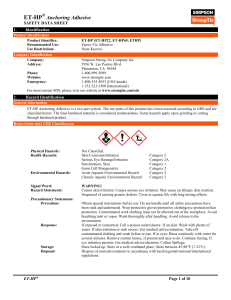
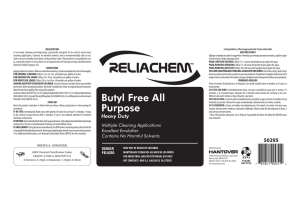
Logopedics Phoniatrics Vocology ISSN: 1401-5439 (Print) 1651-2022 (Online) Journal homepage: http://www.tandfonline.com/loi/ilog20 Childhood apraxia of speech: A survey of praxis and typical speech characteristics Ann Malmenholt, Anette Lohmander & Anita McAllister To cite this article: Ann Malmenholt, Anette Lohmander & Anita McAllister (2016): Childhood apraxia of speech: A survey of praxis and typical speech characteristics, Logopedics Phoniatrics Vocology, DOI: 10.1080/14015439.2016.1185147 To link to this article: http://dx.doi.org/10.1080/14015439.2016.1185147 Published online: 31 May 2016. Submit your article to this journal Article views: 22 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ilog20 Download by: [La Trobe University] Date: 21 June 2016, At: 04:01 LOGOPEDICS PHONIATRICS VOCOLOGY, 2016 http://dx.doi.org/10.1080/14015439.2016.1185147 ORIGINAL ARTICLE Childhood apraxia of speech: A survey of praxis and typical speech characteristics Ann Malmenholta,b , Anette Lohmandera,b and Anita McAllistera,b,c Downloaded by [La Trobe University] at 04:01 21 June 2016 a Division of Speech and Language Pathology, Department of Clinical Science, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden; bFunctional Area Speech & Language Pathology, Karolinska University Hospital, Stockholm, Sweden; cDivision of Speech and Language Pathology, Department of Clinical and Experimental Medicine, Link€oping University, Sweden ABSTRACT ARTICLE HISTORY Purpose: The purpose of this study was to investigate current knowledge of the diagnosis childhood apraxia of speech (CAS) in Sweden and compare speech characteristics and symptoms to those of earlier survey findings in mainly English-speakers. Method: In a web-based questionnaire 178 Swedish speech–language pathologists (SLPs) anonymously answered questions about their perception of typical speech characteristics for CAS. They graded own assessment skills and estimated clinical occurrence. Results: The seven top speech characteristics reported as typical for children with CAS were: inconsistent speech production (85%), sequencing difficulties (71%), oro-motor deficits (63%), vowel errors (62%), voicing errors (61%), consonant cluster deletions (54%), and prosodic disturbance (53%). Motorprogramming deficits described as lack of automatization of speech movements were perceived by 82%. All listed characteristics were consistent with the American Speech–Language–Hearing Association (ASHA) consensus-based features, Strand’s 10-point checklist, and the diagnostic model proposed by Ozanne. The mode for clinical occurrence was 5%. Number of suspected cases of CAS in the clinical caseload was approximately one new patient/year and SLP. Conclusions: The results support and add to findings from studies of CAS in English-speaking children with similar speech characteristics regarded as typical. Possibly, these findings could contribute to crosslinguistic consensus on CAS characteristics. Received 17 May 2015 Revised 10 March 2016 Accepted 21 April 2016 Published online 27 May 2016 Introduction Childhood apraxia of speech (CAS) is a speech sound disorder (SSD) negatively affecting children’s intelligibility. The disorder leads to a reduced ability to communicate, which in turn affects participation. Children displaying impaired intelligibility are assessed and diagnosed by speech–language pathologists (SLPs). To date there is no validated, replicable method for clinical diagnosis of CAS (1), resulting in uncertainty whether studies on CAS examine the correct population, displaying core difficulties of CAS or difficulties also seen in children with other SSDs. The reported prevalence rates vary between 0.125% and 4.3% (2–5), which may reflect the difficulties to define the diagnosis of CAS. The lowest estimates are based on clinical referral data (4), and the highest include children with suspected CAS (5). Several clinical studies have investigated key characteristics for CAS reported by SLPs based on English-speaking children (Table 1). Forrest asked SLPs attending a continuing education workshop to name up to three characteristics that they felt were necessary for a diagnosis of CAS. Altogether 50 different characteristics were listed. The analyses showed that the six most frequent criteria accounted for 51.5% of all KEYWORDS Assessment; clinical occurrence; consensus; global speech characteristics; inconsistent speech production; selfrating; speech–language pathologist; speech sound disorders responses; they were: inconsistent productions, general oromotor difficulties, groping, inability to imitate sounds, increased errors with increased length, and poor sequencing of sounds (6). In a follow-up survey gathered during conferences addressing the diagnosis and treatment of childhood apraxia of speech, SLPs listed the most essential characteristics used to diagnose CAS (7). The result showed no increased consensus among SLPs regarding key features of CAS. A new question added, compared to the Forrest survey, was if participating SLPs had read the American Speech–Language–Hearing Association (ASHA) position statement on CAS (8), and the outcome showed that 17% had done so. The answers from these did not differ from other SLPs concerning key features (7). Aiming for consensus among researchers and practicing SLPs, a literature review and a US national survey were conducted in order to define characteristics of CAS (9). This query resulted in five top characteristics that were agreed upon by at least 60% of researchers and SLPs showing ‘. . . a greater amount of agreement regarding CAS diagnostic criteria than commonly believed’. The top five were: inconsistent productions, difficulty with sound sequencing, groping or struggle behavior, articulation errors, and poor or reduced intelligibility. CONTACT Ann Malmenholt ann.malmenholt@ki.se Department of Clinical Science, Intervention and Technology, Division of Speech and Language Pathology, Karolinska Institutet, S–141 86 Stockholm, Sweden ß 2016 