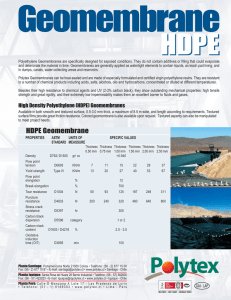
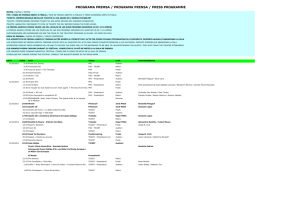
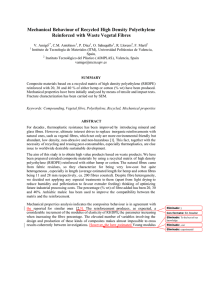
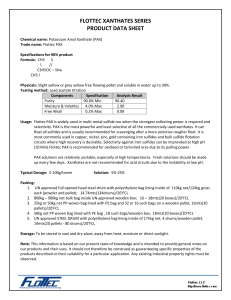
SCIENTIFIC ARTICLE Wear Particles and Osteolysis in Patients With Total Wrist Arthroplasty Michel E. H. Boeckstyns, MD, Anders Toxvaerd, MD, Manjula Bansal, MD, Lars Soelberg Vadstrup, MD Purpose To determine whether the amount of polyethylene debris in the interphase tissue between prosthesis and bone in patients with total wrist arthroplasty correlated with the degree of periprosthetic osteolysis (PPO); and to investigate the occurrence of metal particles in the periprosthetic tissue, the level of chrome and cobalt ions in the blood, and the possible role of infectious or rheumatoid activity in the development of PPO. Methods Biopsies were taken from the implantebone interphase in 13 consecutive patients with total wrist arthroplasty and with at least 3 years’ follow-up. Serial annual radiographs were performed prospectively for the evaluation of PPO. We collected blood samples for white blood cell count, C-reactive protein, and metallic ion level. Results A radiolucent zone of greater than 2 mm was observed juxta-articular to the radial component in 4 patients and at the carpal component in 3. The magnitude of the radiolucent zone tended to level out over time. We observed subsidence of the implant in 3 patients on the carpal side and in none on the radial side. The amount of polyethylene and metallic debris was generally small and did not correlate with the width of the radiolucent zone. The blood levels of chrome and cobalt ions were normal. There was no evidence of infectious or rheumatoid activity. Conclusions Polyethylene wear has been accepted as a major cause of osteolysis in total hip arthroplasty, and metallic debris has also been cited to be an underlying cause. However, our hypothesis that polyethylene debris correlated with the degree of PPO could not be confirmed. Also, metallic debris and infectious or rheumatoid activity did not correlate with PPO. (J Hand Surg Am. 2014;39(12):2396e2404. Copyright Ó 2014 by the American Society for Surgery of the Hand. All rights reserved.) Type of study/level of evidence Prognostic I. Key words Wrist arthroplasty, osteolysis, histopathology, interphase. P ERIPROSTHETIC OSTEOLYSIS (PPO) is a biological process of bone resorption seen as radiolucent lines or areas on radiographs. Polyethylene wear has been accepted as a major cause of osteolysis in total hip arthroplasty. Particles, which occur because of abrasive wear, are considered to stimulate a foreign body response resulting in bone loss mainly mediated by macrophages that lead through complex cellular interactions to the recruitment and activation of osteoclasts.1e3 Metallic debris has also been cited as an underlying cause, and abnormal chrome (Cr) and cobalt (Co) levels in blood can be found in patients with metalon-metal total hip arthroplasty.4e7 Osteolysis may be silent, and loosening of the implants may be incomplete From the Clinic of Hand Surgery, Gentofte Hospital, and the Department of Pathology, Herlev Hospital, University of Copenhagen, Denmark; and the Department of Pathology, Hospital for Special Surgery, New York, NY. Corresponding author: Michel E. H. Boeckstyns, MD, Clinic of Hand Surgery, Gentofte Hospital, University of Copenhagen, Niels Andersens Vej 65, 2900 Hellerup, Denmark; e-mail: mibo@dadlnet.dk. Received for publication May 14, 2014; accepted in revised form July 23, 2014. 0363-5023/14/3912-0007$36.00/0 http://dx.doi.org/10.1016/j.jhsa.2014.07.046 M.E.H.B. received support from Gentofte Hospital, Clinic for Hand Surgery. No benefits in any form have been received or will be received related directly or indirectly to the subject of this article. 2396 r Ó 2014 ASSH r Published by Elsevier, Inc. All rights reserved. 