate verbal skills to understand and answer verbal instructions. Exclusion criteria were having an IDD (Full-Scale Intelligence Quotient ≤70 for the WISC-V, a total adaptive score of the VABS-II ≤70, and ICM F70, F71, F72), or sensory disabilities, such as blindness or deafness (n = 4), according to clinical examinations and self-completed parental questionnaires concerning the potential co-occurrence of sensory disabilities. Measures Intellectual functioning of participants was assessed using the French form of the WISC-V administrated by licensed and trained psychologists. The WISC-V is composed of 10 primary subtests (represented by scaled scores: mean = 10, standard deviation = 3) that can be clustered into composite quotients for five indices (represented by standard scores: mean = 100, standard deviation = 15) (described in Table 1). Only the first seven subtests are used to calculate the Full-Scale Intelligence Quotient (FSIQ). The internal consistency indicators attest to excellent reliability; alpha indices range from 0.88 to 0.96. Moreover, the measures are considered to be stable over time. Concerning the validity of the scale, links between the subtests within a given index are strong (on average > 0.70) [Terriot & Ozenne, 2015]. Adaptive functioning was assessed using the parent/caregiver form of the VABS-II [Sparrow et al., 2005]. This standardized caregiver interview of 297 items measures adaptive behaviors in the domains of communication, daily living skills and socialization. The reliability of the VABS-II for each domain was excellent (α = 0.80) and the intra-class coefficient of the test/retest 0.89. ASD symptom severity was measured using the ADOS-2 [Lord et al., 2012] a semi-structured behavioral observation protocol. This scale is composed of 25 to 30 items across social interaction, communication, repetitive and Table 1. Subtests and Indices of the WISC-V Indices Verbal Comprehension Index (VCI) Visual–spatial Index (VSI) Fluid Reasoning Index (FRI) Working Memory Index (WMI) Processing Speed Index (PSI) Audras-Torrent et al./WISC-V in children with ASD without IDD Subtests Similarities [SI] Vocabulary [VC] Block Design [BD] Visual Puzzles [VP] Matrix Reasoning [MR] Figure Weight [FW] Digit Span [DG] Picture Span [PS] Coding [CD] Symbol Search [SS] 999 stereotyped behaviors, and play domains. The internal consistency was good (α = 0.50–0.92), the test–retest reliability acceptable (0.64–0.88), and the inter-rater reliability excellent (0.79–0.98). For this study, we used the Calibrate Severity Score (CSS), ranging from 1 to 10. A diagnosis of Attention Deficit Hyperactivity Disorder (ADHD) or Developmental Coordination Disorder (DCD) was collected at inclusion and systematically completed using the ICM-10 medical diagnosis (F90 and F82, respectively) and medical records after being established by a child psychiatrist. The parent occupation was recorded for the mother and father and coded into eight categories: 1 – Agricultural worker; 2 – Craftsman, sale worker, or entrepreneur; 3 – Manager, engineer, or doctor; 4 – Intermediate occupation; 5 – Employee; 6 – Worker; 7 – Retired; 8 – No professional occupation. Procedure This study was cross-sectional in that it used intellectual measurements from WISC-V for each participant that could be entirely collected at one of the timepoints of the prospective follow-up of the ELENA cohort (at inclusion, 3 years later, or 6 years later). At each timepoint, the intellectual measurements were collected simultaneously with other data, including that of the VABS-II [Sparrow et al., 2005] and ADOS-2 [Lord et al., 2012]. Data Analysis Descriptive statistics were generated for all measures to provide an overview of the children’s characteristics in the entire sample. For the first aim, we performed intraindividual analysis between the 10 WISC-V subtests using the Wilcoxon signed rank test, for which we calculated index differences (Δ) for each participant. For the second aim, we studied intergroup comparisons between sex, age, VABS-II adaptive scores, ADOS-2 CSS (independent variables), and the scores for the WISC-V indices and subtests (dependent variables) using Spearman correlation coefficients, except for the independent variable, sex, for which ANOVA was used. Finally, hierarchical cluster analysis (HCA) was performed on the entire sample