Informa UK Limited, trading as Taylor & Francis Group 2 A. MALMENHOLT ET AL. Table 1. Survey studies stating typical characteristics for CAS (in chronological order). References No of participants Participants Most prevalent characteristic 75 104 11 98 302 SLPs SLPs Researchers SLPs SLPs Inconsistent productions, 14.1% Difficulty planning speech, 78% Inconsistent production, 90% Inconsistent production, 55% Inconsistency of errors, 50% Forrest, 2003 (6) Millspaugh & Weiss, 2006 (9) Millspaugh & Weiss, 2006 (9) Joffe & Pring, 2008 (10) Meredith & Potter, 2011 (7) Table 2. Overview according to Ozanne’s diagnostic model (13). Cluster I Vowel errors Errors in phrases Cluster II DDK rate DDK sequence Errors in polysyllables Oro-motor Downloaded by [La Trobe University] at 04:01 21 June 2016 Errors not rules/processes Poor phonotactics Inconsistent articulation Distortion Cluster III Groping Consonant deletion Voluntary versus Involuntary Metathesis Cluster IV No babbling Prosodic disturbance The ‘Ozanne model’ contains three levels: phonological planning (cluster I), phonetic programming (clusters II–IV), and oro-motor control (clusters II–IV). To be diagnosed with CAS, children should display deficits on all three levels. Unsolicited information on CAS was received when asking SLPs about their clinical practice concerning children with phonological problems. Altogether 61% of responding SLPs reported uncertainty regarding differential diagnostic criteria for children with suspected CAS. The responses included inconsistent production, oro-motor problems, groping, sequencing problems, difficulty in copying sounds, distortions of vowels, and a history of feeding and drinking problems as potential markers for CAS. Slow progress or a resistance to therapy was mentioned to be behaviors not typically seen in children with phonological delay or disorder thus indicating CAS (10). In a Dutch study the six most pronounced CAS speech characteristics reported by SLPs were: difficulty sequencing articulatory movements, highly unintelligible speech, groping behavior, suprasegmental disturbances, inconsistent speech errors, and articulation errors (11), largely similar to the top six characteristic reported by Forrest (6) despite different languages. Mapping actual cases Guyette and Diedrich claimed that characteristics of CAS are commonly seen in all children displaying any speech disorder of unknown origin (12). Ozanne (13) studied 100 children with speech disorders of unknown origin benchmarking previously mentioned motor planning or programming problems (14–16). A cluster analysis of the 18 behaviors thought to reflect an underlying motorprogramming or motor-planning disorder showed that between 27% and 38% exhibited difficulties with diadochokinetic tasks, increased errors with increased load, and inconsistent productions, indicating that these characteristics are not specific for CAS alone. The diagnostic model suggested by Anne Ozanne (13) categorizes displayed speech errors to their presumed underlying deficits constructing a speech output planning and programming model for the diagnosis of CAS, as summarized in Table 2. Speech motor control in typical developing children was less mature in boys compared to girls up to the age of 5 years. The authors also observed a plateau in the development of co-ordination skills between the ages of 7 and 12 years, with consistency increasing also after 12 years of age, an important indication of the complexity of speech motor development (17). The influence of increased utterance length and complexity on speech motor performance in typically developing children (5-year-olds) and adults has been found to result in increased errors in both children and adults (18). Different frameworks to describe key features and etiology have been suggested (19). In response to the lack of consensus an Ad Hoc Committee on Childhood Apraxia of Speech was formed to review the research background for CAS in a technical report (20) and a supporting position statement (8). The ASHA report led to a proposition of a definition of CAS and consensus on three features observed in children with suspected CAS in the literature: ‘a) Inconsistent errors on consonants and vowels in repeated productions of syllables or words, b) lengthened and disrupted co-articulatory transitions between sounds and syllables, and c) inappropriate prosody, especially in the realization of lexical or phrasal stress.’ Another ASHA recommendation was henceforth to use the term CAS–childhood apraxia of speech exclusively, a term elsewhere referred to as speech delay–apraxia of speech (SD-AOS), developmental verbal dyspraxia (DVS), developmental apraxia of speech (DAS), and developmental verbal dyspraxia (DVD), to mention some. Recently a checklist for CAS has been developed by Edythe Strand and colleagues (21) and used as diagnostic tool in some studies (1,21). To meet criteria, participants should display evidence of four of the following 10 behaviors in three or more Madison Speech Assessment Protocol (MSAP) tasks: (1) difficulty achieving initial articulatory configurations or transitionary movement gestures; (2) syllable segregation; (3) equal stress or lexical stress errors; (4) vowel distortions and distorted substitutions; (5) groping; (6) intrusive schwa; (7) voicing errors; (8) slow rate; (9) slow diadochokinetic rates; and (10) increased difficulty with multisyllabic words. Murray and colleagues examined a sample of children with suspected CAS and asked two experts to rate presence and severity of CAS based on perceptual features of speech samples plus the three ASHA consensus-based features and Strand’s 10-point checklist (1). After using a discriminant function analysis, they concluded that ‘Polysyllabic production accuracy and an oral motor examination that includes diadochokinesis may be sufficient to reliably identify CAS and rule out structural abnormality or dysarthria’ (1, p. 43). For assessment of young or severely speech-impaired children with speech praxis difficulties, i.e. children not able to produce polysyllabics, Strand