2397 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY with the implant remaining steadily anchored in the bone.3 Periprosthetic osteolysis with or without complete loosening occurs in other joints as well and has been frequently reported after total wrist arthroplasty (TWA).8e13 Since 2003, we have been using the Re-motion TWA (SBI, Inc, Morrisville, PA) as an alternative to total wrist arthrodesis for the reconstruction of severely destroyed and painful wrists. This implant contains an articular component made of conventional polyethylene that articulates with a metallic CreCo component. Our hypothesis was that the occurrence of polyethylene debris in the interphase tissue between prosthesis or cement and bone was correlated with the degree of PPO. A secondary aim of the study was to investigate the occurrence of metal particles in the periprosthetic tissue, the level of Cr and Co ions in the blood of patients, and the possible role of infectious or rheumatoid activity in the development of PPO. MATERIALS AND METHODS Ethics The study conformed to the ethical guidelines of the 1975 Helsinki Declaration. The Scientific Ethical Committee for the Capital Region in Denmark approved the study (Study H-2-2013-032). We obtained written informed consent from all patients. Selection of patients Re-motion TWA is an elliptical ball and socket design consisting of radial and carpal CreCo components that are titanium coated and an intercalated polyethylene ball. It mainly articulates with the radial component in an unconstrained link but also permits a rotational articulation of 20 with the carpal plate. It requires minimal bone resection and is designed to act much like a surface replacement. The carpal plate is fixated to the carpus by its stem and 2 screws. The polyethylene in the carpal ball is of a conventional, not highly cross-linked type. All patients in whom a Re-motion TWA was implanted at Gentofte Hospital, Denmark, between September 2003 and April 2010 (21 patients) were eligible for this study. We excluded wrists that had been revised to a new TWA or arthrodesis (3 patients), those who were unable to participate for geographical reasons (2 patients), those who had not given informed consent (1 patient), those with conditions that contraindicated the surgical procedure (one patient: recent ipsilateral J Hand Surg Am. r TABLE 1. Included Demographics of the 13 Patients Age, y (mean [range]) Sex Mean follow-up, y (mean [range]) 68 (53e87) 2 male, 11 female 6 (3e10) Diagnosis Rheumatoid arthritis 6 Idiopathic osteoarthritis 4 Posttraumatic arthritis 3 Fixation technique 2 cemented, 11 not cemented* *Cemented fixation was used when the bone was considered too fragile to support uncemented implant components. shoulder fracture), and those who were already included with the contralateral wrist (one patient). Thus, 13 patients were included. Table 1 shows the demographics. We obtained tissue samples from the implantebone or implantecementebone interphase, collected blood samples, obtained plain x-ray examinations, and updated the clinical status in June 2013. Surgical procedure We used Bier block for anesthesia, made a 2- to 3-cm straight incision in the existing dorsal surgical scar, and approached the dorsal wrist capsule between the third and fourth extensor compartments. Through windows in the capsule we collected samples from the soft tissue surrounding the implant for bacteriological cultures. From the dorsal interphase area between the radial component and the radius and from the interphase area between the carpal plate and the carpus, we collected tissue samples for histopathological examination. In one patient we also collected tissue under an ulnar head component; but to avoid a potential confounding influence, we did not include this in the analyses aimed at testing our hypothesis. We closed the wound with resorbable sutures in the capsule and nonresorbable sutures in the skin. Patients were allowed to mobilize the wrist without delay. Histopathological examination After fixation in 10% buffered formaldehyde all tissue samples were sectioned and embedded in paraffin. Sections cut at 2 mm thickness were prepared, stained with hematoxylineeosin, and examined by light and polarized microscopy. The amount of foreign body particles was graded semi-quantitatively from 0 to 3, in which 0 represented no particles; 1, particles present but hard to find; 2, no problem in identifying particles; and 3, a marked amount of particles as seen on Vol. 39, December 2014 2398 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY high-field magnification. Two pathologists (AT and MBa) blinded to the study protocol, who had experience in examining implantebone interphases, reviewed the biopsies independently; after a general common discussion, they performed an independent second look examination. The reliability (ie, agreement