using squared Euclidian distance proximity measures [Hair, Black, Grimm, & Yarnold, 2000] and Ward’s minimumvariance method [Ward, 1963]. This classification into homogeneous subgroups was based on the 10 subtests of the WISC-V (SI, VC, BD, MR, FW, DS, CD, VP, PS, and SS). Cluster analysis aims to maximize between-cluster variance relative to within-cluster variance. The number of clusters chosen was based on three graphical methods: (a) the cubic clustering criterion, (b) semi-partial R2 [Milligan & Cooper, 1985], and (c) a dendrogram that reflected the hierarchy of the clusters. Analyzes were conducted to assess cluster group differences in WISC-V scores and clinical characteristics using chi square for nominal variables (sex) or ANOVA for continuous variables (age, VABS-II scores). The analyzes were conducted using SAS® version 9.3 statistical software. Results Participants The 121 participants were aged from 6 years to 16 years and 11 months (mean age 10.7 ± 2.7 years). Their clinical characteristics and psychiatric comorbidities are presented in Table 2. The parent occupation of mothers covered the following categories: employee (46.4%), worker (43. 6%), manager (21.4%), intermediate occupation (12.5%), craftsman (8.9%), and without professional Table 2. Clinical Characteristic of the Children n % 102 19 84.3 15.7 40 81 24 13 33.1 66.9 19.8 10.7 Measures ADOS-2 Severity score n 115 Mean 7.5 SD 2.0 VABS II score Communication Daily living skills Socialization 121 80.8 71.1 75.7 10.3 9.7 10.5 Sex Male Female Age 6–11.11 years 12–16.11 years Psychiatric comorbidities ADHD (F90) DCD (F82) ADHD: attention deficit hyperactivity disorder; DCD: developmental coordination disorder. 1000 Audras-Torrent et al./WISC-V in children with ASD without IDD INSAR occupation (7.1%). The parent occupation of fathers covered the following categories: employee (30.7%), manager (28.8%), craftsman (19.2%), worker (15.4%), intermediate occupation (3.8%), and without professional occupation (2%). The ASD symptom severity score on the ADOS-2 (CSS) was assessed as high for 54.8% (scores from 8–10), moderate for 35.7% (scores from 5–7), and mild for 9.5% (scores <4). For most of these children, it was possible to administer ADOS-2 modules 3 and 4 (module 3 for 81% and module 4 for 4.2%), with module 2 having been used for the others in spite a correct language level (verified in the medical report). The mean communication, socialization, and daily living skills VABS-II scores ranged from low to moderate. Intellectual Functioning and Intra-Individual Analysis for Indices and Subtests Within the entire sample, all mean index and subtest scores were in the mean range relative to those of typical children (Table 3). Intra-individual analysis showed significant differences between indexes scores using the Wilcoxon signed rank test. VCI scores were higher than WMI scores (100.8 ± 20.2 vs. 94.0 ± 13.6, Δ = 6.8, P < 0.001) and PSI scores (100.8 ± 20.2 vs. 93.2 ± 14.1, Δ = 7.6, P < 0.001). FRI scores were higher than WMI scores (102.0 ± 14.0 vs. 94.0 ± 13.6, Δ = 8.1, P < 0.001) and PSI scores (102.0 ± 14.0 vs. 94.0 ± 14.1, Δ = 9.0, P < 0.001). VSI scores were higher than PSI scores (102.2 ± 14.6 vs. 93.2 ± 14.1 scores, Δ = 9.0, P < 0.001) and WMI scores (102.0 ± 14.6 vs. 94.0 ± 13.6 scores, Δ = 8.2, P < 0.001). We observed no significant differences between VCI and FRI, VSI and FRI, or WMI and PSI. Intra-individual analysis between FSIQ and index scores showed the VSI (Δ = −3.4, P = 0.005) and FRI (Δ = −3.2, P < 0.001) to be higher than the FSIQ and the PSI Table 3. Description of WISC-V Scores by Index and Subtest WISC-V Indexes Verbal Comprehension Index Visual Spatial Index Fluid Reasoning Index Working Memory Index Processing Speed Index Full-Scale IQ WISC-V Subtests Similarities Vocabulary Block Design Visual Puzzles Matrix Reasoning Figure Weights Digit Span Picture Span Coding Symbol Search INSAR Mean 100.8 102.2 102.0 94.0 93.2 98.9 Mean 10.5 9.7 10.3 10.5 10.1 10.5 8.5 9.5 8.6 9.0 SD 20.2 14.6 14 13.6 14.0 15.7 SD 3.8 4 2.8 2.9 2.6 2.8 2.6 2.8 3.0 2.8 Min 45 61 72 65 60 70 Min 1 1 2 4 4 4 1 4 1 3 Max 155 141 127 125 129 147 Max 19 19 18 17 16 16 14 16 17 16 (Δ = 5.7, P < 0.001) and WMI (Δ = 4.9, P < 0.001) to be lower. However, the VSI scores were similar to the FSIQ scores (P < 0.08). Intra-individual analysis showed only one