et al. constructed the valid and LOGOPEDICS PHONIATRICS VOCOLOGY reliable test DEMSS—The Dynamic Evaluation of Motor Speech Skill—further aiding the differential diagnosis of CAS (22). There is an ongoing effort to establish consensus on clinical diagnostic markers for CAS. Due to the historic lack of consensus the body of research on the disorder has been questioned since it may also include children with symptoms currently not included in the diagnosis. Expanded information on current clinical knowledge of SLPs assessing and treating children with CAS, speaking other languages than English, would be of great value in order to enhance current knowledge. Downloaded by [La Trobe University] at 04:01 21 June 2016 Aim The aim of this study was to investigate current knowledge about the diagnosis of CAS and compare speech characteristics and symptoms in Swedish to those of earlier survey findings in mainly English-speakers. The following research questions were posed: 1) How do Swedish SLPs rate their clinical knowledge assessing and diagnosing children with suspected CAS? 2) What speech characteristics and other deficits do SLPs consider typical in Swedish-speaking children with suspected CAS? 3) How frequent is suspected CAS in Swedish children seeing SLPs? What is the estimated clinical occurrence? 3 appropriate from a list of 17 speech characteristics (Question 14). These listed characteristics, often stated as typical for CAS in the literature, were chosen to avoid confusion due to variations in terminology. The respondents were divided into a less experienced (<10 years) and an experienced SLP group (>10 years). Differences between the two groups on the 17 speech characteristics were tested with chi-square. A P < 0.05 was regarded as significant. A subgroup of SLPs who reported having met with more than 100 cases of suspected CAS was put together and labeled as ‘experts’. The distribution of the answers on typical characteristics was ranked and categorized according to the cluster analysis presented by Ozanne (13). A total of 6 out of 17 characteristics (phonological deficits, language impairment, attention deficits, learning difficulties, poor gross-motor and poor finemotor skills) were listed to capture described co-occurring general features in the literature, e.g. academic difficulties (3) or generalized motor incoordination (24). Questions 16 and 17 asked for SLPs’ preconceived opinions and thoughts, in their own words, about observed cooccurring difficulties and important assessment considerations. The concluding summaries of these answers are more qualitative and processed using content analysis. The scale used in the question on how confident SLPs felt assessing children with CAS (Question 20) had six scale steps, ranging from very confident to very unsure. In the analyses the answers were dichotomized to either confident or unsure. Method A survey questionnaire was constructed, asking quantitative and qualitative questions about the population of children displaying the SSD of suspected CAS. The questionnaire was tested in a web-based pilot study. Four clinically and academically experienced SLPs participated. Comments from the pilot study concerned technical issues and choice of words, and resulted in the final version that consisted of 22 questions (see Appendix). Questions targeted the SLPs’ background (Questions 1 to 5), clinical accustomedness and theoretical knowledge regarding CAS (Questions 6–10 and 13–19), estimation of own competence regarding CAS (Questions 20–22), and questions regarding estimated occurrence of CAS in children at their own clinic (Questions 11 and 12). Six questions are not addressed in this paper, three questions due to their limited interest for the international reader (Questions 1, 3, and 5) and three (Questions 18, 19, and 21) because they survey intervention and will be reported elsewhere. We contacted SLP heads of departments throughout Sweden asking for email addresses of SLPs working with preand primary school-aged children. The web-based questionnaire was distributed to 289 Swedish SLPs during June–November 2011 using Google Docs Form to ensure that answers remained anonymous. The participants volunteered by completing the survey targeting SLPs’ professional know-how, not including any patient-specific data. Hence this study was regarded to be outside the scope of the ethical review board according to current guidelines. Respondents were asked to select as many characteristics as they felt Results A total of 178 clinical SLPs from 19 of Sweden’s 21 counties responded; this equals a survey response rate of 62%. The response rate between different questions in the survey varied with a mean response rate of 90% (Table 3). SLP experience and knowledge on assessment and diagnosis Respondents were from different clinical settings and had a range of clinical experience. Participating SLPs had graduated from different universities between the years 1972 and 2011 Table 3. Response rate in percent specified for each included survey question (see Appendix). Question Response rate (%) 2 4 6 7 8 9 10 11 12 13 14 15 16 17 20 22 96 97 94 98 97 98 96 89 82 96 96 96 38 74 97 97 Downloaded by [La Trobe University] at 04:01 21 June 2016 4 A. MALMENHOLT ET AL. Figure 1. Different assessment approaches for CAS reported by Swedish SLPs. (Question 2). Forty-one percent of respondents were in their first five years of practice, 22% had from five to ten years of experience, and 37% more than ten years of clinical experience primarily working with preschool and primary school children (Question 9). Forty-four percent of the SLPs worked in hospitals or public speech and language clinics, 12% at university hospitals, 24% within child habilitation services, 9% in special pre- and primary schools for children with speech and language disorders, 8% at private clinics, and 3% in other work places (Question 4). Figure 1 summarizes the main assessment approaches which emerged when analyzing respondents’ answers on what they considered important when assessing children with suspected