between the 2 investigators) was assessed. Radiology According to our protocol for TWA, plain radiographs were obtained within 6 weeks after the index operation, then 6 months later, and annually thereafter. If the last of these radiographs were older than 3 months, new radiographs were obtained in view of the present study. Two senior hand surgeons (MBo and LSV), who were blinded with respect to the clinical and the histological findings, examined the radiographs independently. On all serial posteroanterior radiographs, we measured the width of the radiolucent area (if present) at selected spots (Fig. 1) and calculated the mean of the width at spots 1/2/3, 4/5, 6/7/8, and 9/10 (expressed in millimeters). We correlated these mean values with the histopathological, clinical, and serological findings. Furthermore, we established the evolution of radiolucency in function of time in the individual patients. To evaluate angulation and subsidence, we measured the angle between the radial component and the radial diaphysis and the angle between the carpal component and the third metacarpal. We also measured the distance from the tip of the radial component to the tip of the radial styloid and the distance from the tip of the central carpal peg to the third carpometacarpal joint on all radiographs. The digitalized measurement systems were provided by Sectra’s IDS5/web (Sectra AB, Linköbing, Sweden). We considered a progressive and consistent change of distances from the first postoperative to the latest radiograph of 3 mm or greater as indicating subsidence and a corresponding change of angulation of 5 or greater as indicating tilting of the implants.14 The inter-observer reliability of the measurements was also calculated. Bacteriology Bacteriological examination of the samples included direct microscopy and aerobic as well as anaerobic cultures. Blood analyses We determined C-reactive protein values and white blood cell count to evaluate possible ongoing infection. We also measured the concentration of Cr and Co in whole blood according to the EPA J Hand Surg Am. r FIGURE 1: Spots for measurement of the width of radiolucency on serial posteroanterior radiographs. In this example, a small radiolucent area is visible at spot 4 (maximal width, 1.4 mm). 200.7þ8-ICP/AES/SFMS method (Swedish Board for Accreditation and Conformity Assessment, Borås, Sweden), expressed as micrograms per liter. Clinical examination Patients expressed the general level of wrist pain on a visual analog scale (0e100) with 0 indicating no pain and 100 indicating maximal pain. We recorded grip strength in kilograms and used the Quicke Disabilities of the Arm, Shoulder, and Hand questionnaire as a validated outcomes measure. Statistics For correlations of values on interval scales, we used Pearson correlation coefficient and for values on ordinal scales, Spearman rho correlation coefficient. To evaluate the reliability of the radiological measurements, we used Pearson correlation coefficient and the intra-class coefficient (ICC3, single, fixed raters).15 We considered correlation coefficients between 0.8 and 1.0 to indicate a very strong correlation, between 0.6 and 0.79 a strong correlation, between 0.4 and 0.59 a moderate correlation, between 0.2 and 0.39 a weak correlation, and between 0.0 and 0.19 a very weak or absent correlation. To evaluate the histopathological findings, we used Cohen kappa, in which values less than 0.40 indicated poor agreement, 0.40 to 0.75 fair Vol. 39, December 2014 2399 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY TABLE 2. Interobserver Reliability of Measurements on Serial Radiographs Measurements per Observer, n Pearson Correlation Coefficient Intra-class Coefficient Width of radiolucent zone at all spots (IeX) 820 0.85 0.85 Width of radiolucent zone at spots 4 and 5 164 0.81 0.81 Width of radiolucent zone at spots 9 and 10 164 0.81 0.80 Tilt of radial component 78 0.96 0.96 Subsidence of radial component 78 0.90 0.89 Tilt of carpal component 78 0.87 0.87 Subsidence of carpal component 78 0.98 0.98 FIGURE 2: Evolution of radiolucency. Each graph represents an individual patient. A Mean width at zones 4 and 5. B Mean of width at zones 9 and 10. to good agreement, and greater than 0.75 excellent agreement. We calculated that the required sample size to reveal strong correlations (r ¼ 0.7) was 11 with a