significant difference for the subtest scores (Δ = 0.9, P < 0.001), participants having a higher score for the Picture Span (9.5 ± 2.9) than Digit Span (8.5 ± 2.6). Comparisons of Intellectual Functioning across Sex-AgeParent Occupation-ASD Symptom Severity-Adaptive Skills Intergroup comparisons of index and subtest scores showed no significant differences due to sex (all P < 0.05). Intergroup comparisons between children aged from 6 years to 11 years, 11 months and those aged from 12 years to 16 years, 11 months showed significant differences with higher scores for the older group for the VCI (106.7 ± 19.6 vs. 97.9 ± 20.0, P < 0.03), Vocabulary subtest (10.8 ± 3.9 vs. 9.2 ± 3.9, P = 0.04), and Similarities subtest (11.5 ± 3.8 vs. 10.1 ± 3.7, P = 0.04). There were no significant differences between age groups for the other indices and subtests (all P > 0.05). We examined the effect of parents’ occupation on their children’s FSIQ and found that children whose mothers were employees (96.5 ± 12.8) had a significantly lower FSIQ than those whose mothers were managers (114.2 ± 12.5, P = 0.02). However, there was no effect of the fathers’ occupation on their children’s FSIQ (P = 0.5). We also examined correlations between ASD symptomseverity scores and index and subtest scores. For the indices, the ASD symptom-severity scores negatively correlated with the VCI score (r = −0.20, P = 0.03), VSI score (r = −0.27, P = 0.004), and FSIQ (r = −0.20, P = 0.03). Thus, the FSIQ, VCI, and VSI scores decreased with increasing ASD severity score. For the subtests, the ASD symptom severity scores negatively correlated with the Block Design score (r = −0.19, P = 0.04) and Visual Puzzle score (r = −0.28, P = 0.003). Thus, the Block Design and Visual Puzzle scores decreased with increasing global ASD symptom severity score. We then examined correlations between the indices and domains of the VABS-II. The VABS-II communication score positively correlated with all indices. Thus, with an increasing Vineland communication score, the FSIQ (r = 0.50; P = 0.0001), VCI (r = 0.49; P = 0.0001), FRI (r = 0.36; P = 0.001), VSI (r = 0.31; P = 0.0005), WMI (r = 0.38; P = 0.001), and PSI scores (r = 0.38; P = 0.0001) also increased. The daily living skills score also positively correlated with the VSI (r = 0.22; P = 0.01), FRI (r = 0.21; P = 0.02), and FSIQ scores (r = 0.21; P = 0.02). Finally, there were no correlations between the Vineland Socialization score and the indices (all P > 0.05). In our sample, ASD-symptom severity measured by the ADOS-2 negatively correlated with adaptive functioning measured by the VABS-II for communication (r = −0.34; P = 0.01), Audras-Torrent et al./WISC-V in children with ASD without IDD 1001 socialization (r = −0.31; P = 0.01), and daily living skills (r = −0.23; P = 0.01). Cluster Analysis of Intellectual Profiles The 10 WISC-V Subtests scores allowed us to discriminate between subgroups in the entire sample. The agglomeration coefficients (Pseudo-F statistic, pseudo-T2, Semipartial R2, and cubic clustering criteria) and dendrogram generated by the cluster analysis suggested a six-cluster solution (Fig. 1). Based on the Subtests scores of these six clusters, titles were proposed for each cluster concerning verbal skills (SI, VC) and reasoning (BD, VP, MR, FW) Subtests’ differences. Scores equal or below 8 are considered as “low,” scores between 9 to 11 are considered as “average,” and scores equal or above 12 are considered as “high.” One subgroup had homogenous scores, with average scores for all subtests (cluster 2, n = 23), named the Average Scores (AS) profile. The other five subgroups had heterogeneous scores. Two subgroups showed low average scores, the first with average reasoning scores (cluster 1, n = 33), named the Low Scores with Average Reasoning (LSAR) subgroup, and the second with average verbal scores (cluster 3, n = 11), named the Low Scores with Average Verbal (LSAV) subgroup. Finally, three subgroups showed average scores: high average reasoning scores for cluster 4 (n = 20), called the Average Scores with Figure 1. 