CAS (Question 17). In Question 10, SLPs, diagnosing children with suspected CAS, were asked to choose one or several codes from a selected list of the International Classification of Diseases (ICD-10) stating their typical use for patients with CAS. The most frequently used diagnoses were oral and/or verbal apraxia (R48.2) occurring in 44%, phonological disorder (F80.0A) in 22%, a combination of phonological disorder and oral motor developmental delay (F80.0A þ F80.0B) in 23%, and other ICD-10 codes in 11% of answers. SLPs were also asked to report the sources of their theoretical and clinical knowledge regarding CAS. Possible alternatives were lectures during undergraduate studies (Question 6), lectures or courses after undergraduate studies (Question 7), or search for information about CAS by themselves (Question 8). Courses included in undergraduate studies had been undertaken by 68%, later courses or lectures by 54%, and search for information on their own using different sources (e.g. browsing the internet, reading studies obtained via PubMed, asking colleagues specialized in speech motor disorders) was reported by 83%. Three SLPs answered ‘no’ to all three questions about knowledge base regarding CAS. One diagnosed children with suspected CAS. Twenty-nine percent of the SLPs perceived CAS to be a disorder in its own right, 10% considered the disorder to be part of or in co-morbidity with another disorder, 51% of the SLPs experienced that some cases are clear cases of CAS and some are part of or in co-morbidity with other disorders. The alternative: ‘CAS is a consequence of another disorder’ was not agreed upon by any SLP, but 10% replied that they did not know (Question 13). When asked to share observations of co-occurring difficulties seen in children with suspected CAS (Question 16) respondents raised different issues using the free text answering space. Most answers were clarifications and comments on issues covered in general, often using a different terminology, compared to the listed typical characteristics (Question 17) and statements about typical behaviors (Question 15). The notion of variability in the ability to produce speech during different days was added. Some SLPs observed additional co-ordination difficulties not only obstructing smoothness of articulators and body movements but also affecting the control of air flow, resulting in voice initiation and voice quality issues. When rating their own ability as SLPs to assess children with suspected CAS 55% of respondents felt unsure and 45% confident about diagnosing CAS (Question 20). A further analysis of these figures was conducted based on the fact that only half of the SLPs reported that they do assess and diagnose CAS (Question 10). The analyses revealed that out of the SLPs not assigned to diagnose children with suspected CAS, 29% felt confident about performing CAS assessment, and 71% did not. Among the SLPs that assessed and LOGOPEDICS PHONIATRICS VOCOLOGY 5 Downloaded by [La Trobe University] at 04:01 21 June 2016 Table 4. Typical characteristics of CAS in rank order from a SLP survey and a subgroup of experts (>100 CAS cases), fitted into the ASHA consensus-based features (8), Strand’s 10-point checklist (21), and categorized according to the cluster analysis proposed by Ozanne (13). Typical characteristics in CAS Frequency of selection of characteristics (n ¼ 171) Frequency of selection of characteristics by a subgroup of experts on CAS (n ¼ 6) Inconsistent production Motor-programming deficits Sequencing difficulties Oro-motor deficits Vowel errors Voicing errors Consonant cluster deletion Prosodic disturbance Phonological deficits Resonance inconsistency Poor fine-motor skills Metathesis Suprasegmental disturbance Poor gross-motor skills Language impairment Learning difficulties Attention deficits 85% 82% 71% 63% 62% 61% 54% 53% 44% 36% 34% 23% 19% 12% 10% 5% 4% 67% 100% 67% 83% 50% 67% 67% 50% 2% 33% 0% 2% 0% 0% 0% 0% 0% ASHA consensus-based features (2007) Strand’s 10-point checklist (2011) a c b b c b b c 1 8 1 4 7 4 3 Clusters according to Ozanne’s model (presented in 1995) I III II II I II III IV II c 2 III IV Key: a ¼ Inconsistent errors on consonants and vowels in repeated productions of syllables or words; b ¼ lengthened and disrupted co-articulatory transitions between sounds and syllables; c ¼ inappropriate prosody, especially in the realization of lexical or phrasal stress; 1 ¼ difficulty achieving initial articulatory configurations or transitionary movement gestures; 2 ¼ syllable segregation; 3 ¼ equal stress or lexical stress errors; 4 ¼ vowel distortions and distorted substitutions; 5 ¼ groping; 6 ¼ intrusive schwa; 7 ¼ voicing errors; 8 ¼ slow rate; 9 ¼ slow diadochokinetic rate; 10 ¼ increased difficulty with multisyllabic words; I–IV, see Table 2. Figure 2. The 17 speech characteristics typical for CAS clustered using Ozanne’s model and co-occurring characteristics. diagnosed CAS 59% reported that they felt confident and 41% that they felt unsure. Eighty-nine percent of all responding SLPs declared a lack of competence regarding CAS (Question 22). The question regarding additional training, ‘What kind of supplementary training would meet your needs?’, was answered in free text, describing different areas of interest. One-quarter (25%) stated a need for an update on current literature and research, another quarter (23%) knowledge about intervention. Knowledge about evidencebased practice was called for by 5% and about diagnosis/differential diagnosis by 15%. Five percent of responding SLPs reported an interest for CAS in a broader context or regarding co-morbidity. Settings for education and training were suggested: coaching by experienced colleagues (11%) and through workshops or case discussions or video examples by 14% of the responding SLPs. Three SLPs were interested in consensus discussions with Swedish examples. Speech characteristics and other deficits seen in CAS The 171 respondents selected between 2 and 17 characteristics from the list of 17 characteristics (Question 14). A total of 1043 characteristics