power of 0.8 and a ¼ .05. RESULTS Complications There were no complications related to harvesting of biopsies in terms of infection, pain, or deterioration of J Hand Surg Am. r function. Surgical wounds healed uneventfully within 2 weeks in all patients. Radiology Reliability of the measurements was very strong (Table 2), and we used the measurements of the senior author (MBo) for further analyses. Radiolucency was not seen in zones 1 to 3 and only in 2 patients in zones 6 to 8 (0.3 and 0.4 mm, respectively). Some degree of radiolucency was seen in 10 patients in Vol. 39, December 2014 2400 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY FIGURE 3: Radiographs in a patient undergoing total wrist arthroplasty. A Two weeks after surgery. The peg penetrates the third metacarpal, which does not comply with usual recommendations but resulted from an unusually large carpal resection. B Four years after the operation. A large area of periprosthetic osteolysis has developed under the radial component. The mean width of radiolucency was 8.5 mm at spots 4 and 5. No radiolucency at spots 1, 2, or 3. Osteolysis is also present under the carpal plate and around the screws and central peg. The carpal component has not subsided since surgery. C Computed tomography scan. The radiolucent lines seen at zone 2 and 3are artifacts caused by the imaging software. Bone condensation is present at the tip of the radial component where load is transmitted maximally from implant to bone. TABLE 3. Reliability of Histological Findings (Agreement Between 2 Pathologists) Findings Necrotic tissue k 0.68 Metal particles 0.59 Polyethylene debris 0.78 Preponderance of macrophages compared with lymphocytes 1.00 Foreign body reaction 0.74 zone 4 to 5 (Fig. 2). In 6 of these, the width remained less than 2 mm throughout the observation period. In 3 patients it increased initially to between 3 and 4 mm and then stabilized. In one patient it increased rapidly but seemed to stabilize between 8 and 9 mm after 4 years (Fig. 3). In zones 9 to 10 radiolucency was seen in 7 patients (Fig. 2). In 4 of these the width remained less than 1 mm. In 3 patients it increased to between 3 and 4 mm. There was no evidence of radial component loosening in any patient. In 3 patients subsidence of the carpal component was evident. None of the cemented components had subsided. Histopathology We harvested 13 samples at the radial component, 10 at the carpal component, and 1 at a metallic ulnar head implant. Table 3 shows the interobserver agreement of the histological findings. Foreign body giant cell J Hand Surg Am. r reaction was a common finding, encountered by at least one of the pathologists in 15 of the 24 specimens. Macrophages were predominant compared with lymphocytes in 22 specimens. Necrotic tissue was seen in 17. Polyethylene debris was detected in 17 specimens by both investigators and in another 2 specimens by at least one investigator (Fig. 4). In 11 of these, the polyethylene particles were sparse and small or minute. No marked amount of particles was encountered in any case. In 5 cases no polyethylene was identified by either of the investigators (Fig. 4). The amount of polyethylene at the radial component correlated very weakly or not at all with the width of radiolucency according to both pathologists (Spearman r, e0.16 and 0.18, respectively) (Fig. 5). On the carpal side, the correlation was negative (Spearman r, e0.55 and -0.69 respectively) (Fig. 6). The same applied to the metallic particles (Fig. 4): Spearman r ¼ e0.26 and 0.12, respectively, on the radial side and e0.18 and e0.26, respectively, on the carpal side. Blood analyses Mean blood level of Cr was 0.264 mg/L (SD, 0.384) and of Co 0.253 mg/L (SD, 0.275). There was no correlation between the blood level of Cr and the width of the radiolucent zones 4 to 5 and 9 to 10 and a reversed weak or moderate correlation for the blood level of Co. White blood cell count was normal in all patients, and the C-reactive protein level was normal in all but one patient. Vol. 39, December 2014 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY 2401 FIGURE 4: Examples of histology. A Polarized light microscopy (x200 magnification). Polyethylene fragments engulfed by multinucleated foreign body giant cells (arrows), semi-quantitatively estimated as 2 on a scale of 0 to 3 for the amount of foreign body