1002 High Reasoning (ASHR) subgroup; high average verbal scores for cluster 5 (n = 20), called the Average Scores with High Verbal (ASHV) subgroup; and both high verbal and reasoning scores for cluster 6 (n = 14), called the Average scores with High Verbal/Reasoning (ASHVR) subgroup. The cluster results for the ten WISC-V Subtests scores are presented in Figure 1. Comparison of the clusters showed no significant difference in age (P = 0.3) or ASD symptom-severity score (P = 0.08). The percentage of psychiatric comorbidities by cluster is shown in Table 4. For the VABS-II scores, comparison of the clusters showed significant differences in the communication scores. The LSAR subgroup had a lower score than that of the AS (73.9 ± 7.9 vs. 83.0 ± 11.0, P < 0.001), ASHR (73.9 ± 7.9 vs. 83.0 ± 8.5, P < 0.001), ASHV (73.9 ± 7.9 vs. 84.6 ± 10.0, P < 0.001), and ASHVR (73.9 ± 7.9 vs. 87.8 ± 11.4, P < 0.001) subgroups. However, there were no significant differences between clusters for VABSII socialization and daily living skills (all P > 0.05), as represented in Figure S1. Discussion We examined overall WISC-V intellectual functioning in children with ascertained ASD without IDD. As expected, there was marked heterogeneity in the WISC-V indexes Mean subtest-scaled scores for each cluster. Audras-Torrent et al./WISC-V in children with ASD without IDD INSAR Table 4. Percentage of Psychiatric Comorbidities by Cluster ADHD (F90), % (n) DCD (F82), % (n) ASHVR (n = 14) ASHR (n = 20) ASHV (n = 20) AS (n = 23) LSAR (n = 33) LSAV (n = 11) Intergroup differences 21.4 (3) 7.1 (1) 20 (4) 10 (2) 15 (3) 15 (3) 13.0 (3) 8.7 (2) 21.1 (7) 6.1 (2) 36.4 (4) 27.3 (3) ns ns AS: average scores; ASHR: high average reasoning; ASHV: average scores with high verbal; ASHVR: average scores with high reasoning; LSAR: low scores with average reasoning; LSAV: low scores with average verbal; ns: non significant. and subtests. Intra-individual analyzes showed the VCI, FRI, and VSI to be significantly higher than the WMI, PSI, and FSIQ (except VCI, which was quasi equal). Previous studies have also reported that children with ASD have strengths in performance reasoning skills [Girardot et al., 2012; Mayes & Calhoun, 2008; Scheuffgen et al., 2000], perhaps enhanced by the motor-free design of the intellectual tasks that were used [Oliveras-Rentas et al., 2012]. Charman et al. [2011] and Nader et al. [2016] showed that people with ASD have higher visual–spatial and abstract reasoning abilities, which may be specific markers of their intellectual functioning. In our sample, as well as in previous studies, the mean VABS-II Communication, Socialization, and Daily Living Skills scores were lower than the mean FSIQ scores [Charman et al., 2011; Flanagan et al., 2015; Matthews et al., 2015; Yang, Paynter, & Gilmore, 2016]. This result suggests that many individuals with ASD have problems in converting their intellectual skills into efficient adaptive skills [Charman et al., 2011; Tillmann et al., 2019]. It is well recognized that people with ASD and average intellectual functioning are not spared from adaptive difficulties [Charman et al., 2011; Kraper, Kenworthy, Popal, Martin, & Wallace, 2017]. Consequently, the term “highfunctioning” should be used with caution for the population of individuals with ASD without IDD [Alvares et al., 2020]. Furthermore, the Working Memory (WMI) of the children in our sample was poorer than their Verbal (VCI), Fluid Reasoning (FRI), Visuo-Spatial (VSI), and Global Intellectual Skills (FSIQ), in accordance with the results of previous studies [Mayes & Calhoun, 2008; Wang et al., 2017]. A low WMI could be attributed to the attention and language comprehension problems commonly found in ASD [Hedvall et al., 2013; Mayes & Calhoun, 2008; Oliveras-Rentas et al., 2012]. The results in the literature concerning WM have been contradictory, with some studies finding no differences between spatial and verbal WM in ASD [Joseph et al., 2005], whereas others found that spatial WM was more highly impaired in this population [Lai et al., 2017; Wang et al., 2017]. We found better visual than auditory WM among our participants. This could be due to the visual component of the Picture Span subtest, which may have helped the participants to maintain their attention [Girardot et al., 2012]. INSAR In our findings, child’s FSIQ was associated to mother occupation. Indeed, children whose mothers were employees had a lower FSIQ than children whose mothers were managers. This result is concordant with past literature [Delobel-Ayoub et al., 2015; Piccolo, Arteche, Fonseca, Grassi-Oliveira, & Salles, 2016], which