were selected by the respondents; the mode value was 7.2. The characteristics were fitted into the consensus-based features from ASHA’s technical report (20), Strand’s 10-point checklist (21), and clustered according to Ozanne’s model (13) showing overlap on eight characteristics, as seen in Table 4. Dividing respondents into less experienced (n ¼ 109) and more experienced (n ¼ 64) SLPs, based on years of practice, showed that the less experienced SLPs significantly more often registered vowel errors as a typical speech characteristic for CAS. Answers for other typical characteristics were not significantly different between groups. The expert group (n ¼ 6), consisting of SLPs seeing more than 100 cases of Downloaded by [La Trobe University] at 04:01 21 June 2016 6 A. MALMENHOLT ET AL. suspected CAS, showed a slightly different pattern, even more in line with characteristics from the ASHA consensus-based features, Strand’s 10-point checklist, and Ozanne’s model. Clustering all survey answers on typical speech characteristics revealed that 81% of SLPs listed characteristics from all three clusters (I–III), sufficient for the three levels in the diagnostic model (Figure 2); a similar distribution was found for clusters I, II, and III, whereas characteristics in cluster IV were chosen somewhat less frequently. The remaining six characteristics not included in any of the used models were grouped in four areas of difficulties, showing that almost half of the answering SLPs perceived that CAS patients display language impairment as well. Motor difficulties, i.e. poor fineand gross-motor skills, were noted to be a typical characteristic by one-third of the SLPs. Learning difficulties and attention deficits were not reported to be typically co-occurring. Statements about typical behaviors seen in children with CAS had to be agreed with by the respondents (Question 15). In total 92% shared the opinion that ‘children with CAS make very slow progress (in therapy)’, and 58% felt that ‘patients (with CAS) were resistant to therapy’. ‘Regressing after a treatment break’ was an experience shared by 58%, and ‘persistent speech difficulties at school age’ was noted by 84% of the SLPs. ‘Difficulties with reading development’ was observed by 24% and ‘difficulties with writing development’ by 23% of the SLPs. Estimation of clinical occurrence of CAS The mode value for rated clinical occurrence, consisting of an estimation of the number of patients showing difficulties with verbal praxis in percent, was 5% over all clinical settings in this study (Question 12). Answers ranged from 0% to 70%. The mode value for clinical occurrence estimated by SLPs working at habilitation centers was twice as high (11%), including one estimation of 70%. About half of the SLPs (52%) reported seeing between 0 and 1 new patient with suspected CAS per year in their clinic, and answers ranged from 0–20 patients/year (Question 11), including those specialized in motor speech disorders. Discussion In this study comprehensive information about clinical SLPs’ knowledge concerning children with suspected CAS was collected. The overall aim was to investigate current knowledge about the diagnosis of childhood apraxia of speech (CAS) by letting Swedish SLPs share their clinical experience and observations of typical speech characteristics and other symptoms in these children. They were also asked to estimate clinical occurrence, e.g. the number of patients in their clinical population. In addition, we wanted to compare speech characteristics and symptoms to those of earlier survey findings in mainly English-speakers. The survey response rate and distribution of SLPs throughout the country and in different work settings make it likely that the responding SLPs, despite the lack of responses from two counties, together represent the current praxis, knowledge, and clinical competence in Sweden. SLPs’ experience and knowledge on assessment and diagnosis Assessment approaches differed, reflecting the absence of consensus on a specific assessment approach for CAS in Sweden. At present SLPs administer their own test batteries reflecting their view of CAS as a disorder of primarily phonologic/linguistic and/or motor difficulty. A disparity was also seen in the reported ICD-10 diagnoses. Differences in SLP education in the field of motor speech disorders and, in particular, regarding CAS during the past decades could also explain this disparity. A theory-based test battery for children in Swedish, as in other countries and languages, with the purpose to differentiate between speech sound disorders is needed. In this survey no question mentions severity of CAS manifestations or age of the children affected. In children with milder symptoms, where suspected CAS is to be differentiated from phonological delay and/or oro-motor difficulties, some children might have been diagnosed with a combination of diagnoses, in this survey used by 23% of SLPs. The use of other diagnoses might reflect an insecurity concerning the diagnosis of CAS and neurological disorders in children. Answers from experts (n ¼ 6) indicate that SLPs with experience of more than 100 cases of suspected CAS have enhanced diagnostic skills regarding differentiating phonological and speech disorders from oral motor and speech motor disorders. The age of the child is another factor influencing and changing the manifestations of CAS in different children and over time in the same child (25). Actively searching for information and knowledge on their own was reported by 83% of SLPs. Due to the uncertainty of the disorder and new developments in the field this must be seen as a highly adequate method to update theoretical knowledge and clinical competence. About one-third of SLPs in this survey viewed CAS as a defined, exclusive disorder, but 10% had not experienced clear-cut cases of CAS. About half of the SLPs reported that they had experienced clear-cut cases of CAS but also children displaying CAS symptoms as a part of or in co-morbidity with other disorders. This diversity of clinical experience and viewpoints