particles. B Polarized light microscopy ( 100 magnification). No polyethylene fragments or particles could be demonstrated in this specimen. C Hematoxylineeosin staining ( 200 magnification). Only sparse metal particles were demonstrable (arrows). Bacteriology All samples were negative with respect to direct microscopy and culture for bacteria. Clinical findings QuickeDisabilities of the Arm, Shoulder, and Hand and the visual analog scale scores and grip strength did not correlate with radiolucency (all correlation coefficients lower than 0.10). DISCUSSION Periprosthetic osteolysis has been reported frequently after TWA.16 In a series of Biaxial implants (DePuy Orthopedics, Inc., Warsaw, IN), a periprosthetic radiolucent zone of at least 2 mm was found in 12 of 32 cases (mean follow-up, 6 y).8 In a Re-motion series, periprosthetic radiolucency more than 2 mm in width was found in 16 of 44 cases on the radial side and in 7 on the carpal side.17 In a series of cemented Universal I TWA (KMI Inc., San Diego, CA) in rheumatoid patients, 9 of 19 patients seen at followup of more than 5 years after the operation had received revisions because of loosening of the carpal component.12 Among the remaining ten, 3 had radiographic subsidence and/or osteolysis. The Biaxial, Re-motion, and Universal TWA are metal-on-polyethylene implants but similar PPO has also been demonstrated in J Hand Surg Am. r metal-on-metal TWA18 and even in metallic single component implants such as ulnar head replacement devices.19 The histology of PPO has been investigated in other joints. Kepler et al20 studied 52 patients who underwent revision total shoulder arthroplasty at a mean of 4.5 years after the index surgery. Ten patients (19%) had radiographic evidence of osteolysis at the glenoid component. Histological specimens taken at the time of revision surgery demonstrated no significant differences between patients with or without osteolysis with respect to the presence of metallic, polyethylene, or cement debris particles or with the presence of inflammatory reactions. Dalat et al21 revised 25 total ankle arthroplasties. Radiographically, all patients showed tibial and talar osteolytic lesions, and in 25% the implant had collapsed into the osteolytic cysts. Histological examination of the biopsies showed granulomatous response associated with a foreign body giant cell reaction in all cases. The cysts contained necrotic material. Implant material, primarily polyethylene, was identified in 95% of the specimens and metallic debris in 60% of patients. Generally, it has been hypothesized that the macrophage phagocytosis of particulate debris from component abrasive and adhesive wear activates the macrophages and other inflammatory cells with Vol. 39, December 2014 2402 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY FIGURE 5: Scatterplot showing the width of radiolucency in zones 4 and 5 versus the amount of polyethylene fragments in the samples taken at the interphase between the radial component and the radius: A According to pathologist AT. B According to pathologist MBa. FIGURE 6: Scatterplot showing the width of radiolucency in zones 9 and 10 versus the amount of polyethylene fragments in the samples taken at the interphase between the carpal component and the carpal: A According to pathologist AT. B According to pathologist MBa. cytokine release that in turn activate the osteoclasts, but other possible mechanisms have been proposed. According to Skoglund and Aspenberg,22 the much less studied osteolytic effects of pressure could be far more important, and stress shielding is also considered a potent stimulator of bone resorption.19,23,24 The main strength of our study is that it investigated a consecutive group of patients with TWA, regardless of their clinical or radiological status, and that we followed these patients prospectively with annual clinical and radiographical examinations. Another strength of this study was that 2 pathologists investigated all specimens independently and in a blinded manner. Our results confirm that the histopathological findings may be subject to differences of interpretation and interobserver variation that deserve consideration and discussion. Thus, the relative disagreement between the 2 pathologists concerning the presence of metallic particles may be because in several cases the metallic particles