highlight the need to focus attention more on family contextual factors in adapting the child intervention and family support plan. Our study also highlighted the presence of links between WISC-V intellectual functioning and several clinical dimensions of ASD. We observed a negative correlation between intellectual functioning, particularly verbal and visual–spatial skills, and the ASD symptomseverity score. These findings replicate those of previous studies [Black et al., 2009; Oliveras-Rentas et al., 2012] that showed lower intellectual verbal skills to be related to greater impairment of communication and socialization, measured by the ADOS [Joseph et al., 2005; Klin et al., 2007]. The finding of weak associations between ADOS-2 and WISC-V scores requires further studies on larger samples. Furthermore, our results show that overall intellectual functioning is strongly related to adaptive functioning, especially to VABS-II communication skills, as previously reported in the literature [Oliveras-Rentas et al., 2012]. The observation that visual–spatial and fluid reasoning in children with ASD is related to daily living skills reinforces the evidence that intellectual functioning influences daily life functioning [Black et al., 2009]. We then performed a cluster analysis on our sample and identified six WISC-V profiles, the cluster-based differences mainly covering verbal and reasoning skills, previously reported to be discriminant in ASD [Black et al., 2009; Girardot et al., 2012; Mayes & Calhoun, 2008; Mottron, 2004; Oliveras-Rentas et al., 2012; Silleresi et al., 2020]. The subgroup with the highest intellectual scores in all domains and strengths in both verbal and reasoning skills (ASHVR) was that with the fewest children with associated psychiatric conditions (28.6%). At the opposite extreme, the subgroup with the lowest scores in all domains, except verbal (LSAV), was that with the most children with associated conditions (63.6%). The VABS-II scores did not differ between the groups, except in the domain of communication, for which the LSAR group had lower scores than the others, possibly related to lower verbal skills. Audras-Torrent et al./WISC-V in children with ASD without IDD 1003 Our study had several strengths, including a large sample of children with an ascertained ASD who underwent a full clinical assessment, including administration of the entire WISC-V scale. Our results, however, need to be interpreted in the light of certain limitations. First, we excluded children with IDD from our sample to identify specific patterns in intellectual functioning, implying that our results cannot be generalized. Second, we did not use a control group of children with TD to verify the specificity of our results. As weaknesses in verbal working memory and processing speed in ASD may be related to attention, graphomotricity, and language difficulties, it is necessary to promote early and targeted developmental intervention. Indeed, early language training improves the overall outcome in ASD [Warren et al., 2011]. Also, several authors have suggested that the motor skills involved in processing speed could be improved by innovative training programs, such as a mechatronic door training kit [Moorthy, Iyer, Krishnan, & Pugazhenthi, 2019]. Moreover, cognitive remediation used in ASD could positively influence a range of cognitive dimensions, learning, and daily living skills, and improve the quality of life [Doyen et al., 2020; McConnell, 2002]. Although our results suggest that the verbal skills of children improved as they got older, further prospective studies are needed to better describe the course of intellectual functioning in ASD over time. Moreover, as children with ASD and IDD were excluded from our sample, future studies should also include individuals with IDD to examine their psychological profile with appropriate psychological assessments. There is also a need to study the influence of associated neurodevelopmental disorders in ASD, especially ADHD, frequently found in ASD, on psychological functioning. In conclusion, intellectual functioning assessed by the WISC-V in children with ASD without IDD shows common patterns. In addition, children with ASD without IDD had a poor auditory WM relative to their visual WM that could not be previously explored with previous versions of the WIS. Intellectual