on CAS reflects the multi-faceted character of the disorder and the influence of different work settings and clinical populations. Speech characteristics and other deficits seen in CAS The ranking of typical speech characteristics in CAS corresponded largely with other surveys of English-speaking SLPs (6,7,9,10). Forrest (6) concluded that her study on diagnostic criteria was limited due to predetermined instructions (i.e. provide up to three criteria for diagnosing CAS). In the present study the limitation was in the list of predetermined, typical characteristics for CAS (i.e. the SLPs could not use their own words, and the terms provided were not additionally defined), yet the mode for the number of chosen characteristics was over seven, close to the number repeatedly stated in other surveys. More than 50% of the SLPs in the present study listed as many as seven characteristics, with inconsistent production being the most common (85%), also Downloaded by [La Trobe University] at 04:01 21 June 2016 LOGOPEDICS PHONIATRICS VOCOLOGY mentioned as the most prevalent characteristic in several other studies (6,7,9,10). Motor-programming deficits (82%) described as lack of automatization of speech motor movements (i.e. a global term including groping and voluntary versus involuntary speech movements) (14,16) is a feature difficult to capture in one term but is probably also reflected in sequencing difficulties (71%) (11,14). Oro-motor deficits were marked by 63% of the SLPs, also supported by several studies (14–16). Vowel errors (62%) (14,16), voicing errors (61%) (26), consonant cluster deletion (54%) (14,26), and prosodic disturbance (53%) (14,16) are all difficulties alerting SLPs. When comparing our findings with the three consensus features from the ASHA position statement (8), Strand’s checklist (21), and the ‘Ozanne model’ (13) they correspond to a great extent for all surveyed SLPs. Furthermore, the characteristics identified by the expert group were even more in line with current models and checklists, apart from the features of prosodic and suprasegmental disturbance. A possible explanation for this could be that experts see more children with severe difficulties, hence less speech output, which is required for assessment of prosodic difficulties. Our findings in Swedish-speaking children are in line with findings across studies from English-speaking countries (6,7,9,10) and a report from Dutch (11) and Danish children (27), suggesting shared characteristics of children with CAS across these Germanic languages. It would be interesting to study how stable these characteristics are across languages. We found one significant difference between experienced and less experienced SLPs: the less experienced SLPs registered vowel errors as a typical speech characteristic for CAS more often. Since experience is related to years post exam in the present study, it is reasonable to interpret this as more updated knowledge on key speech characteristics. One-quarter of responding SLPs perceived patients with CAS as having difficulties in reading and writing development, but just 5% estimated that CAS patients had learning difficulties. Other deficits in language, reading, and writing skills at school age are reported in children with CAS, despite the articulation difficulties being partially resolved (28). Probably a broader view on CAS with a multiple domain framework can explain the numerous and varying core features of CAS displayed as auditory-perception encoding and memory and transcoding deficits (23). Future research in CAS would benefit from more detailed descriptions of the subjects’ core and co-occurring difficulties. Furthermore, many SLPs (81%) displayed knowledge of current theoretical frameworks and awareness of typical speech characteristics in CAS. This is a positive finding, considering the impact a correct diagnosis may have on individualized intervention plans and accuracy of prognosis. In the body of CAS literature much effort is spent on finding diagnostic markers in order to specify the diagnosis of CAS and distinguishing it from other subsets of speech sound disorders (4,23,29). There is a need for evidence-based assessment of children with CAS and for consensus on overt speech characteristics and their presumed underlying deficits. However, a cluster of diagnostic markers might be clinically appropriate in order to differentiate these children from children with other speech sound disorders (1,13,22,23). 7 Survey reports on SLPs’ knowledge about CAS characteristics show similar presentations across studies. This could reflect a growing knowledge on speech characteristics in CAS. If international consensus on the characteristics of children with CAS is emerging, and CAS characteristics are shared between languages, this would have major implications on future, shared diagnostic methods, facilitating research collaborations and studies including larger, international samples. Estimation of clinical occurrence of CAS The estimated clinical occurrence with a mode value of 5% reflects different work settings, given that the highest, outlying, estimate (70%) came from a clinician working at child habilitation services. Other high estimates (25%–50%) were made by seven colleagues from different work settings, in different parts of the country, and with varying years of experience. Two of these SLPs still rated their ability to diagnose CAS as unsure. The other six felt more certain about their own ability to diagnose CAS. One SLP reported seeing ‘some signs of dyspraxic involvement in about 50%’. This reflects that some SLPs have specialized in motor speech disorders, hence mostly seeing patients with CAS or dysarthria, leading to these high numbers in their caseloads. Asking informally for information on clinical occurrence is not comparable to calculations of prevalence and incidence but may give an indication of the occurrence of CAS in pre- and primary school children seen in Swedish SLP clinics. The quest in this study was to describe SLPs’ clinical reality, and the diversity of answers highlights