were minute and sparse and on occasion could be confused with corrosion products. Generally, however, interobserver agreement was good to excellent. J Hand Surg Am. r Vol. 39, December 2014 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY The hypothesis in the current study was that the presence and severity of PPO correlated with the presence and degree of polyethylene and metallic debris. We showed that this was not the case. Moreover, foreign body giant cell reaction was seen as frequently in patients with no or minimal PPO as in those with pronounced PPO. The patient with the most marked osteolytic lesion at the radial component (Fig. 3) had no detectable polyethylene debris in the collected specimen at all according to one pathologist and only minimal amounts according to the other. Only one of the pathologists considered a foreign body giant cell reaction to be present in this specimen, whereas both pathologists considered the presence of metallic particles minimal or very small. In most cases PPO was associated with a low amount of metallic debris. Also, metallic wear did not cause elevated levels of metallic ions in the blood samples. The values were far below the proposed acceptable upper limits of 2.56 mg/L for Cr and 2.02 mg/L for Co in whole blood, based on the studies by Hart et al.25 According to Trace Elements LaboratoryeLondon Health Sciences Centre, the reference values for Cr in whole blood is 0.40 to 1.60 mg/L and for Co, 0.032 to 0.290 mg/L . The only patient with a Co value exceeding this reference had a bilateral TWA and a bilateral total knee arthroplasty. In a systematic study of the literature concerning Cr and Co ion concentrations in blood and serum after various types of metal-on-metal hip arthroplasties, Jantzen et al26 found that the average Cr concentration ranged between 0.5 and 2.5 mg/L in blood. For Co, the range was 0.7 to 3.4 mg/L. Our series was underpowered because of the small number of cases; conversely, however, it represents a broad spectrum of histopathological findings (amounts of debris) as well as radiological findings (width of radiolucency) and the lack of correlations was unequivocal. Moreover, the sample size was reasonable according to our calculations. Our evaluation of the osteolytic areas may not represent the volume of bone resorption correctly because we used a 2-dimensional surrogate for a 3-dimensional space. Nevertheless, our method was highly reproducible and corresponded to the method described by Cobb et al14 and Takwale et al.10 None of the radial components collapsed into the osteolytic area, which consequently was intact for evaluation. The PPO tended to level out in time and rarely caused gross loosening of the components. In light of the lack of correlation between particulate debris and PPO and the absence of rheumatoid or infectious activity, we suggest that the PPO we describe can be J Hand Surg Am. r 2403 at least partially attributed to stress shielding of the bony structures by the implants. The fact that bone resorption occurred at the edges of the components nearest to the joint, where load is transmitted through the implant components, is consistent with this hypothesis. There is a need for further investigation, however, including radiostereographical methods and serial focal bone mineral density measurements. For the time being, we recommend close and continued observation of patients with marked asymptomatic PPO. Bisphosphonates, denosumab, strontium, ranelate, and parathyroid hormone have been reported as possible treatment agents with regard to maintaining more periprosthetic bone mineral density, but clinical documentation is limited.27 We find that there is currently no need to change conventional polyethylene in the Re-motion implant to the more resistant highly cross-linked polyethylene because the occurrence of polyethylene debris was low. REFERENCES 1. Zhu YH, Chiu KY, Tang WM. Review article: polyethylene wear and osteolysis in total hip arthroplasty. J Orthop Surg. 2001;9(1):91e99. 2. Orishimo KF, Claus AM, Sychterz CJ, Engh CA. Relationship between polyethylene wear and osteolysis in hips with a secondgeneration porous-coated cementless cup after seven years of followup. J Bone Joint Surg Am. 2003;85(6):1095e1099. 3. Goosen JHM, Castelein RM, Verheyen CCPM. Silent osteolysis associated with an uncemented acetabular component: a monitoring and treatment algorithm. Curr Orthop. 