functioning measured by the WISC-V positively correlated with adaptive functioning measured by the VABS-II, but both intellectual and adaptive functioning negatively correlated with ASD-symptom severity measured by the ADOS-2. Intellectual functioning of the children, based on the WISC-V scores, could be divided into six profiles according to their verbal and reasoning skills. These findings highlight the relevance of WISC-V assessment in ASD to individualize early psychological remediation. Future studies are needed to describe the evolution of these intellectual functioning profiles in ASD during childhood and to assess effects of remediation. 1004 Acknowledgments The authors thank the contributing families and the ELENA cohort staff (Myriam Soussana, Julie Loubersac, Laetitia Ferrando, Philippe Antoine, and Colette Boy). The authors express gratitude to the CNSA and DGOS for funding to conduct this research and prepare the results for publication. Grant sponsor 1: French Health Ministry (DGOS) PHRCN 2013, grant number 1: 13–0232; and Grant sponsor 2: Caisse Nationale de Solidarité pour l’Autonomie (CNSA), grand number 2: 030319. Conflict of Interest The authors have no conflicts of interest to declare. Ethical Approval This study and informed consent procedure have been approved by the Ethics Committee on the Research of Human Subjects at Marseille Mediterranean (CNIL number DR-2015-393). Informed Consent Signed informed consent is obtained from all participating families included in the ELENA cohort. Author Contributions L.A.T., E.M., F.C., F.D., and M.B. conceived the study; contributed to the collection, analysis, and interpretation of the data; and drafted the manuscript. A.B. is the PI of the ELENA cohort and also participated in the design of the current study, drafted the manuscript, and critically revised it for main intellectual content. C.M. and M.-C. P. analyzed and interpreted the data. All authors read and approved the final version to be published. References Alvares, G. A., Bebbington, K., Cleary, D., Evans, K., Glasson, E. J., Maybery, M. T., … Whitehouse, A. J. O. (2020). The misnomer of ’high functioning autism’: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism, 24(1), 221–232. https://doi.org/10.1177/ 1362361319852831 American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Washington, DC: American Psychiatric Pub. Baghdadli, A., Miot, S., Rattaz, C., Akbaraly, T., Geoffray, M. M., Michelon, C., … ELENA Study Group. (2019). Investigating the natural history and prognostic factors of ASD in children: The multicEntric Longitudinal study of childrEN with ASD – Audras-Torrent et al./WISC-V in children with ASD without IDD INSAR the ELENA study protocol. BMJ Open, 9(6), e026286. https:// doi.org/10.1136/bmjopen-2018-026286 Black, D. O., Wallace, G. L., Sokoloff, J. L., & Kenworthy, L. (2009). Brief report: IQ split predicts social symptoms and communication abilities in high-functioning children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(11), 1613–1619. https://doi.org/10. 1007/s10803-009-0795-3 Bölte, S., Dziobek, I., & Poustka, F. (2009). Brief report: The level and nature of autistic intelligence revisited. Journal of Autism and Developmental Disorders, 39(4), 678–682. https://doi. org/10.1007/s10803-008-0667-2 Boucher, J., Bigham, S., Mayes, A., & Muskett, T. (2008). Recognition and language in low functioning autism. Journal of Autism and Developmental Disorders, 38(7), 1259–1269. https://doi.org/10.1007/s10803-007-0508-8 Charman, T., Pickles, A., Simonoff, E., Chandler, S., Loucas, T., & Baird, G. (2011). IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychological Medicine, 41(3), 619–627. https://doi.org/10. 