the need for formal calculations. Even the variance of reported prevalences in the literature, from 0.125% to 4.3% (2–5) raises questions about descriptions and inclusion criteria in research studies, possibly also reflecting lack of agreement on diagnostic criteria over time. The somewhat higher occurrence of CAS reported by Swedish SLPs could mirror the large number of vowels in Swedish, distinguished by subtle articulatory and durational properties (30). This may also indicate a need for more in-depth training regarding judgement of vowel quality and prosodic features. The overall low occurrence reminds us that CAS occupies a small portion of SLP caseloads. This in turn may lead to a lack of knowledge, experience, and confidence within the profession and a need for continued education considering research results in the field. This could be resolved by specialization of SLPs with a recognized competence in motor speech disorders, a suggestion already made in ASHA’s position statement (8). Methodological concerns The 17 typical speech characteristics listed were presented without definitions. This makes it precarious to control the respondents’ understanding of the listed characteristics in detail. However, we presuppose that all SLPs have specific knowledge about speech characteristics, and judging by the answers most SLPs seemed to have knowledge about the included speech characteristics. Our aim was to explore Downloaded by [La Trobe University] at 04:01 21 June 2016 8 A. MALMENHOLT ET AL. present knowledge of a sample of SLPs. The respondents had graduated during a time span of 39 years, yet significant discrepancies were found only regarding one CAS speech characteristic, namely vowel errors. During the construction of this survey no weighting of speech characteristics was performed. However, in the analysis the 17 characteristics were distributed into Ozanne’s model consisting of four clusters which resulted in similar frequencies (90%–96%) for clusters I, II, and III. Cluster IV showed a somewhat lower frequency (72%), probably because cluster IV consists of only two characteristics, one being deviant prosody and the other an anamnestic feature regarding no history of babbling, not included in the present survey. Prosodic errors, reflected in vowels and sonorants, are difficult to assess especially in children with multiple speech disorders and limited speech production, which often is the case in children with more severe CAS (31). The survey question with the lowest response rate (Question 16) was about observations made on co-occurring difficulties in children with CAS. However, few new topics were raised when the SLPs were given the opportunity to answer in their own words. This might reflect the broadness of the survey, or it could be due to the fact that respondents were focused on deficits concerning speech characteristics and not more general characteristics. SLPs may not routinely ask for co-occurring difficulties. A drawback to distributing the survey anonymously was that it ruled out the possibility of sending out a reminder. On the other hand, we presume that answers are sincere. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Conclusions The results support and add to findings from studies of CAS in English-speaking children with similar speech characteristics regarded as typical. Possibly, these findings could contribute to cross-linguistic consensus on CAS characteristics. Also this study reveals that 98% of SLPs reported having some theoretical and clinical knowledge about the disorder, although the majority (89%) reported a need for further education about CAS. Future studies on CAS, including other languages, are needed to investigate possible global speech characteristics. 14. 15. 16. 17. 18. 19. Acknowledgements We are grateful to all colleagues answering the survey and sharing their clinical experience. 20. 21. Disclosure statement The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper. 22. ORCID 23. Ann Malmenholt http://orcid.org/0000-0002-3615-4891 Anette Lohmander http://orcid.org/0000-0003-0951-4908 Anita McAllister http://orcid.org/0000-0003-2208-0630 24. Murray E, McCabe P, Heard R, Ballard KJ. Differential diagnosis of children with suspected childhood apraxia of speech. J Speech Lang Hear Res. 2015; 58: 43–60. Morley ME. The development and disorders of speech in childhood. 3rd ed. London: Livingstone; 1972. Shriberg LD, Kwiatkowski J. Developmental phonological disorders. I: A clinical profile. J Speech Hear Res. 1994; 37: 1100–26. Shriberg LD, Aram DM, Kwiatkowski J. Developmental apraxia of speech: I. Descriptive and theoretical perspectives. J Speech Lang Hear Res. 1997; 40: 273–85. Delaney AL, Kent RD. Developmental profiles of children diagnosed with apraxia of speech. Poster session presented at the annual convention of the American Speech-Language-Hearing Association; 2004 Nov 18–20; Philadelphia, USA. Forrest K. Diagnostic criteria of developmental apraxia of speech used by clinical speech-language pathologists. Am J Speech Lang Pathol. 2003; 12: 376–80. Meredith A, Potter N. Diagnostic criteria for childhood apraxia of speech: a survey study. ASHA Convention; 2011. Handouts. American Speech-Language-Hearing Association. Childhood apraxia of speech: position statement. 2007. Available at: www. asha.org. Millspaugh S, Weiss D. Diagnosing childhood apraxia of speech: a national survey of speech-language pathologists. ASHA Convention; 2006. Handouts. Joffe V, Pring T. Children with phonological problems: a survey of clinical practice. Int J Lang Commun Disord. 2008; 43: 154–64. Nijland L. Speech perception in children with speech output disorders. Clin Linguist Phon. 2009; 23: 222–39. Guyette T, Diedrich W. A critical review of developmental apraxia of speech. In: Lass N, editor. Speech and language: advances in basic research and practice. New York: Academic Press; 1981. p. 1–49. Ozanne A. Childhood apraxia of speech. In: Dodd B, editor. Differential diagnosis and treatment of children with speech disorder. 