2005;19:288e293. 4. Brodner W, Bitzan P, Meisinger V, Kaider A, Gottsauner-Wolf F, Kotz R. Elevated serum cobalt with metal-on-metal articulating surfaces. J Bone Joint Surg Br. 1997;79(2):316e321. 5. Smolders JM, Hol A, Rijnberg WJ, van Susante JL. Metal ion levels and functional results after either resurfacing hip arthroplasty or conventional metal-on-metal hip arthroplasty. Acta Orthop. 2011;82(5):559e566. 6. Fabi D, Levine B, Paprosky W, et al. Metal-on-metal total hip arthroplasty: causes and high incidence of early failure. Orthopedics. 2012;35(7):e1009ee1016. 7. Hasegawa M, Yoshida K, Wakabayashi H, Sudo A. Cobalt and chromium ion release after large-diameter metal-on-metal total hip arthroplasty. J Arthroplasty. 2012;27(6):990e996. 8. Harlingen Dv, Heesterbeek PJ, J de Vos M. High rate of complications and radiographic loosening of the biaxial total wrist arthroplasty in rheumatoid arthritis: 32 wrists followed for 6 (5-8) years. Acta Orthop. 2011;82(6):721e726. 9. Rizzo M, Beckenbaugh RD. Results of biaxial total wrist arthroplasty with a modified (long) metacarpal stem. J Hand Surg Am. 2003;28(4):577e584. 10. Takwale VJ, Nuttall D, Trail IA, Stanley JK. Biaxial total wrist replacement in patients with rheumatoid arthritis: clinical review, survivorship and radiological analysis. J Bone Joint Surg Br. 2002;84(5):692e699. 11. Ferreres A, Lluch A, Del Valle M. Universal total wrist arthroplasty: midterm follow-up study. J Hand Surg Am. 2011;36(6): 967e973. 12. Ward CM, Kuhl T, Adams BD. Five to ten-year outcomes of the Universal total wrist arthroplasty in patients with rheumatoid arthritis. J Bone Joint Surg Am. 2011;93(10):914e919. Vol. 39, December 2014 2404 WEAR PARTICLES AND OSTEOLYSIS AFTER TOTAL WRIST ARTHROPLASTY 13. Boeckstyns ME, Herzberg G, Merser S. Favorable results after total wrist arthroplasty: 65 wrists in 60 patients followed for 5-9 years. Acta Orthop. 2013;84(4):415e419. 14. Cobb TK, Beckenbaugh RD. Biaxial total-wrist arthroplasty. J Hand Surg Am. 1996;21(6):1011e1021. 15. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86(2):420e428. 16. Boeckstyns MEH. Wrist arthroplasty—a systematic review. Dan Med J. 2014;61:A4834. 17. Boeckstyns MEH, Herzberg G. Periprosthetic osteolysis after total wrist arthroplasty. J Wrist Surg. 2014;3(2):101e106. 18. Reigstad O, Lutken T, Grimsgaard C, Bolstad B, Thorkildsen R, Rokkum M. Promising one- to six-year results with the Motec wrist arthroplasty in patients with post-traumatic osteoarthritis. J Bone Joint Surg Br. 2012;94(11):1540e1545. 19. Herzberg G. Periprosthetic bone resorption and sigmoid notch erosion around ulnar head implants: a concern? Hand Clin. 2010;26(4):573e577. 20. Kepler CK, Nho SJ, Bansal M, et al. Radiographic and histopathologic analysis of osteolysis after total shoulder arthroplasty. J Shoulder Elbow Surg. 2010;19(4):588e595. 21. Dalat F, Barnoud R, Fessy MH, Besse JL, French Association of Foot Surgery AFCP. Histologic study of periprosthetic osteolytic lesions J Hand Surg Am. r 22. 23. 24. 25. 26. 27. after AES total ankle replacement: a 22 case series. Orthop Traumatol Surg Res. 2013;99(6 suppl):S285eS295. Skoglund B, Aspenberg P. PMMA particles and pressure—a study of the osteolytic properties of two agents proposed to cause prosthetic loosening. Orthop Res. 2003;21(2):196e201. Huiskes R, Weinans H, van Rietbergen B. The relationship between stress shielding and bone resorption around total hip stems and the effects of flexible materials. Clin Orthop Relat Res. 1992;274:124e134. Taylor AF, Saunders MM, Shingle DL, Cimbala JM, Zhou Z, Donahue HJ. Mechanically stimulated osteocytes regulate osteoblastic activity via gap junctions. Am J Physiol. 2007;292(1): C545eC552. Hart AJ, Skinner JA, Winship P, et al. Circulating levels of cobalt and chromium from metal-on-metal hip replacement are associated with CD8þ T-cell lymphopenia. J Bone Joint Surg Br. 2009;91(6): 835e842. Jantzen C, Jorgensen HL, Duus BR, Sporring SL, Lauritzen JB. Chromium and cobalt ion concentrations in blood and serum following various types of metal-on-metal hip arthroplasties: a literature overview. Acta Orthop. 2013;84(3):229e236. Albanese CV, Faletti C. Imaging of Prosthetic Joints: A Combined Radiological and Clinical Perspective. Milan: Springer; 2014: 151e157. Vol. 39, December 2014