1017/s0033291710000991 Dai, D. Y., & Sternberg, R. J. (2004). Motivation, emotion, and cognition: Integrative perspectives on intellectual functioning and development. Mahwah, NJ: Lawrence Erlbaum Associates. Dawson, M., Soulières, I., Gernsbacher, M. A., & Mottron, L. (2007). The level and nature of autistic intelligence. Psychological Science, 18(8), 657–662. https://doi.org/10.1111/j. 1467-9280.2007.01954.x Delobel-Ayoub, M., Ehlinger, V., Klapouszczak, D., Maffre, T., Raynaud, J. P., Delpierre, C., & Arnaud, C. (2015). Socioeconomic disparities and prevalence of autism spectrum disorders and intellectual disability. PLoS One, 10(11), e0141964. https://doi.org/10.1371/journal.pone.0141964 Doyen, C., Renou, S., Burnouf, I., Baron, T., Amado, I., Launay, C., & Kaye, K. (2020). La remédiation cognitive pour l’inclusion des enfants et des adolescents avec troubles du neurodéveloppement et/ou émotionnels. Neuropsychiatrie de l’Enfance et de l’Adolescence., 68, 196–201. Flanagan, H. E., Smith, I. M., Vaillancourt, T., Duku, E., Szatmari, P., Bryson, S., … Georgiades, S. (2015). Stability and change in the cognitive and adaptive behaviour scores of preschoolers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(9), 2691–2703. https://doi. org/10.1007/s10803-015-2433-6 Girardot, A. M., De Martino, S., Chatel, C., Da Fonseca, D., Rey, V., & Poinso, F. (2012). Cognitive profiles in pervasive developmental disorders. Encephale, 38(6), 488–495. https:// doi.org/10.1016/j.encep.2012.01.013 Habib, A., Harris, L., Pollick, F., & Melville, C. (2019). A metaanalysis of working memory in individuals with autism spectrum disorders. PLoS One, 14(4), e0216198. https://doi.org/ 10.1371/journal.pone.0216198 Hair, J. F., Black, W. C., Grimm, L. G., & Yarnold, P. R. (2000). Reading and understanding more multivariate statistics. Cluster Analysis (pp. 147–205). Washington, DC: American Psychological Association. Hedvall, Å., Fernell, E., Holm, A., Åsberg Johnels, J., Gillberg, C., & Billstedt, E. (2013). Autism, processing speed, INSAR and adaptive functioning in preschool children. ScientificWorldJournal, 2013, 158263–158267. https://doi.org/ 10.1155/2013/158263 Joseph, R. M., Steele, S. D., Meyer, E., & Tager-Flusberg, H. (2005). Self-ordered pointing in children with autism: Failure to use verbal mediation in the service of working memory? Neuropsychologia, 43(10), 1400–1411. https://doi.org/10. 1016/j.neuropsychologia.2005.01.010 Klin, A., Saulnier, C. A., Sparrow, S. S., Cicchetti, D. V., Volkmar, F. R., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal of Autism and Developmental Disorders, 37(4), 748–759. https://doi.org/10.1007/s10803-006-0229-4 Kraper, C. K., Kenworthy, L., Popal, H., Martin, A., & Wallace, G. L. (2017). The gap between adaptive behavior and intelligence in autism persists into young adulthood and is linked to psychiatric co-morbidities. Journal of Autism and Developmental Disorders, 47(10), 3007–3017. https://doi. org/10.1007/s10803-017-3213-2 Kuehnel, C. A., Castro, R., & Furey, W. M. (2019). A comparison of WISC-IV and WISC-V verbal comprehension index scores for children with autism spectrum disorder. The Clinical Neuropsychologist, 33(6), 1127–1137. https://doi.org/10.1080/ 13854046.2018.1503721 Lai, C. L. E., Lau, Z., Lui, S. S. Y., Lok, E., Tam, V., Chan, Q., … Cheung, E. F. C. (2017). Meta-analysis of neuropsychological measures of executive functioning in children and adolescents with high-functioning autism spectrum disorder. Autism Research, 10(5), 911–939. https://doi.org/10.1002/aur.1723 Le Couteur, A., Lord, C., & Rutter, M. (2003). The autism diagnostic interview-revised (ADI-R) (pp. 659–685). Los Angeles, CA: Western Psychological Services. Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule, (ADOS-2) modules 1–4. Los Angeles, CA: Western Psychological Services. Matson, J. L., & Shoemaker, M. (2009). Intellectual disability and its relationship to autism spectrum disorders. Research in Developmental Disabilities, 30(6), 1107–1114. https://doi. org/10.1016/j.ridd.2009.06.003 Matthews, N. L., Smith, C. J., Pollard, E., Ober-Reynolds, S., Kirwan, J., & Malligo, A. (2015). Adaptive functioning in autism spectrum disorder during the transition to adulthood. Journal of Autism and Developmental Disorders, 45(8), 2349–2360. https://doi.org/10.1007/s10803-015-2400-2 Mayes, S. D., & Calhoun, S. L. (2008). WISC-IV and WIAT-II profiles in children with high-functioning autism. Journal of Autism and Developmental Disorders, 38(3), 428–439. https://doi.org/10.1007/s10803-007-0410-4 McConnell, S. R. (2002). Interventions to facilitate social interaction for young children with autism: Review of available research and recommendations for educational intervention and future research. Journal of Autism and Developmental Disorders, 32(5), 351–372. https://doi.org/10.1023/a: 1020537805154 Milligan, G. W., & Cooper, M. C. (1985). An examination of procedures for determining the number of clusters in a data set. Psychometrika, 