2nd ed. London: Whurr Publishers; 2005. p. 71–82. Rosenbek J, Wertz R. A review of 50 cases of developmental apraxia of speech. Lang Speech Hear Serv Sch. 1972; 3: 23–33. Adams C. Syntactic comprehension in children with expressive language impairment. Br J Disord Commun. 1990; 25: 149–71. Pollack K, Hall P. An analysis of vowel misarticulations of five children with developmental apraxia of speech. Clin Linguist Phon. 1991; 5: 207–24. Smith A, Zelaznik HN. Development of functional synergies for speech motor coordination in childhood and adolescence. Dev Psychobiol. 2004; 45: 22–33. Maner KJ, Smith A, Grayson L. Influences of utterance length and complexity on speech motor performance in children and adults. J Speech Lang Hear Res. 2000; 43: 560–73. Waring R, Knight R. How should children with speech sound disorders be classified? A review and critical evaluation of current classification systems. Int J Lang Commun Disord. 2013; 48: 25–40. American Speech-Language-Hearing Association. Childhood apraxia of speech: Technical report Ad Hoc Committee on Apraxia of Speech in Children. Rockville Pike, MD: ASHA; 2007. Shriberg LD, Potter NL, Strand EA. Childhood apraxia of speech in children and adolescents with galactosemia. J Speech Lang Hear Res. 2011; 54: 487–519. Strand EA, McCauley RJ, Weigand SD, Stoeckel RE, Baas BS. A motor speech assessment for children with severe speech disorders: reliability and validity evidence. J Speech Lang Hear Res. 2013; 56: 505–20. Shriberg LD, Lohmeier HL, Strand EA, Jakielski KJ. Encoding, memory, and transcoding deficits in childhood apraxia of speech. Clin Linguist Phon. 2012; 26: 445–82. Crary, MA. Developmental motor speech disorders. San Diego, CA: Singular Publishing Group, Inc.; 1993. LOGOPEDICS PHONIATRICS VOCOLOGY 25. 26. 27. 28. Stackhouse J. Developmental verbal dyspraxia. I: A review and critique. Eur J Disord Commun. 1992; 27: 19–34. Yoss KA, Darley FL. Developmental apraxia of speech in children with defective articulation. J Speech Hear Res. 1974; 17: 399–416. Skov L. Danske børn med verbal dyspraksi – hvor har de deres vanskeligheder? Master thesis in Audiologopædi, University of Southern Denmark, Odense; 2008. Lewis BA, Freebairn LA, Hansen AJ, Iyengar SK, Taylor HG. School-age follow-up of children with childhood apraxia of speech. Lang Speech Hear Serv Sch. 2004; 35: 122–40. 29. 30. 31. 9 Shriberg LD, Green JR, Campbell TF, McSweeny JL, Scheer AR. A diagnostic marker for childhood apraxia of speech: the coefficient of variation ratio. Clin Linguist Phon. 2003; 17: 575–95. McAllister R. Talkommunikation [Speech communication]. 2nd ed. Lund: Studentlitteratur; 1998. p. 45–59. T€ ukel S, Bj€ orelius H, Henningsson G, McAllister A, Eliasson AC. Motor functions and adaptive behaviour in children with childhood apraxia of speech. Int J Speech Lang Pathol. 2015; 17: 470–80. Appendix Downloaded by [La Trobe University] at 04:01 21 June 2016 Survey questions Questions in bold are addressed in the present article. 1 2 Where did you study to become a speech–language pathologist? Which year did you graduate? 3 Which county are you working in? 4 5 What type of setting are you working in? Hospital; university hospital; public speech and language clinic; private clinic; child habilitation services; special pre- and primary school for children with speech and language disorders; other working places How many SLP colleagues seeing pre- and primary school patients do you have at your setting? 6 Was there a lecture about CAS during your undergraduate studies? 7 Have you participated in lectures or courses after your undergraduate studies? 8 Have you searched for information about CAS on your own? 9 For how long have you been working with pre- or primary school-aged children? <5 years; 5–10 years; 11–15 years; 16–20 years; >20 years 10 Do you assess and diagnose children with CAS? yes/no If you do, what ICD code do you use? (Choose one or multiple answers) F80.0A; F80.0A þ F80.0B; R48.2; R48.2A; R48.2B; other 11 Approximately how many children displaying CAS have you met? (Space for free answer) 12 Approximately what percentage of patients on your caseload do you consider to have difficulties with verbal praxis? (Space for free answer) 13 I consider CAS to be: (Choose one or multiple answers) a diagnosis in its own right, not necessarily coexisting with other disorders part of or in co-morbidity with other disorders such as SLI, ADHD, ADD, dyslexia, cerebral palsy, Down syndrome, Rett syndrome, or other disorders a consequence of other disorders I do not know 14 Typical symptoms for children displaying CAS are: (Choose one or multiple answers) Inconsistent production; motor-programming deficits; sequencing difficulties; oro-motor deficits; vowel errors; voicing errors; consonant cluster deletion; prosodic disturbance; phonological deficits; resonance inconsistency; poor fine-motor skills; metathesis; suprasegmental disturbance; poor gross-motor skills; language impairment; learning difficulties; attention deficits 15 Children with CAS: (Choose one or multiple answers) Make very slow progress; make expected progress; are during periods almost resistant to therapy; regress after treatment break; have persistent speech difficulties at school age; have difficulties with reading development; have difficulties with writing development 16 Co-occurring difficulties you have observed in children with CAS? (Space for free answer) 17 If a child is suspected of having CAS, what do you consider to be important during assessment? (Space for free answer) 18 What do you consider to be most important when treating children with CAS? 19 If you have any experience treating children with CAS, please share examples of successful intervention. 20 How secure do you feel assessing children with CAS? Very confident; confident; fairly confident; fairly unsure; unsure; very unsure 21 How secure do you feel when treating children with CAS? 22 Do you consider yourself lacking competence concerning CAS? yes/no If yes: What kind of supplementary training would meet your needs? Questions 1, 3, 5, 18, 19, and 21 are not addressed in the present article.