50(2), 159–179. Audras-Torrent et al./WISC-V in children with ASD without IDD 1005 Moorthy, R. S., Iyer, K., Krishnan, R. H., & Pugazhenthi, S. (2019). Enhancement of psychomotor skills in children with autism spectrum disorder by employing a mechatronic training kit. Paladyn, Journal of Behavioral Robotics, 10(1), 1–13. Mottron, L. (2004). Matching strategies in cognitive research with individuals with high-functioning autism: Current practices, instrument biases, and recommendations. Journal of Autism and Developmental Disorders, 34(1), 19–27. https:// doi.org/10.1023/b:jadd.0000018070.88380.83 Mottron, L. (2010). Que fait-on de l’intelligence autistique. Enfance, 1, 45–57. Nader, A. M., Courchesne, V., Dawson, M., & Soulières, I. (2016). Does WISC-IV underestimate the intelligence of autistic children? Journal of Autism and Developmental Disorders, 46(5), 1582–1589. https://doi.org/10.1007/s10803-014-2270-z Oliveras-Rentas, R. E., Kenworthy, L., Roberson, R. B., 3rd, Martin, A., & Wallace, G. L. (2012). WISC-IV profile in highfunctioning autism spectrum disorders: Impaired processing speed is associated with increased autism communication symptoms and decreased adaptive communication abilities. Journal of Autism and Developmental Disorders, 42(5), 655–664. https://doi.org/10.1007/s10803-011-1289-7 Piccolo, L. d. R., Arteche, A. X., Fonseca, R. P., GrassiOliveira, R., & Salles, J. F. (2016). Influence of family socioeconomic status on IQ, language, memory and executive functions of Brazilian children. Psicologia: Reflex~ ao e Crítica, 29. https://doi.org/10.1186/s41155-016-0016-x Samson, F., Mottron, L., Soulières, I., & Zeffiro, T. A. (2012). Enhanced visual functioning in autism: An ALE meta-analysis. Human Brain Mapping, 33(7), 1553–1581. https://doi. org/10.1002/hbm.21307 Scheuffgen, K., Happé, F., Anderson, M., & Frith, U. (2000). High "intelligence," low "IQ"? Speed of processing and measured IQ in children with autism. Development and Psychopathology, 12(1), 83–90. https://doi.org/10.1017/s095457940000105x Silleresi, S., Prévost, P., Zebib, R., Bonnet-Brilhault, F., Conte, D., & Tuller, L. (2020). Identifying language and cognitive profiles in children with ASD via a cluster analysis exploration: Implications for the new ICD-11. Autism Research, 13(7), 1155–1167. https://doi.org/10.1002/aur.2268 Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland adaptive behavior scales Vineland-II: Survey forms manual. Minneapolis, MN: Pearson. 1006 Terriot, K., & Ozenne, R. (2015). L’échelle d’intelligence de Wechsler pour enfants, 5 e édition (WISC-V). Approche Neuropsychologique des Apprentissages chez l’Enfant, 134, 95–102. Tillmann, J., San José Cáceres, A., Chatham, C. H., Crawley, D., Holt, R., Oakley, B., … Zwiers, M. P. (2019). Investigating the factors underlying adaptive functioning in autism in the EUAIMS Longitudinal European Autism Project. Autism Research, 12(4), 645–657. https://doi.org/10.1002/aur.2081 Wang, Y., Zhang, Y. B., Liu, L. L., Cui, J. F., Wang, J., Shum, D. H., et al. (2017). A meta-analysis of working memory impairments in autism spectrum disorders. Neuropsychology Review, 27(1), 46–61. https://doi.org/10.1007/ s11065-016-9336-y Ward, J. (1963). Hierarchical grouping to optimize an objective function. Journal of the American Statistical Association, 58, 236–244 Find this article online. Warren, Z., McPheeters, M. L., Sathe, N., Foss-Feig, J. H., Glasser, A., & Veenstra-Vanderweele, J. (2011). A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics, 127(5), e1303–e1311. https://doi.org/10. 1542/peds.2011-0426 Wechsler, D. (2014). WISC-V: Administration and scoring manual. Bloomington, MN: NCS Pearson, Incorporated. Weiss, L. G., Saklofske, D. H., Holdnack, J. A., & Prifitera, A. (2015). WISC-V assessment and interpretation: Scientistpractitioner perspectives. San Diego, CA: Academic Press. Yang, S., Paynter, J. M., & Gilmore, L. (2016). Vineland adaptive behavior scales: II profile of young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(1), 64–73. https://doi.org/10.1007/s10803-0152543-1 Supporting Information Additional supporting information may be found online in the Supporting Information section at the end of the article. Figure S1 Adaptive functioning and ASD severity scores for each cluster. Audras-Torrent et al./WISC-V in children with ASD without IDD INSAR